Hemophagocytic Lymphohistiocytosis
advertisement

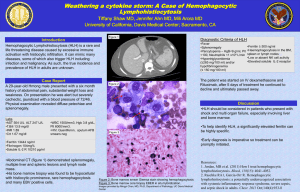
Hemophagocytic Lymphohistiocytosis By: Michelina Kauffman, MD PGY-3 December 4, 2015 Disclosures Neither Dr. Pirich nor I have any financial disclosures. Objectives • Untangle the differences between primary HLH, secondary HLH, and MAS. • Review the etiology and risk factors for HLH. • Describe the variable clinical presentations of HLH. • Review the HLH-2004 diagnostic criteria. • Discuss treatment strategy and prognosis. Which lab finding would be most helpful in the diagnosis of HLH? 20% 1. 2. 3. 4. 5. 20% 20% 2 3 20% 20% Hemoglobin 8.4 g/dL Platelets 164 x 109/L Neutrophils 4.1 x 109/L Ferritin 11,900 mg/L sIL-2R 150 U/mL 1 4 5 What is the genetic association for secondary hemophagocytic lymphohistiocytosis? 20% 20% 20% 2 3 20% 20% 1. None 2. PRF1 3. UNC13D 4. Chediak-Higashi 5. I don’t know. 1 4 5 An 8 mo M is admitted to the PICU with a four day history of persistent fever and an erythematous rash. He is found to have hepatosplenomegaly, anemia, thrombocytopenia, and hyperferritonemia. You suspect this patient may have HLH. What is the best study to confirm this diagnosis? 1. 2. 3. 4. MRI Brain Lumbar puncture Genetic testing Bone marrow aspirate and biopsy 5. Abdominal ultrasound 20% 1 20% 20% 2 3 20% 4 20% 5 For patients with familial HLH, hematopoietic cell transplantation remains the only long-term curative treatment. 50% 50% 1.True 2.False 1 2 Case Presentation A PH 6 wo AA F was taken to the ED for a fever of 101.4F at home. She had felt subjectively warm for 3-4 days prior but no temperatures had been obtained and no other symptoms were noted. On arrival, her temperature was 103.4F and her exam was remarkable for fussiness and hepatosplenomegaly. A full sepsis work up was performed and she was empirically started on ampicillin and cefotaxime in the ED. Lab work up was concerning for: • CBC: WBC 4, Hgb 7.3, and Plt 65 • CMP: TB 6.2, AST 321, ALT 127 • CSF: P 73, G 52, WBC 22, RBC 0 • Coags: PT 23.6, PTT 52.9, INR 2, Fibrinogen 60 • Blood, Urine, and CSF Cx’s – P Due to concern for sepsis and DIC the patient was admitted to the PICU for further care. History of HLH • The first documented description of HLH was published by Farquhar and Claireux at the University of Edinburgh in 1952. • They noted a constellation of symptoms in two previously healthy infant siblings: • • • • Recurrent, unexplained fevers Progressive panhematopenia Hepatosplenomegaly Bruising • At autopsy, they found “inflammatory cell infiltration” and a “great proliferation of histiocytes.” Introduction • HLH is a non-malignant, aggressive, life-threatening syndrome characterized by excessive immune activation. • HLH typically affects infants from birth to 18 months of age but can be seen in children and adults. • Although the distinction is blurred, HLH has been historically divided into primary and secondary types. • Rapid recognition and initiation of treatment is necessary for survival. Immune System Review Immune System Review The normal elimination of activated macrophages occurs via NK cells and CTLs that lyse target cells through perforin-dependent cytotoxicity. 1 Create a pore in the macrophage membrane. 2 Deliver cytolytic granules into the macrophage. 3 Proteases, such as Granzyme B, initiate cell death. HLH Pathophysiology • Excessive inflammation occurs due to overactive but impaired immune function. • There is a lack of normal feedback to activated macrophages which leads to excessive activity. • Most patients exhibit impaired cytotoxic function of NK cells and CTLs. • NK cells and/or CTLs fail to eliminate activated macrophages. • Tissue damage is caused by excessive cytokine production otherwise known as a cytokine storm. Cytokine Storm A pro-inflammatory state is created which is ultimately responsible for multi-organ failure and high mortality without treatment or with delayed treatment. Hemophagocytosis • The pathologic finding of activated, histologically benign macrophages engulfing host blood cells. • Can be seen in biopsies