16-UJP-15515-RS - universal journals publication
advertisement

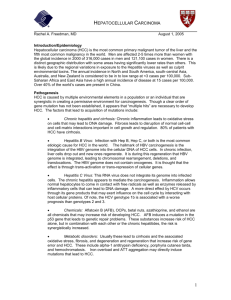
Mona Talaat Kamel et al. UJP 2015, 04 (03): Page 92-97 Universal Journal of Pharmacy www.ujponline.com Research Article ISSN 2320-303X Take Research to New Heights DETECTION OF SOME TUMOR MARKERS IN PATIENTS WITH LIVER CIRRHOSIS AND HEPATOCELLULAR CARCINOMA RELATED TO HEPATITIS C VIRUS Ola Sayed Mohammed1, Omnia Azat Ali2, Mona Talaat Kamel1, Hassan Shalaby3, Khadega K. El Gohary4, Seham Mahmoud5, Amal El Shimy6 1 Department of Biochemistry, Faculty of Pharmacy, Al-Azhar University, Cairo, Egypt Department of Biochemistry, Faculty of Pharmacy, Egyptian Russian University, Cairo, Egypt 3 Department of Internal Medicine, Misr University for Science and technology, Egypt 4 Department of Biochemistry, El Sahel Teaching Hospital, Egypt 5 Department of Tropical, El Sahel Teaching Hospital, Egypt 6 Department of Microbiology and Immunology, Faculty of Medicine, Cairo University, Egypt 2 Received 30-04-2015; Revised 28-05-2015; Accepted 26-06-2015 ABSTRACT Hepatocellular carcinoma is the fifth most common cancer worldwide and the most common form of liver cancer, being responsible for 80% of the primary malignant liver tumors in adults. Early detection of the disease is thus an important goal allowing the patient to be treated before the enlargement of the tumor or its metastasis to distant organs. The first serologic assay for detection and clinical follow up of patients with hepatocellular carcinoma was alphafetoprotein (AFP) which has been the standard tumor biomarker for Hepatocellular Carcinoma for many years. Further studies showed the relationship between highly concentration of some biochemical parameters and the presence of Hepatocellulr Carcinoma as Cerulplasmin, Des -gamma –Carboxy Prothrombin, Ferritin and iron for early diagnosis of HCC. Aim: To detect the level of some tumor markers as Alpha-fetoprotein, Cerulplasmin, Des -gamma –Carboxy Prothrombin, Ferritin and Iron in sera of patients suffering from cirrhosis & HCC and comparing which one is more sensitive and specific for early diagnosis of HCC. Methods: This study was conducted on a total number of 150 patients admitted at El Sahel Teaching Hospital and Department of Internal Medicine, Misr University for Science and technology. The patients of this study were subdivided as follows: 50 apparently healthy individuals control, 50 patients with chronic hepatitis C (genotype 4) and developed to cirrhosis and the other 50 patients as HCC group related to Hepatitis C virus (HCV). Complete examination was carried out for each individual to confirm diagnosis. Individuals, sera were subjected to quantitative determination of alpha-fetoprotein (AFP), Ceruoplasmin, Des -gamma -Carboxyprothrombin (DCP), Ferritin, iron and other biochemical parameters. Results: Using the best cut-off value of Ferritin (258.5 ng/mL) showed sensitivity and specificity of 86% and 78% respectively , Iron cut-off value (210.5 μg/dL)showed a sensitivity and specificity of 86% and 61% respectively, Ceruloplasmin cut-off value (322.5 ng/ml) showed a sensitivity and specificity of 68 % and 71% respectively , DCP cutoff value (4.15 ng/ml) showed a sensitivity and specificity of 80% and 35% respectively , while cut-off value of AFP (17 μg/L ) showed a sensitivity and specificity of 70 % and 61% respectively. Conclusion: Ferritin was proved to be superior to Alpha-fetoprotein, Ceruloplasmin , Des -gamma -Carboxyprothrombin and Iron for early detection of HCC patients being highly sensitive and specific. Keywords: Alpha fetoprotein –Ceruoplasmin -DCP– Ferritin-Hepatocellular carcinoma-HCV. INTRODUCTION Hepatocellular carcinoma is the fifth most common cancer worldwide and the most common form of liver *Corresponding author: Mona Talaat Kamel Department of Biochemistry, Faculty