THE EFFECTS OF DIETARY FAT INTAKE ON RESTING ENERGY
EXPENDITURE AND BODY COMPOSITION
A Thesis
Presented to the faculty of the Department of Kinesiology
California State University, Sacramento
Submitted in partial satisfaction of
the requirements for the degree of
MASTER OF SCIENCE
in
Kinesiology
(Exercise Science)
by
Nichole Mi Hui Eytcheson
SPRING
2012
© 2012
Nichole Mi Hui Eytcheson
ALL RIGHTS RESERVED
ii
THE EFFECTS OF DIETARY FAT INTAKE ON RESTING ENERGY
EXPENDITURE AND BODY COMPOSITION
A Thesis
by
Nichole Mi Hui Eytcheson
Approved by:
__________________________________, Committee Chair
Roberto Quintana, PhD
__________________________________, Second Reader
Wendy Buchan, PhD
____________________________
Date
iii
Student: Nichole Mi Hui Eytcheson
I certify that this student has met the requirements for format contained in the University format
manual, and that this thesis is suitable for shelving in the Library and credit is to be awarded for
the thesis.
__________________________, Graduate Coordinator
Michael Wright, PhD
Department of Kinesiology
iv
__________________
Date
Abstract
of
THE EFFECTS OF DIETARY FAT INTAKE ON RESTING ENERGY
EXPENDITURE AND BODY COMPOSITION
by
Nichole Mi Hui Eytcheson
Statement of Problem
Whether changing from a high-fat diet to an isoenergetic, low-fat, high- complexcarbohydrate diet results in thermogenic benefits is controversial. Brief dietary
interventions and failure to account for the potential influence of body-fat distribution on
energy metabolism could have confounded the interpretation of previous studies. The
success of individuals who lose weight by changing from high fat diets to low-fat diets
has prompted numerous, well-controlled studies of this phenomenon. The literature
regarding a thermogenic effect of low-fat, high-CHO diets reveals conflicting evidence.
The present study was designed to answer the following questions; 1) Does dietary fat
restriction increase the caloric need to maintain weight? 2) Does lowering the fat intake
in the diet affect resting energy expenditure (REE)? 3) Does dietary fat restriction affect
body composition?
Methods
Sixty-four healthy post menopausal women were recruited to the study and enrolled
in four cohorts of 16 participants every 4 months. Each cohort went under 3 dietary
v
interventions over a 4 month period. Dietary intervention involved a 4-month long
eucaloric controlled-feeding that was designed to reduce the fat intake stepwise to 15% of
the daily energy intake. Bioelectrical impedance (BIA) was used to assess body
composition and provide values for FFM and FM. REE was collected using indirect
calorimetry and calculated using the Weir equation. Data were expressed as means +
standard deviations (SD).
Results
The four dietary interventions did not alter REE (p=.979). There was a trend for
an increased respiratory exchange ratio with the low-fat diet (p=.067). Although the
controlled-feeding phase was designed by calculated, computer generated analysis to
deliver 35%, 25% and 15% of the energy intakes from fat, laboratory and chemical
analysis of the diet showed that the actual dietary fat intakes were 31%, 23% and 14%
respectively. There was a significant difference in body weight (0.9 kg) between baseline
and after the 35% fat diet (p=0.0003), no significant change between the 35% and 25%
fat diet (0.05 kg, p=0.218), and no significant change between the 25% fat diet and the
15% fat diet (0.05 kg, p=0.156). During the eucaloric feeding as dietary fat decreased
from 31 % to 23% to 14 %, the energy cost of weight maintenance increased from
8724+1281 kJ, to 8946+ 1310 kJ, and to 9122+ 1365 kJ, respectively. These increases
were significant (+223+400 kJ, p< 0.02 and +398+638 kJ, p < 0.0001 ). There was a
significant decrease in body fat (kg), fat mass (kg), and fat free mass (kg) after the 35%
fat eucaloric feeding (p=0.033, 0.0008, 0.0001) respectively. There was no significant
vi
difference between the 25% fat (p=0.297, 0.224, 0.419) and 15% fat feeding (p=0.079,
0.147, 0.177).
Conclusions Reached
Our results demonstrate that restriction of fat intake increases the energy cost of
weight maintenance (ECWM), has no effect on REE or RER, and caused small
differences on FM, FFM, and BF. Given the evidence that carbohydrate is 25% less
efficiently utilized by the body, one could speculate that a person could consume 25%
more calories in CHO than fat without gaining weight. While the study also failed to
demonstrate any change in REE, this suggests that the increase in energy expenditure
must likely occurs post-prandially. While the study controlled for body composition
using a eucaloric diet, decreases in FFM, FM, and BF were observed. In summary, the
present study supports that low-fat intake increases the ECWM and reduces body lipid
stores. It appears that low-fat intake can improve risk factors for coronary artery disease,
such as dyslipidemia, decreases risk of diabetes and obesity, and results in weight loss
without food deprivation. Therefore, it seems prudent to suggest restriction of dietary fat
especially in an obese post-menopausal female population.