of lymph nodes, spleen, liver, bone marrow, and sometimes CNS. • Hemophagocytosis alone is not pathognomonic, nor required, for diagnosis of HLH. • In 1996, of 122 children with HLH from the Histiocyte Society’s International Registry, only 75% had evidence of hemophagocytosis at diagnosis. Primary vs. Secondary HLH Familial HLH • Primary HLH is caused by inborn defects in the primary cytotoxicity effector pathway in lymphocytes and NK cells. • Autosomal Recessive • Incidence 1:50,000 • Median survival is <2 months if left untreated. • Onset is typically during infancy or early childhood. • May be triggered by infection. • Non-syndromic forms consist of 5 mutations, FHL 1-5. • FHL 1 mutation is unknown. Immunodeficiency Syndromes • Chediak Higashi syndrome • Mutations in CHS1/LYST • Griscelli syndrome type II • Mutations in RAB27A • Hermansky-Pudlak syndrome type II • Mutations in AP3B1 • Partial oculocutaneous albinism, immunodeficiency, and neurologic abnormalities. FHL-2 FHL-5 FHL-4 FHL-3 Secondary HLH • sHLH develops as a consequence of a strong immunologic response to a stimulus: • • • • Infection Rheumatologic illness such as JIA or SLE Malignancy, either at presentation or during treatment Immunodeficiency • There is no inherited immune defect found in sHLH. • More prevalent than FHL but incidence is poorly defined. • Median age of onset is higher than FHL. Epstein-Barr Virus • The most frequent infectious trigger of familial and secondary HLH. • Of 219 patients diagnosed with infection associated HLH from 1979 to 1995, 55% were attributed to EBV. • Janka, G. (1998) Hematology/Oncology Clinics of North America • EBV associated HLH varies from spontaneously resolving inflammation to unrelenting disease requiring HCT. • EBV-HLH has been associated with acute infections in B cells, T cells, and NK cells. Macrophage Activation Syndrome • Life threatening complication of systemic inflammatory conditions characterized by all of the clinical symptoms and laboratory findings of HLH. • JIA and SLE are the most common. • Clinical manifestations include fever, hepatitis, hepatosplenomegaly, lymphadenopathy, and DIC. • Cytopenias are typically a late finding. • May be the first manifestation of the rheumatologic disease. • In patients with known JIA or SLE, infections, flares, or changes in medication may trigger MAS. Malignancy • HLH has been reported with lymphomas or leukemia of the T or NK cell lineage. • Many patients have a simultaneous bacterial, viral, or fungal infection that may trigger HLH. • May occur during treatment for a known cancer in clinical remission or as a manifestation of an aggressive uncontrolled cancer. • Iatrogenic immune dysregulation Clinical Presentation Clinical Presentation • The presentation of HLH is variable and laboratory findings are similar to more common disease processes. • Typical findings include persistent fever, splenomegaly with or without hepatomegaly, and cytopenias that affect at least two cell lines. • Less common initial findings include lymphadenopathy, rash, jaundice, and edema. • Clinical features may not be initially or simultaneously present, however, patients are usually acutely ill at presentation. Liver Disease • Most patients have evidence of hepatitis on presentation. • Clinical findings include jaundice, hepatomegaly, and bleeding. • Autopsy findings of 22 out of 27 patients diagnosed with HLH found infiltration of lymphocytes into the portal tracts similar to what is seen in chronic persistent hepatitis. • Ost, A. (1998). Histopathology • Lab findings include hypertriglyceridemia, elevated transaminases, hyperbilirubinemia, and hyperferritonemia. • A serum ferritin >10,000 mg/L is highly sensitive and specific. • Impaired synthetic function and clotting factor consumption leads to hypofibrinogenemia as well as prolongation of PT and PTT. Pulmonary Dysfunction • In a review of radiographic abnormalities in 25 patients, 17 had acute respiratory failure with alveolar or interstitial opacities. • 88% fatal • Worsening pulmonary function is an ominous sign and should