of Pharmacy, Al-Azhar University, Cairo, Egypt, Address: Faculty of Pharmacy (Girls), Al-Azhar University, Nasr City, Cairo, Egypt. Telephone: +226066606, Mobile: +201117832406 cancer, being responsible for 80% of the primary malignant liver tumors in adults. The 5-year relative survival rate is about 7% and causes more than 600000 deaths annually worldwide1. Hepatocellular carcinoma rarely occurs before the age of 40 years and reaches a peak at approximately 70 years of age. Rates of liver cancer among men are two to four times as high as the rates among women. Risk factors for hepatocellular carcinoma include infection with HBV or HCV, alcoholic Universal Journal of Pharmacy, 04(03), May-June 2015 92 Mona Talaat Kamel et al. UJP 2015, 04 (03): Page 92-97 liver disease, and most probably nonalcoholic fatty liver disease. Less common causes include hereditary hemochromatosis, alpha1-antitrypsin deficiency, autoimmune hepatitis, some porphyrias, and Wilson’s disease. The distribution of these risk factors among patients with hepatocellular carcinoma is highly variable, depending on geographic region and race or ethnic group. Most of these risk factors lead to the formation and progression of cirrhosis, which is present in 80 to 90% of patients with hepatocellular carcinoma2. The estimated risk of hepatocellular carcinoma is 15 to 20 times as high among persons infected with HCV as it is among those who are not infected, with most of the excess risk limited to those with advanced hepatic fibrosis or cirrhosis 3. Egypt has the highest prevalence of HCV worldwide and has rising rates of hepatocellular carcinoma (HCC). Egypt's unique nature of liver disease presents questions regarding the distribution of HBV and HCV in the etiology of HCC 4. Early detection of the disease is thus an important goal allowing the patient to be treated before the enlargement of the tumor or its metastasis to distant organs. Serum tumor markers may be useful in predicting the tumor at early stages 5.The first serologic assay for detection and clinical follow up of patients with hepatocellular carcinoma was alphafetoprotein (AFP) which has been the standard tumor biomarker for HCC for many years 6.Although detection of AFP level is easy and less expensive, but it shows less sensitivity7. Serum ferritin concentration is a marker of varied pathophysiological events and is elevated with increased liver iron concentration, hepatic necroinflammation, and systemic illness, all of which may cause a deterioration in liver function and clinical status8. A study suggested a potential association of increased hepatic iron deposition with more advanced hepatic fibrosis in patients with chronic hepatitis C virus infection. The serum ferritin value, an independent predictor of severe hepatic fibrosis in patients with chronic hepatitis C virus infection, may predict hepatic iron deposition and severity of fibrosis9. The Cu/Zn ratio was found to be significantly higher in patients with HCC compared with that in age and sexmatched controls, with a sensitivity of 87.5%, this ratio might be useful in the evaluation of suspected hepatocellular malignancy10. Liebman, et al11., first reported that 67% of patients with HCC had abnormally elevated levels of des- γ –Carboxy Prothrombin (DCP), also known as the protein induced by vitamin K absence or antagonist II (PIVKA-II). So in this study we try to compare the sensitivity of different marker as AFP, Ceruloplasmin, DCP, Ferritin and Iron in HCC early detection. PATIENTS AND METHODS This case control study was conducted on total numbers 150, subdivided as follows: 50 apparently healthy www.ujponline.com individuals as control, 50 patients with chronic hepatitis C (genotype 4) proven by Polymerase Chain Reaction (PCR) and 50 patients as HCC group proven by PCR for chronic hepatitis C and using