_______________________, Committee Chair
Roberto Quintana, PhD
_______________________
Date
vii
ACKNOWLEDGEMENTS
I would like to thank and acknowledge not only the people who helped me to
complete this thesis, but supported me in the process. The completion of my Master’s
course work along with this thesis would not have been attainable without everyone. I
would like to thank my family, teachers, and friends for all your support.
First, and foremost, I would like to thank my parents. Without their love, support
and guidance I know I would not have accomplished all that I have today. I strive to be
the best because of you, and I thank that you instilled the importance of education in me
since I was a little girl. Thank you so much for believing in me and helping me attain all
my aspirations. You are the best parents and have given me the opportunity to be my
best. I love you so much!
To my fiancé, thank you for helping me make it through the long hours of
commuting, studying, and countless hours working on my coursework and thesis. You
have made my life so much easier being there and supporting me through it all. I cannot
thank you enough for keeping me level headed and the encouragement you have given
me throughout the process. There is not a day that goes by that I don’t thank you for all
that you are.
To the faculty, Dr. Roberto Quintana and Wendy Buchan, your guidance and
support throughout this thesis has been more than I can ask. In the midst of my busy life,
you have helped attain my degree and for that I will be forever grateful. I am lucky to
have found such great faculty support in this program. I cannot say thank you enough!
viii
TABLE OF CONTENTS
Page
Acknowledgments…………………………………………………………………… viii
List of Tables…………………………………………………………………………. xii
List of Figures…………………………………………………………………………xiii
Chapter
1. INTRODUCTION …………….. ………………………………….……………... 1
Statement of Purpose………………………………………………………….. 3
Significance of Thesis………………………………………………………… 3
Definition of Terms…………………………………………………………… 3
Limitations……………………………………..………………………………4
Delimitations………………………..………………………………………….5
Assumptions……………..……………………………………………………..5
Hypotheses……………….…………………………………………………….5
2. REVIEW OF LITERATURE……………………………………………………... 6
Resting Energy Expenditure Methodology…………………………………… 6
Effects of Fats and Carbohydrates on Resting Energy Expenditure………….. 7
Increase in Caloric Need on a Low-Fat Diet…………….……………………11
No Increase in Caloric Need on a Low-Fat Diet….…………………………..12
Macronutrient Composition…………………….…………………..………...14
Body Composition on a Low-Fat Diet…….……………………………….…15
Summary……………………….……………………………………………..17
3. METHODOLOGY……………….………………………….………………….. .19
Subjects…………………….………………………………………………….19
Experimental Design………………………………………………………….20
Data Analysis………………………………………………………………....24
4. RESULTS……………………………………………………………………..…. 25
Resting Energy Expenditure and Respiratory Quotient…………………........25
Changes in Nutrient Intake……………………………………………………25
ix
Energy and Dietary Fat Intake………………………………..…………….25
Energy Cost of Weight Maintenance………………………..……………...26
Changes in Weight…………………………………..……………………...26
Percent Body Fat, Fat Mass, and Fat Free Mass…………………...……….27
5. DISCUSSION…………...……………………………………………………….37
Future Research………….…………..…………………………...…………40
Conclusion……………….…………………..…………………...…………41
REFERENCES………………………………………………………………..…… .42
x
LIST OF TABLES
Tables
1.
Page
Table 1. Changes in weight, percent body fat, daily energy intake, resting
energy expenditure, respiratory quotient, fat mass, and fat free mass
during eucaloric restriction of dietary fat intake……………………….28
2.
Table 2. Differences in analysis of dietary energy, fat, and carbohydrate
of the same 7 day menu cycles by Hazelton Laboratories, Nutritionist IV,
and Nutrition Data Systems…………………………………………….29
xi
LIST OF FIGURES
Figures
1.
Page
Figure 1. Effects of Resting Energy Expenditure (REE) with dietary fat
restriction………………………..……………………………………......31
2.
Figure 2. Effects of Respiratory Quotient (RQ) with dietary fat
restriction………………………………………………………….….......32
3.
Figure 3. Effects of Body Weight (BW) with dietary fat restriction. …....33
4.
Figure 4. Effects of Fat Free Mass (FFM) with dietary fat restriction..….34
5.
Figure 5. Effects of Fat Mass (FM) with dietary fat restriction…………..35
6.