suggest inadequate control of HLH. Bone Marrow Abnormalities & Cytopenias • Anemia and thrombocytopenia occur in >80% of patients at presentation. • The cellularity of bone marrow may be normocellular, hypocellular, or hypercellular. • Presence of hemophagocytosis ranges from 25-100%. • Hemophagocytosis in the bone marrow may be seen in other disease states. • The diagnosis of HLH should never be made solely based on the presence or absence of hemophagocytosis. Neurologic Symptoms • More than 1/3 of patients will present with neurologic symptoms. • Seizures, meningismus, decreased level of consciousness, cranial nerve palsy, psychomotor retardation, ataxia, irritability, hypotonia, or peripheral neuropathy • CSF is abnormal in more than half of patients. • Hyperprotienemia, pleocytosis, and hemophagocytosis • Variable MRI findings that correlate with symptoms. • Discrete lesions, leptomeingeal enhancement, or global edema. • Retinal hemorrhages, swelling of the optic nerve, and infiltration of the choroid has been seen in infants. Skin Manifestations Differential Diagnosis • Viral infections • Sepsis • Malignancy • Metabolic disorder • Non Accidental Trauma • If the patient improves clinically, it is most likely not HLH. • Spontaneous partial remission has been observed but relapse is inevitable without appropriate treatment. Diagnostic Criteria HLH-2004 • Molecular diagnosis consistent with HLH. • Or 5 of the 8 criteria listed below: • Clinical criteria • Fever • Splenomegaly • Laboratory criteria • Cytopenias: Hgb <9 g/dL; platelets <100 x 109/L; neutrophils <1x109/L • Fasting hypertriglyceridemia and/or hypofibrinogenemia • Hyperferritinemia: >500 mg/L • Elevated soluble CD25 (sIL-2R): ≥ 2400 U/L • Low/Absent natural killer function • Histopathologic criteria • Hemophagocytosis in bone marrow, spleen, lymph node, or CSF Treatment Supportive Care • Neutropenic precautions • Prophylaxis for Pneumocystis jirovecii and fungal infections. • IVIG supplementation. • Fever should be evaluated for reactivation and opportunistic infection. • Broad spectrum antibiotics should be initiated. • Bleeding • Goal platelet count >50 x 109/L. • Platelets, FFP, cryoprecipitate, and activated factor VII. • Cardiac function • Baseline cardiac function should be evaluated because patients may present with or develop acute cardiac dysfunction. Treatment • Current management involves: • Controlling the hyperinflammatory state. • Control or eliminate the infectious trigger. • Stop T-cell proliferation and activation. • Stop or control the inflammatory process by blocking excessive cytokine production and function. • Correct the underlying genetic defect by allogeneic HCT. Treatment • To control T-cell proliferation and activation, based on the HLH-94 protocol, an 8-week course of dexamethasone and etoposide therapy is used. • Remission rate was 71% and 5 year post-HCT survival probability was 54%±6%. • The HLH-2004 protocol was developed in an effort to improve remission rates. • Intensification of initial therapy by adding cyclosporine and intrathecal steroids. CNS Treatment • Patients may present with CNS involvement or inflammation may recur as treatment doses are being tapered. • Patients with proven CNS disease should be treated with weekly IT MTX and hydrocortisone until CSF abnormalities and symptoms resolve. • CNS involvement suggests a genetic etiology with associated morbidity so HCT is recommended. Treat the Underlying Disease • EBV • Rituximab • Rheumatologic disorder • Immunosuppression, IVIG • Malignancy • Treat malignancy first vs. HLH Salvage Therapy • If patients do not display at least a partial response within 2-3 weeks of therapy, salvage therapy should be considered. • Alemtuzumab • Monoclonal antibody to CD52. • Induced partial response in 64% of patients. • In HLH-2004 refractory patients, may be useful as a bridge to transplant. Hematopoietic Cell Transplant • HCT is the only long-term curative treatment for familial HLH. • Reasons to transplant: • Proven familial/genetic disease • Recurrent/refractory disease • CNS involvement • Myeloablative Conditioning (MAC) • Standard treatment with busulfan, cyclophosphamide, and etoposide with or without antithymocyte globulin (ATG). • Associated with high transplantation related mortality. • Reduced Intensity Conditioning (RIC) • Alemtuzumab, fludarabine, and melphalan. • Better outcomes in HCT, three year survival of 92%. Risk Factors • In October 2011, Trottestam et al., published a study evaluating 232 children with HLH to determine risk factors that predict mortality. • At onset: hyperbilirubinemia, hyperferritinemia, and CSF pleocytosis. • Two weeks into therapy: hyperferritonemia and thrombocytopenia. • No improvement of fever and anemia. Follow Up • Relapse, if it occurs, generally occurs within the first year. • Close monthly follow up is necessary to evaluate for recurrent disease. • Signs of recurrent disease: fever, hepatosplenomegaly, neurological abnormalities. • Labs that indicate recurrence: cytopenia and elevated ferritin, serum transaminases, and sIL-2R. Resources • www.histio.org • https://go.cincinnatichildrens.org/service/hlhphysician/overview.php Case Conclusion • PICU course: all cultures were found to be negative and antibiotics were discontinued. Viral studies including HSV, CMV, and EBV were negative. She was found to be adenovirus positive. • Due to persistent cytopenia and evidence of DIC in spite of aggressive supportive management, Heme/Onc was consulted. Concern for HLH led to investigation of ferritin, found to be elevated at 9045, and fasting triglyceride of 164. • Bone marrow aspirate did reveal hemophagocytosis. • Lab studies sent to Cincinnati confirmed the diagnosis with: • Elevated sIL-2R 49,724 and Perforin level close to zero, indicative of PRF1 gene mutation. • Treatment was initiated per HLH-94 protocol and she was transferred to MUSC for HCT. Which lab finding would be most helpful in the diagnosis of HLH? 20% 1. 2. 3. 4. 5. 20% 20% 2 3 20% 20% Hemoglobin 8.4 g/dL Platelets 164 x 109/L Neutrophils 4.1 x 109/L Ferritin 11,900 mg/L sIL-2R 150 U/mL 1 4 5 What is the genetic association for secondary hemophagocytic lymphohistiocytosis? 20% 20% 20% 2 3 20% 20% 1. None 2. PRF1 3. UNC13D 4. Chediak-Higashi 5. I don’t know. 1 4 5 An 8 mo M is admitted to the PICU with a four day history of persistent fever and an erythematous rash. He is found to have hepatosplenomegaly, anemia, thrombocytopenia, and hyperferritonemia. You suspect this patient may have HLH. What is the best study to confirm this diagnosis? 1. 2. 3. 4. MRI Brain Lumbar puncture Genetic testing Bone marrow aspirate and biopsy 5. Abdominal ultrasound 20% 1 20% 20% 2 3 20% 4 20% 5 For patients with familial HLH, hematopoietic cell transplantation remains the only long-term curative treatment. 50% 50% 1.True 2.False 1 2 References • • • • • • • • • • • • • • • • • • Al Asad, O., et al. (2015). Alternative Therapy for Epstein-Barr Virus Related Hemophagocytic Lymphohistiocytosis. Case Reports in Oncological Medicine. Chandrakasan, S., et al. (2013). Hemophagocytic Lymphohistiocytosis: Advances in Pathophysiology, Diagnosis, and Treatment. The Journal of Pediatrics. Degar, B. (2015). Familial Hemophagocytic Lymphohistiocytosis. Hematology/Oncology Clinics of North America. Faitelson, Y., et al. (2014). Hemophagocytic lymphohistiocytosis and primary immune deficiency disorders. Clinical Immunology. Filipovich, A., et al. (2015). Pathogenesis of Hemophagocytic Lymphohistiocytosis. Hematology/Oncology Clinics of North America. Filipovich, A., et al. (2010). Histiocytic Disorders: Recent Insights into Pathophysiology and Practical Guidelines. American Society for Blood and Marrow Transplantation. Fitzgerald, N., et al. (2003). Imaging characteristics of hemophagocytic lymphohistiocytosis. Pediatric Radiology. Hamideih, A., et al. (2013). Fludarabine-based reduced-intensity conditioning regimen for hematopoietic stem cell transplantation in primary hemophagocytic lymphohistiocytosis. European Journal of Haematology. Henter, J.I., et al. (2007). HLH-2004: Diagnostic and Therapeutic Guidelines