Computed Tomograghy (CT) for proven of Hepatocellular Carcinoma cases. An informed consent was taken from each patient before the beginning of the study. The Ethical Committee of El Sahel Teaching Hospital approved the study protocol, which was prepared in accordance with the ethical guidelines of the 1975 Declaration of Helsinki and later revisions. On admission to the hospital during the study period, every patient fulfilling the inclusion criteria is allocated to one intervention group and informed written consent for the study was obtained from all patients. The inclusion criteria of HCV- Cirrhotic cases were: adult male or female (30–73 years old) with proven genotype 4 chronic hepatitis C, positive serum HCV RNA by quantitative polymerase chain reaction (PCR) and developed to cirrhosis. Those with HCC proved by liver biopsy were allocated to GIII. Besides the necessary investigations needed to fulfill the selection criteria all individuals included in this study were subjected to the following: Full history was taken with special reference to risk factors for HCV infection: as previous exposure to HCV in surgical wards, blood transfusions, dental clinics, needle stick injury, history of HCV in the spouse and i.v. injection. 2. Serum samples Ten ml of venous blood were withdrawn from each patient in dry sterile vacutainers. After centrifugation, the serum was tested for: a- liver function tests: which included serum aminotransferases (AST), (ALT) and total bilirubin (Beckman Synchron systems; Galway, Ireland).b- Quantitative determination of serum alpha fetoprotein (AFP) level by using Monobind INC. kit USA. c- Quantitation of HCV-RNA using Real Time polymerase chain reaction (RT-PCR) (Strata gene) was done after RNA Extraction (by Viral RNA Extraction Kit, QiagenGermany). d-ELISA for HBcAb and HBsAg was done for all cases to exclude presence of hepatitis B viral etiology of liver disease. e-Quantitative Colorimetric Determination of Iron by Stanbio procedure (USA). fDetection of Ferritin by DRG® Ferritin (EIA1872)ELISA(USA).h-Detection of Human Ceruloplasmin and Des-γ-Carboxy Prothrombin by EIAab ELISA kit. Statistical methods Data management and statistical analysis were performed using Statistical Package for Social Sciences (SPSS) vs. 21.Numerical data were summarized using means and standard deviations or medians and ranges. Categorical data were summarized as percentages. Comparisons between the 3 groups with respect to normally distributed Univariate ANOVA and Bonferroni post hoc test numeric. For categorical variables, differences were analyzed with 2(chi square) tests. Correlations among different study parameters were Universal Journal of Pharmacy, 04(03), May-June 2015 93 Mona Talaat Kamel et al. UJP 2015, 04 (03): Page 92-97 determined by using Pearson’s test. Receiver Operator Curve (ROC curve) was done to determine the cut off value of different markers in diagnosis of HCC. All pvalues are two-sided. P-values < 0.05 were considered significant. RESULTS Baseline characteristics The mean age of the studied control group was 32.8. Patients in GII with a mean age of 52.6, while GIII with a mean age 58.8. Sex distribution in GI was 12 (60%) females and 8 (40%) males, in GII number of females was 12 (48%) and number of males was 13(52%),while in GIII, there were 7(28%) females and 18(72%) males. There was no statistically significant difference between the three groups as regards the distribution of sex (Table 1). Results of laboratory investigation We found a significant difference of AST, ALT, T.Bil., D.Bil., Glucose, PT, Creatinine, Albumin, INR, WBCs and GGT levels in HCC and cirrhotic patients groups compared to healthy control ( P< 0.001). Also, There was a significant difference between HCC group compared to cirrhotic group AST, ALT, T.Bili., INR, Glucose, Albumin, PT, WBCs and