hrs
advertisement

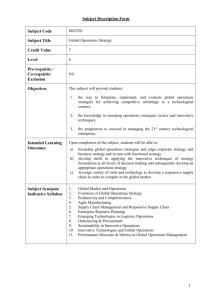
CLINICAL TYPES OF HEPATORENAL SYNDROME (HRS) Type-2 HRS 6 Creatinine (mg/dL) 5 Type-1 HRS Cefotaxime 4 Therapeutic paracentesis 3 Encephalopathy Jaundice 2 1 0 -6 -4 -2 Months 0 1 2 Weeks 3 DIFFERENCES BETWEEN TYPE-1 AND TYPE-2 HRS Type-2 Type-1 Moderate and steady Severe and progressive Setting Non-azotemic cirrhosis Type-2 HRS Onset Spontaneous Precipitated Refractory ascites Terminal hepatorenal failure Months Days Renal failure Consequence Survival HRS. SURVIVAL 1.0 Median survival Type-1 Type-2 Probability 0.8 15 days 150 days 0.6 Type-2 0.4 p<0.0001 0.2 Type-1 0.0 0 100 200 300 400 500 600 Days TIME-COURSE OF THE CIRCULATORY, NEUROHORMONAL AND RENAL FUNCTION ABNORMALITIES IN CIRRHOSIS No Ascites Ascites Time Hyperdinamic circulation RAAS, SNS and sodium retention ADH and hyponatremia HRS CARDIOVASCULAR HEMODYNAMICS IN 8 PATIENTS DEVELOPING TYPE-1 HRS AFTER SBP At SBP diagnosis SBP-HRS MAP (mmHg) 83±7 73±8* PRA (ng/mL.h) 18±11 28±12* 1137±220 1268±320 5.7±0.9 4.6±0.7* SVR (dyn.s/cm-5) CO (L/min) * p<0.02 Ruiz del Arbol et al., Hepatology 2002 CARDIOVASCULAR HEMODYNAMICS IN 12 PATIENTS DEVELOPING TYPE-1 HRS* Baseline Type-1 HRS p MAP (mmHg) 84±2.6 70±2.3 <0.001 PRA (ng/mL.h) 12.9±2.6 25.8±3.4 <0.01 NE (pg/mL) 735±69 1385±99 <0.001 SVR (dyn.s/cm-5) 1099±81 1211±97 NS CO (L/min) 5.8±0.2 4.6±0.3 <0.01 RAP (mmHg) 7±0.8 5±0.5 <0.01 PCP (mmHg) 8.7±1 6.5±1 <0.01 HR (bpm) 86±5 84±4 NS * baseline measurements: 9±1 months prior HRS Ruiz del Arbol et al., Hepatology 2005 80 0.9 * p<0.05 60 40 * * 20 Resistive index middle cerebral artery Brachial blood flow (mL/min) REGIONAL CIRCULATORY CHANGES IN CIRRHOSIS p<0.001 0.8 0.7 0.6 0.5 0.4 0 H NA A HRS Maroto et al., Hepatology 1993 H NA A Guevara et al., Hepatology 1998 Healthy subjects (H), cirrhotic patients without ascites (NA), with ascites (A) and with hepatorenal syndrome (HRS) CHANGES IN HEPATIC HEMODYNAMICS ASSOCIATED WITH TYPE-1 HRS 30 HVPG (mmHg) p<0.05 25 20 15 At SBP diagnosis After SBP resolution HBF IN PATIENTS DEVELOPING TYPE-1 HRS Hepatic blood flow (mL/min) HVPG IN PATIENTS DEVELOPING TYPE-1 HRS AFTER SBP 1000 800 600 400 Baseline Type-1 HRS Baseline measurements: 9±1 months prior HRS Ruiz del Arbol et al., Hepatology 2002 Ruiz del Arbol et al., Hepatology 2005 INCIDENCE OF RELATIVE ADRENAL INSUFFICIENCY* IN CIRRHOTIC PATIENTS (n=20) WITH SEPTIC SHOCK Non-cirrhotic patients 10-40% Cirrhotics Child B 25% Cirrhotics Child C 75% * Diagnostic criteria: - baseline cortisol <9 mg/dL - increase in cortisol after ACTH <9 mg/dL - peak cortisol <20 mg/dL Fernández et al. (unpublished) TYPE-I HRS AS A PART OF A MULTIORGAN FAILURE Spontaneous bacterial peritonitis or other precipitating event Adrenal dysfunction Increase in arterial vasodilation Decrease in cardiac output A-II, NE, ADH resistance to portal venous flow Aggravation of portal hypertension Regional