for Hemophagocytic Lymphohistiocytosis. Pediatric Blood & Cancer. Iwatani, S., et al. (2015). Familial Hemophagocytic Lymphohistiocytosis Presenting as Hydrops Fetalis. American Journal of Perinatal Reports. Jordan, M., et al. (2011). How I treat hemophagocytic lymphohistiocytosis. Blood. Jordan, M., et al. (2008). Hematopoietic cell transplantation for hemophagocytic lymphohistiocytosis: a journey of a thousand miles begins with a single (big) step. Bone Marrow Transplantation. Kanhere, S., et al. (2014). Hemophagocytic Lymphohistiocytosis Associated with Cytomegalovirus Infection in an Immunocompetent Infant: A Diagnostic and Therapeutic Challenge. Indian Journal of Hematology and Blood Transfusion. Khan, S., et al. (2015). Cerebellar swelling due to familial hemophagocytic lymphohistiocytosis: An unusual presentation. Official Journal of the European Paediatric Neurology Society. Lehmberg, K., et al. (2015). Consensus recommendations for the diagnosis and management of hemophagocytic lymphohistiocytosis associated with malignancies. Haematologica. Marsh, R., et al. (2013). Salvage Therapy of Refractory Hemophagocytic Lymphohistiocytosis with Alemtuzumab. Pediatric Blood & Cancer. Marsh, R, et al. (2010). Reduced-Intensity Conditioning Significantly Improves Survival of patients with hemophagocytic lymphohistiocytosis undergoing allogenic hematopoietic cell transplantation. Blood. McClain, K., et al. Clinical features and diagnosis of hemophagocytic lymphohistiocytosis. In: UpToDate, Boxer, L (Ed), UpToDate, Waltham, MA, 2015. References • • • • • • • • • • • • • • • • • McClain, E., et al. Treatment and prognosis of hemophagocytic lymphohistiocytosis. In: UpToDate, Boxer, L (Ed), UpToDate, Waltham, MA, 2015. Mellor-Heineke, S., et al. (2013). Elevated granzyme B in cytotoxic lymphocytes is a signature of immune activation in hemophagocytic lymphohistiocytosis. Frontiers in Immunology. Nathan, D., et al. (2015). Histiocytoses. In Nathan and Oski's hematology and oncology of infancy and childhood (8.th ed.). Philadelphia, Pa.: Elsevier. Nikiforow, S. (2015). The Role of Hematopoietic Stem Cell Transplantation in Treatment of Hemophagocytic Lymphohistiocytosis. Hematology/Oncology Clinics of North America. Ost, A., et al. (1998). Autopsy findings in 27 children with haemophagocytic lymphohistiocytosis. Histopathology. Palazzi, D., et al. (2003). Hemophagocytic Syndrome in Children: An Important Diagnostic Consideration in Fever of Unknown Origin. Clinical Infectious Disease. Pantanowitz, L., et al. (2007). Editorial comment: hemophagocytic syndrome—an HIV-associated quagmire. AIDS Read. Parvaneh, N., et al. (2013). Primary immunodeficiencies predisposed to Epstein-Barr virus-driven haematological diseases. British Journal of Haematology. Rahal, A., et al. (2015). Undiagnosed Systemic Lupus Erythematosus Presenting as Hemophagocytic Lymphohistiocytosis. Case Reports in Rheumatology. Ravelli, A., et al. (2015). Macrophage Activation Syndrome. Hematology/Oncology Clinics of North America. Roe, C., et al. (2015). Hemophagocytic Lymphohistiocytosis in Malignant Hematology: Uncommon but Should Not Be Forgotten? Clinical Lymphoma, Myeloma & Leukemia. Saeed, H., et al. (2015). Evaluating the optimal serum ferritin level to identify hemophagocytic lymphohistiocytosis in the critical care setting. International Journal of Hematology. Schulert, G., et al. (2015). Pathogenesis of Macrophage Activation Syndrome and Potential for Cytokine-Directed Therapies. Annual Review of Medicine. Sen, E., et al. (2015). Macrophage Activation Syndrome. Indian Journal of Pediatrics. Seo, J. (2015). Hematopoietic cell transplantation for hemophagocytic lymphohistiocytosis: recent advances and controversies. Blood Research. Trottestam, H., et al. (2011). Chemoimmunotherapy for hemophagocytic lymphohistiocytosis: long-term results of the HLH-94 treatment protocol. Blood. Trottestam, H., et al. (2011). Risk factors for early death in children with haemophagocytic lymphohistiocytosis. Acta Pediatrica. Thanks for listening! Any questions? Thank you!