GGT( P< 0.001) .There www.ujponline.com was a higher mean level of AFP , Iron, Ferritin, Ceruloplasmin and DCP among cases with HCC compared to cirrhosis and control groups with highly statistically significant difference( P< 0.001) (Table 2). No statistical difference between HCC and Cirrhosis was found regarding weight loss, elevation of Temperature, Abdominal pain and Jaundice, while regarding to Encephalopathy and Bleeding showed highly statistical significant difference between the two groups. (Fig .1) & Table (3): showed the comparison between the five parameters regarding to the ROC curve and the area under the curve. The present study reveals that the Ferritin was the best tumor with cut off (258.5 ng/mL) showed sensitivity and specificity of 86% and 78% respectively , Iron cutoff value (210.5 μg/dL) showed a sensitivity and specificity of 86% and 61% respectively , Ceruloplasmin cut-off value (322.5 ng/ml) showed a sensitivity and specificity of 68 % and 71% respectively , DCP cut-off value (4.15 ng/ml) showed a sensitivity and specificity of 80% and 35% respectively , while cut-off value of AFP (17 μg/L ) showed a sensitivity and specificity of 70 % and 61% respectively. Table 1: Comparison regarding clinical Characteristics between all studied groups Control Cirrhosis HCC Factors n=50(%) n=50(%) n=50(%) P value Mean ±SD Age (yrs.) 32.8±8.1 52.6±9.8 58.8±9.6 <0.001 Gender Male 23(46.0) 24(48.0) 31(62.0) 0.218 Female 27(54.0) 26(52.0) 19(38.0) Abdominal pain 3(6.0) 23(46.0) 25(50.0) <0.001 Encephalopathy 0 10(20.0) 24(48.0) <0.001 Bleeding 0 21(42.0) 23(46.0) <0.001 Elevated BT 3(6.0) 15(30.0) 21(42.0) <0.001 BT: Body Temperature., P-values < 0.05 were considered significant. Table 2: Comparison regarding laboratory investigations of all studied groups Control Cirrhosis HCC n=50(%) n=50(%) n=50(%) P value PT 11.5±0.6 12.4±1.9 14.1±1.3 <0.001 INR 1.0±0.1 1.0±0.2 1.2±0.1 <0.001 ALT 29.6±5.8 57.3±16.5 64.3±18.9 <0.001 AST 32.2±8.9 61.2±36.3 149.7±66.2 <0.001 T.Bil 0.7±0.2 1.3±0.7 2.7±1.0 <0.001 D.Bil 0.1±0.1 0.3±0.2 0.8±0.4 <0.001 Glucose 101.2±13.0 167.9±35.8 217.7±166.1 <0.001 Creatinine 0.9±0.1 1.8±0.5 1.8±0.6 <0.001 Alb 3.9±0.2 3.5±0.5 2.7±0.6 <0.001 GGT 287.8±85.0 182.9±53.9 122.3±28.3 <0.001 Hb 11.9±1.7 11.1±1.1 11.0±1.1 0.003 WBCs 6900.0±2290.3 5204.6±1684.6 5204.6±1684.6 <0.001 Iron 175.3±38.3 221.4±54.0 259.7±55.4 <0.001 Universal Journal of Pharmacy, 04(03), May-June 2015 94 Mona Talaat Kamel et al. UJP 2015, 04 (03): Page 92-97 Ferritin Ceruloplasmin DCP AFP 175.8±98.0 186.4±99.3 12.1±20.9 14.9±24.7 240.2±68.5 299.8±95.2 26.8±14.5 35.9±30.1 www.ujponline.com 338.4±97.0 403.1±159.2 36.0±33.4 306.8±281.5 <0.001 <0.001 <0.001 <0.001 PT: Prothrombin Time, INR: International Normalized Ratio, AST: Aspartate transaminase, ALT: Alanine transaminase, T.Bil: Total Bilirubin, D.Bil: Direct Bilirubin , GGT :gamma-glutamyltransferase, Hb :Hemoglobin ,WBCs: White Blood Cells, DCP: Des -gamma -carboxyprothrombin , AFP :alpha-fetoprotein,P-values < 0.05 were considered significant.. Table 3: Comparison between the different biochemical markers regarding Area under curve, Sensitivity and Specificity Area under curve P- value Cut off Sensitivity % Specificity % AFP 0.778 <0.001 17 70% 61% Iron 0.804 <0.001 210.5 86% 61% Ferritin 0.855 <0.001 258.5 86% 78% Ceruloplasmin 0.771 <0.001 322.5 68% 71% DCP 0.66 0.001 4.15 80% 35% AFP: alpha-fetoprotein, DCP: Des -gamma –carboxyprothrombin,P-values < 0.05 were considered significant. Figure1: ROC curve of AFP, Ceruloplasmin, DCP, Ferritin and Iron DISCUSSION Primary liver cancer is one of the most common and deadly malignant neoplasms worldwide. The incidence and mortality rates for hepatocellular carcinoma (HCC) are virtually identical, reflecting the poor overall survival of patients with this kind of tumor12. The management of patients at risk for developing