arterial vasoconstriction Kidneys HRS Brain Encephalopathy Liver Liver failure EFFECT OF VASOCONSTRICTORS (Ornipressin and Terlipressin) PLUS I.V. ALBUMIN IN TYPE-1 HRS Baseline (n=15) Day 7 (n=9) Day 14 (n=7) MAP (mmHg) 70±8 77±9 79±12 PRA (ng/mL.h) 15±15 2±3 1±1 1257±938 550±410 316±161 Creatinine (mg/dL) 3±1 2±1 1±1 GFR (mL/min) 9±1 25±2.5 41±1.5 NE (pg/mL) Guevara et al., Hepatology 1998; Uriz et al., J Hepatol 2000 SERUM CREATININE BEFORE AND AFTER TREATMENT OF TYPE-1 HRS (11 cases) WITH TERLIPRESSIN PLUS ALBUMIN Serum creatinine (mg/dL) 5 4 3 2 1 0 Baseline 1 day 1 month After treatment Ortega et al., Hepatology 2002 TREATMENT OF HRS WITH VASOCONSTRICTORS AND ALBUMIN (Group 1) AND STANDARD MEDICAL THERAPY (Group 2). REVIEW OF 18 STUDIES Group 1 (n=154) Group 2 (n=137) MCFS* (n=99) Reversal of HRS 61.7% 2.9% 58% HRS recurrence 20% - - Survival 1 month 41.6% 3% 40% Survival 3 months 30% 0% 22% 12.3% - 13% Liver transplantation * Multicenter French Study TREATMENT OF TYPE-1 HRS WITH TERLIPRESSIN PLUS I.V. ALBUMIN vs TERLIPRESSIN Terlipressin + Terlipressin albumin (n=13) (n=8) Complete response 10 2 Survival >1 month 12 2 OLT 5 0 Ortega et al., Hepatology 2002 TIPS IMPROVES CIRCULATORY AND RENAL FUNCTION IN TYPE-1 HRS (7 patients) After treatment Baseline Renin (ng/mL/h) NE (pg/mL) Creatinine (mg/dL) GFR (mL/min) Day 7 Day 30 18±5 6±2 3±1 1257±187 853±102 612±197 5.0±0.8 3.7±1.0 1.8±0.4 9±4 11±5 27±7 Guevara et al., Hepatology 1998 PRA (ng/mL.h) CIRCULATORY SUPPORT WITH I.V. ALBUMIN IN PATIENTS WITH SBP. EFFECT ON ARTERIAL BLOOD VOLUME 9 8 7 6 5 4 3 2 1 0 * * * * p<0.05 1 3 Cefotaxime + albumin 6 9 Days Cefotaxime Sort et al., N Engl J Med 1999 CIRCULATORY SUPPORT WITH I.V. ALBUMIN IN PATIENTS WITH SBP. EFFECT ON HRS DEVELOPMENT AND HOSPITAL MORTALITY Cefotaxime (n=63) Cefotaxime + albumin (n=63) Resolution of infection 57 (93%) 59 (98%) HRS 20 (32%) 6 (10%)* Hospital mortality 17 (27%) 6 (10%)* * p<0.001 Sort et al., N Engl J Med 1999 EFFECTS OF HYDROXYETHYL STARCH (HES) AND ALBUMIN (ALB) ON EFFECTIVE BLOOD VOLUME IN SBP MAP (mmHg) PRA (ng.mL/h) Baseline At resolution p HES 80±15 81±8 NS ALB 76±9 85±13 0.01 HES 8.5±7.3 16.8±24.6 NS ALB 5.7±4.7 3.1±3.4 0.04 Fernandez et al., Hepatology 2005 EFFECTS OF HYDROXYETHYL STARCH (HES) AND ALBUMIN (ALB) ON PERIPHERAL ARTERIAL CIRCULATION IN SBP SVR (dyn/cm5) NO (nmol/mL) vWF:Ag (U/dL)* Baseline At resolution p HES 777±239 778±290 NS ALB 668±134 803±197 0.03 HES 39±13 63±32 0.03 ALB 61±30 78±55 NS HES ALB 297±44 331±35 278±47 257±65 NS 0.01 * vWF:Ag Von Willebrand-related antigen factor Fernandez et al., Hepatology 2005 EFFECT OF I.V. ALBUMIN ON SYSTEMIC HEMODYNAMICS IN CIRRHOSIS Albumin infusion Intravascular volume expansion Inhibition of endothelial activation Increased cardiac preload Decreased NO synthesis Improvement in left ventricular function Increased systemic vascular resistance IMPROVEMENT OF CIRCULATORY DYSFUNCTION