final presentation on the day
advertisement

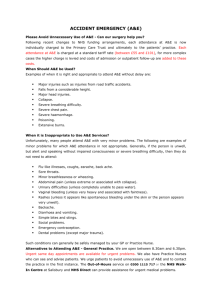
Urgent and Emergency Care Review Keith Willett Director of Acute Care www.england.nhs.uk Annual National Crisis Care Concordat Summit November 2015 Annual National Crisis Care Concordat Summit • update on UECR review • establishment of UEC Networks • Crisis Care access & waiting time standards • winter readiness programme • UEC vanguards to lead the way www.england.nhs.uk Urgent and Emergency Care Review Vision For those people with urgent but non-life threatening needs: • We must provide highly responsive, effective and personalised services outside of hospital, and • Deliver care in or as close to people’s homes as possible, minimising disruption and inconvenience for patients and their families For those people with more serious or life threatening emergency needs: Mental and physical health www.england.nhs.uk • We should ensure they are treated in centres with the very best expertise and facilities in order to maximise their chances of survival and a good recovery UEC Review – 5 key system changes 1. Provide better support for people to self-care Mental health 2. Help people with urgent care needs to get the right advice in the right place, first time 3. Provide highly responsive urgent care services outside of hospital so people no longer choose to queue in A&E 4. Ensure that those people with more serious or life threatening emergency needs receive treatment in centres with the right facilities and expertise in order to maximise chances of survival and a good recovery 5. Ensure that the urgent and emergency care system becomes more than just the sum of its parts through the creation of urgent care: create UEC networks www.england.nhs.uk Helping people help themselves Self care: • Better and easily accessible information about self-treatment options – patient and specialist groups, NHS111 on a digital platform as part of NHS Choices (nhs.uk) • Accelerated development of advance care planning • Right advice or treatment first time - enhanced NHS111 - the “smart call” to make: • Improve patient information for call responders (ESCR, care plan) • Comprehensive Directory of Services (mobile application) • Greater levels of clinical input (mental health, dental heath, paramedic, pharmacist, GP) • Booking systems for GPs, into UCCs, dentists, pharmacy 6 Highly responsive urgent care service close to home, outside of hospital • Faster, convenient, enhanced service: • Same day, every day access to general practice, primary care and community services advice • Harness the skills of community pharmacy, minor ailment service • 24/7 clinical decision-support for GPs, paramedics, community teams from (hospital) specialists – no decision in isolation • Support the co-location of community-based urgent care services in Urgent Care Centres and Ambulatory Care, • Develop 999 ambulances so they become mobile urgent community treatment services, not just urgent transport services • Single Point of Access with Community and Social Care 7 From life threatening to local – where is the expertise and facilities? • Identify and designate available services in hospital based emergency centres • Urgent Care Centres – primary care, consistent, access to network • Emergency Hospital Centres - capable of assessing and initiating treatment for all patients • Emergency Hospital Centres with Specialist services - capable of assessing and initiating treatment for all patients, and providing specialist services: transfer or bypass access, 24/7 specialist network support • Emergency Care Networks: • Connecting all services together into a cohesive network overall system becomes more than just the sum of its parts 8 Parity of esteem for mental health Emergency Centre with Specialist Services UEC Review: arriving here • Three phases to the programme 2013-15: Phase 1 DESIGN Jan – Oct 2013 Phase 2 PRODUCT DELIVERY Nov 13 – Dec 14 Phase 3 IMPLEMENTATION Jan 15 – now • Examined the challenges the UEC system faces, and what principles and objectives a new system should be based on COMPLETED • Translation of ‘what’ needs to happen into ‘how’ these ideas can be operationalised COMPLETED • NOW the final phase is focused on implementing those new models of care and ways of working UEC national enablers: • Self-care initiatives Realising the value, ‘Self-care for Life’ • NHS 111 as portal to out-of-hours integrated service mental health key component of clinical hubs • New system-wide indicators and measures UEC outcomes for both mental/physical health • Local capacity planning tool testing with vanguards: includes mental health UEC products – published help ‘Transforming urgent and emergency care in England’ • Role & establishment of UECNs, published • Safer, Faster Better published • Clinical models for ambulance service publication end 2015 • Improving referral pathways between urgent and emergency services in England publication pending • Financial modelling methodology publication end 2015 • Commissioning guidance for Urgent Care Centres, Emergency Centres and Emergency Centres with specialist services publication end 2015 The four greatest challenges 1. Payment system reform 2. Information sharing 3. System measures 4. Workforce and skills shift 13 Proposed new payment model • A coordinated and consistent payment