HCC remains challenging. Increased understanding of cancer biology and technological advances have enabled identification of a multitude of pathological, genetic, and molecular events that drive hepatocarcinogenesis leading to discovery of numerous potential biomarkers in this disease. They are currently being aggressively evaluated to establish their value in early diagnosis, optimization of therapy, reducing the emergence of new tumors, and preventing the recurrence after surgical resection or liver transplantation. These markers not only help in prediction of prognosis or recurrence but may also assist in deciding appropriate modality of therapy and may represent novel potential targets for therapeutic interventions13. Detection of HCC at early stages is critical for good clinical outcome as the prognosis of HCC patients is very poor when diagnosed at late stages14. Although serum AFP is the most established tumor marker in HCC and considered as the golden standard to which other markers are compared, it was found to be normal in about 30% of the patients, especially in early stages14. In this study AFP showed sensitivity and specificity of 70 % and 61% respectively at Cut off (17 μg/L). Iron excess was mainly located within reticuloendothelial cells, and this is the main argument in favour of the role of iron deposits in hepatic carcinogenesis. Iron plays a role in HCC development in chronic liver diseases associated with minor iron overload/siderosis15.Regading to this study Iron showed high Area under curve of (0.804), sensitivity reach to 86 % and specificity of 61 % at Universal Journal of Pharmacy, 04(03), May-June 2015 95 Mona Talaat Kamel et al. UJP 2015, 04 (03): Page 92-97 Cut off (210.5 μg/dL). Other studies reported that liver iron deposition was more frequent and more important in viral C cirrhotic patients with HCC than in HCC free controls. Liver iron overload seems to contribute to the development of HCC in patients with viral C cirrhosis. Patients with viral C cirrhosis that histological liver iron deposits were more frequent and more important in patients who had developed HCC compared with controls without HCC15. So further prospective studies are needed to confirm the hypothesis that iron deficiency protects against HCC in chronic liver disease CLD. Serum Ferritin concentration is a marker of varied pathophysiological events and is elevated with increased liver iron concentration, hepatic necroinflammation, and systemic illness, all of which may cause a deterioration in liver function and clinical status. Serum Ferritin concentration (SF) is a widely available and easily measured biochemical parameter. SF is increased in patients with elevated body iron stores, hepatic necroinflammatory activity, and systemic inflammatory states. These causes of increased SF may be associated with an increased risk of clinical deterioration and progressive liver dysfunction8.Our results showed Ferritin had increased levels in both cirrhotic and HCC groups at Cut off (258.5ng/mL) with high sensitivity (86%) and high specificity (78%).Our results agree with Dibiscegli and his colleagues (1992) who reported considerable increase in the levels of Ferritin in 30% of 80 patients with viral chronic hepatitis and its increase in males was higher than females16. Also, Albert and his colleagues (1994) reported increase in serum Ferritin in about 31% of HCV positive patients 17. Patil, et al18., found an independent association between serum ferritin levels and HCC in patients with CLD of viral etiology. Combination of AFP and ferritin is useful for early detection of HCC. Correct diagnosis were made in 65.9% of cases by measurement of serum AFP only ,in 56.8% of the cases by measurement of ferritin ,and in 88.6% of the cases by combination of these two tests, and combination of tests for HCC did not decrease the specificity appreciably19.While our results disagreed with Lin, et al20., who considered that several proteins markers in serum have been studied for possible use in the detection of HCC but have not proven to be useful because of poor sensitivity and/or specificity. These include C-reactive protein, matrix metalloproteinase-2 and -9, tissue polypeptide specific antigen, beta2microglobulin, CA 19-9, carcinoembryonic antigen, CA 72-4 and Ferritin. Liebman, et al11., first reported that 67% of patients with HCC had abnormally elevated levels of des- γ -carboxyprothrombin (DCP), also known as the protein induced by vitamin K absence or antagonist II (PIVKA-II). A significant elevation of PIVKA-II and AFP levels in HCC group compared to control and HCV groups. PIVKA-II showed more increase than AFP level in malignant compared to benign liver www.ujponline.com diseases 11. There is excessive synthesis of prothrombin precursors by human HCC tissues, which might contribute to production of PIVKA-II, rendering the latter a useful marker for HCC with a very high specificity21. Durazo, et al., reported that PIVKA-II levels significantly correlate with histopathological grade of HCC and size of solitary tumors, being 25 times higher in tumors more than 2 cm, compared to those less than 2 cm. AFP showed no significant correlations with the stage of HCC. In contrary PIVKA-II showed gradual increase in its level with increase of disease stage22. PIVKA-II was positive in 96%, 93% and 74% in patients with tumor size larger than 5, 3–5, and less than 3 cm while AFP was positive in 65%, 57% and 48% respectively. PIVKA-II levels showed significant elevation in HCC patients with portal vein thrombosis, while AFP level was not affected 21. Recent studies have revealed that DCP functions as a growth factor and might play significant roles in cancer progression. Thus, DCP represents a potential target of drug discovery to establish new chemotherapeutic strategy for HCC. So, DCP have revealed not only the usefulness of this molecule as a diagnostic marker but also its significant role in cancer progression23. Regarding to this study, PIVKA-II showed sensitivity and specificity of 80% and 35% respectively at cut-off value (4.15 ng/ml).In a study Ryaidh, et al., reported that high increasing ceruloplasmin levels, copper and decreased in concentrations of zinc and the increased concentrations of copper in serum do not seem to result from a shift of zinc into or release of copper out of the malignant tumor tissue. Cp accumulates to extremely high levels in the serum of the transgenic mice developing HCC24. About one-half of the Cp from tumor bearing mice is complexed with copper; this is shown by its characteristic absorption at 600 nm as well as by the high specific phenol oxidase and ferroxidase activities and by the immunological quantification of holo-Cp in the serum of the transgenic mice25.Our results showed that Ceruloplasmin with Cutoff value (322.5 ng/ml) showed a sensitivity of (68 %) and specificity of (71%). CONCLUSION Further investigations on a larger scale using wellstandardized techniques are recommended to validate the cut off value or define appropriate one. REFERENCES 1. Bosch F, Ribes J, Diaz M, et al. Gastroenterology 2004; 127: S5–S16. 2. El-Serag. N Engl J Med .2011; 365:1118-27. 3. Donato F, Tagger A, Gelatti U, et al. Alcohol and hepatocellular carcinoma: the effect of lifetime intake and hepatitis virus infections in men and women. Am J Epidemiol. 2002. 155: 323-31. Universal Journal of Pharmacy, 04(03), May-June 2015 96 Mona Talaat Kamel et al. UJP 2015, 04 (03): Page 92-97 4. Lehman, Mark L. Elizabeth M. Epidemiology of hepatitis viruses among hepatocellular carcinoma cases and healthy people in Egypt: A systematic review and meta-analysis DOI2008: 10.1002/ijc.23937. 