approach across all parts of the UEC network • Making use of three elements: Quality Core – Facilities and service standards Capacity - Core Fixed in-year cost “always on” Volume variable • future-proofed Volume - Process measures formative not summative Acting throughout payment Incentives and Sanctions – Patient outcome measures (ToC, PROMs) Patient safety and experience measures (mortality, SAEs, PREMs) mental health included in all UEC networks and payment approaches 14 Summary Care Record: Creating the records • SCRs are an electronic record of key information from the patient’s GP practice • As a minimum contain medication, allergies and adverse reactions • Improved functionality with additional information including crisis care plans GPs need to obtain consent 55m > 2.5m SCRs created contacts in last year (96%) To find out more or enable SCR: scr.comms@hscic.gov.uk 12 secs or @NHSSCR Mobile access to the Directory of Services • Testing with vanguard sites during winter 2015/16 System wide outcomes Outcomes, standards and specifications • Shift to outcome measurement for whole system • List of indicators developed under 3 domains: • Clinical Pathway • Patient Experience • Staff Experience • All will measure physical and mental health www.england.nhs.uk Establishing Urgent and Emergency Care Networks – the purpose • 24 networks based on geographies required to give strategic oversight of urgent and emergency care on a regional footprint • 1 - 5million population based on population rurality, local services • To improve consistency of quality, access and set objectives for UEC by bringing together SRG members and other stakeholders to address challenges that are greater than a single SRGs can solve in isolation • • • • • Access protocols to specialist services Ambulance protocol Clinical decision support hub NHS 111 services Uniform approach to mental health crisis www.england.nhs.uk Programme: 2015/16: Crisis Care access standards Where do people present with urgent MH needs and what response should be expected in the first 24 hrs? (Phase 1) SELF MGT & CARE PLANNNG USE OF DIGITAL TECHNOLOGY ACCESS standards developed Primary care response (in and OoH) 111 (and the DoS) and 999 24/7 MH crisis line (tele-triage & tele-health) and 24/7 community-based crisis response Blue light response, transport hub, S135/136 response & health based places of safety Urgent and emergency Liaison MH services (+ alcohol care teams) during 2016, not ‘just’ a waiting time’, but setting up the system to: 1. Describe the standards – access time + NICE concordant care 2. Agree how to measure 3. Where are we starting from? - a baseline 4. What will it take to get to where we need to be? - gap analysis 5. How? - commissioning guides 6. Drive quality improvement 7. Adapt the workforce 8. Build a payment model 9. Report openly Ensure joined up approach for people with co-existing MH and substance misuse conditions… 19 UEC winter readiness • Assurance process for System Resilience Groups (8 high impact interventions) SRGs provided detailed capacity plans: • Community care beds (nursing residential and dementia beds, specialist Elderly Mental Infirm beds) intermediate care (bed-based and home-based), district nurses and community matrons, and allied health professionals • From this year, 5 mandatory mental health indictors included for first time: Join up between SRGs and local Concordat groups 24/7 crisis resolution and home treatment teams 24/7 on site urgent and emergency liaison mental health S.136 health-based places of safety Up to date mental health Directories of Service www.england.nhs.uk UEC vanguards • Focus on i) local health systems with strongest network progress and ii) addressing greatest operational challenges • Accelerate pace of change • Drive new ways of working across organisation boundaries • Tripartite support for implementation, help remove barriers • Test beds for new UEC initiatives (relationships, workforce, clinical decision support hubs, payment model, new indicators, mental health) • Meet explicit requirements on implementing best practice and national policy expectations • £4m pump prime investment to UEC vanguards to test and evaluate innovative models of mental health crisis care for children and young people, and incorporating mental health crisis in testing of payment models www.england.nhs.uk A new strong consumer offer to the public: NHS urgent care starts to look like what the patients tell us they want, not what we have historically offered • A single number – NHS 111 – for all your urgent health needs • Be able to speak to a clinician if needed • That your health records are always available to clinicians treating you wherever you are (111, 999, community, hospital) • To be booked into right service for you when convenient to you • Care close to home (at home) unless need a specialist service • Provide specialist decision support and care through a network …….. we will change patient and staff behaviour through experiential learning 22 Urgent and Emergency Care Review the new offer It’s great to share so much with this group about my depression I’m so pleased my mum got specialist care really fast and I didn’t lose her 23 It’s like everyone knows all about my problem I feel so much better for not having to go all the way to hospital every time I need help