5. Olfat S, Amal A, Hosam E, et al.: PIVKA-II as early diagnostic marker for hepato cellular carcinoma: an Egyptian study. International Journal of Advanced Research 2013; 1(9): 135141. 6. Wu J. Serum alpha-fetoprotein and its lectin reactivity in liver diseases: a review.Annals of Clinical and Laboratory Science 1990; 20(2): 98– 105. 7. Bertino G, Ardiri A, Malaguarnera M, et al. Hepatocellualar carcinoma serum markers. SeminOncol. 2012; 39(4):410–33. 8. Nicole M, Katherine A , Rebecca J, et al. Serum Ferritin Concentration Predicts Mortalityin Patients Awaiting Liver Transplantation.the American Association for the Study of Liver Diseases.Wiley Inter Science. 2010DOI 10.1002/hep.23537. 9. Metwally M, Zein C, Zein N. Clinical significance of hepatic iron deposition and serum iron values in patients with chronic hepatitis C infection. Am J Gastroenterol.2004; 99(2): 286-91. 10. Poo J, Rosas-Romero, Montemayor A, et al. Diagnostic value of the copper/zinc ratio in hepatocellular carcinoma: a case control study. J Gastroenterol.2003; 38(1):45-51. 11. Liebman H, Furie B, Tong M, et al. Des-ycarboxy (abnormal) prothrombin as a serum marker of primary hepatocellular carcinoma. N Engl.J Med, 1984; 310: 1427-1431. 12. Mona Abu El Makarem. An Overview of Biomarkers for the Diagnosis of Hepatocellular Carcinoma. Hepat Mon, 2012; 12: 10. HCC): e6122. DOI: .10.5812/hepatmon.6122 . 13. Tara B, SitkiCopur M. Biomarkers for Hepatocellular Carcinoma International Journal of Hepatology Volume 2012, Article ID 859076, 7 pages doi:10.1155/2012/859076. 14. Stefaniuk P, Cianciara J, Wiercinska-Drapalo A. Present and future possibilities for early diagnosis of hepatocellular carcinoma. World J Gastroenterol 2010; 16: 418–24. 15. Chapoutot C, Esslimani M, Joomaye Z, et al. Liver iron excess in patients with 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. www.ujponline.com hepatocellular carcinoma developed on viral C cirrhosis. Gut 2000; 46: 711–714. Dibiscegli A, Axiotis C, Hoofnagle J. Measurement of iron status in patients with chronic hepatitis. Gastroentrology 1992; 102: 2108-13. Arbert N, Konikoff F, Moshko W. 1994. Increased serum iron and iron saturation without liver iron accumulation distinguish chronic hepatitis C from other chronic liver disease. Dig Dis Sci., 1994; 39: 2656-9. Patil P, Mohandas K, Bhatia S, et al. Serum ferritin and the risk of hepatocellular carcinoma in chronic liver disease of viral etiology: a case-control study. Indian J Gastroenterol., 2014; 33(1):12-8. doi: 10.1007/s12664-013-0367-5. Tatsuta M, Yamamura H, Lishi H, et al . Value of Serum Alpha- Fetoprotein and Ferritin in the Diagnosis of Hepatocellular Carcinoma, Oncology, 1986; 43: 306-310. Lin Z, Wang L, Yu M, et al. Role of serum Creactive protein as a marker of hepatocellular carcinoma in patients with cirrhosis. J Gastroenterol Hepatol. 2000; 15: 417-21. Nadia I, Sherif M, Hanan E, et al. Impact of PIVKA-II in diagnosis of hepatocellular carcinoma%http://dx.doi.org/10.1016/j.jare.2 012.10.004. Durazo F, Blatt L, Corey W, et al. Des-gammacarboxyprothrombin, alpha-fetoprotein and AFP-L3 in patients with chronic hepatitis, cirrhosis and hepatocellular carcinoma. J GastroenterolHepatol 2008; 23: 1541–8. Inagaki Y, Tang W, Xu H, et al. Des-gcarboxyprothrombin: clinical effectiveness and biochemical importance. Biosci Trends2014; 2: 53–60. Ryaidh S, Saeed H, Rafah R, et al. Evaluation of levels Ceruloplasmin, Copper, Zinc, Calcium and Non-Ceruloplasmin_bound Copper in Lung and Liver cancer Patients. journal of kerbala university 2014 ISSN: 18130410. Dominique P, VeÂronique P, Nicole B,et al. High levels of ceruloplasmin in the serum of transgenic mice developing hepatocellular carcinoma Eur. J. Biochem. 2001; 268: 1491±1499. Source of support: Nil, Conflict of interest: None Declared Universal Journal of Pharmacy, 04(03), May-June 2015 97