Figure 6. Effects of Body Fat (BF) with dietary fat restriction………......36
xii
1
CHAPTER 1
Introduction
The health benefits of adopting an isoenergetic, low-fat, high- complexcarbohydrate diet are controversial. From the patient’s perspective, an ideal treatment of
obesity would permit generous food intake and yet result in the loss of body fat without
the discomfort and inconvenience of exercise. Although pharmacologic approaches
toward increasing energy expenditure are under investigation, modifying the diet
composition to achieve the same goals has more inherent appeal. The success of
individuals who lose weight by changing from high fat diets to low-fat diets has
prompted numerous, well-controlled studies of this phenomenon. High-carbohydrate,
low-fat diets have been shown to reduce energy intake (Lissner, Levitsky, Strupp,
Kalkwarf, & Roe 1987) and confer thermogenic benefits. Not all studies have found
benefits, as measured by weight loss (Leibel, Hirsch, Appel, & Checani, 1992) or
increased energy expenditure (Abbott, Howard, Ruotolo, & Ravussin, 1990) in response
to low-fat, high-carbohydrate, isocaloric diets, however.
Prior research has suggested that low-fat, high-carbohydrate (CHO) diets
increases weight loss (Abbot et al., 1990; Astrup, Buemann, Christensen, Madsen, 1994;
Barrett-Connor, Friedlander, 1993; Cunningham, 1980). In fact, for weight loss purposes,
low-fat intake is as effective and more satisfying when compared to diets maintaining the
usual fat intake and restricting the amount of food (Astrup et al., 1994). There are two
factors that support this claim. First, CHO-rich foods have lower caloric density, and
2
therefore, a larger volume. This leads to a natural restriction of energy intake without the
discomfort of food deprivation. Secondly, High-CHO foods may be thermogenic. While
the energy cost of depositing dietary fat in the adipose tissue is minimal, dietary CHO
needs to be first converted to triglycerides for storage. The energy cost of this process is
approximately 25% of the energy obtained from CHO (Hegsted, Ausman, Johnson,
Dallal, 1993). Therefore, when the same amount of energy is as CHO, instead of fat, 25%
less energy is deposited in the adipose tissue. Between these two explanations the former
has gained a wider acceptance. Although the latter explanation has a solid biochemical
foundation, it remains controversial.
The literature regarding a thermogenic effect of low-fat, high-CHO diets reveals
conflicting evidence. Several studies have demonstrated an increase in the energy cost of
weight maintenance with low-fat diets (Barrett-Connor & Friedlander, 1993; Hegsted et
al., 1993; Leibel et al., 1992). Other studies have failed to find any change in energy
expenditure on low-fat diets (Lissner et al., 1987; Martin, Su, Jones, Lockwood,
Tritchler, Boyd, 1996). Given the biochemical basis for an increase in energy expenditure
with high-CHO, low-fat diets, further research is needed to establish the reason for such
equivocal findings.
Therefore the body of evidence indicates that there are likely benefits of a low fat
with regard ECWM, body composition, and REE. If we are able to demonstrate that low
dietary fat intake can increase the energy cost of weight maintenance, and induce
beneficial body composition changes this would clarify the efficacy of a low fat diet in a
post-menopausal female population.
3
Statement of Purpose
The present study was designed to answer the following three questions; 1) Does
dietary fat restriction increase the caloric need to maintain weight? 2) Does lowering the
fat intake in the diet affect resting energy expenditure (REE)? 3) Does dietary fat
restriction affect body composition?
Significance of Thesis
Prior research has examined the impact of resting energy expenditure and body
composition on a eucaloric diet, but few studies have assed the relationship in
postmenopausal women. Additionally, no study has examined the relationship of energy
cost of weight maintenance, resting energy expenditure, and body composition in
postmenopausal women, both obese and non obese.
Definition of Terms
Amenorrhoea: No menstruation for more than 9 months (Mosby’s Medical Dictionary).
Bioelectrical Impedance Analysis (BIA): A technique to estimate body composition
based on the difference in electrical conductive properties of various tissues.
Body Composition: The relative amount of fat-free mass and fat mass of the body.
Body Mass Index (BMI): Describes relative weight for height, and is calculated by
dividing body mass in kilograms by height in meters squared (Expert panel on the
identification, evaluation, and treatment of overweight in adults, 1998).
Fat Mass (FM): A measure of the amount of lipid content of the body.
Energy Cost of Weight Maintenance (ECWM): Energy intake required to maintain body
weight and prevent weight loss.
4
Fat-Free Mass (FFM): A measure of the total body mass, including water, protein and
mineral content of the human body.
Respiratory Exchange Ration (RER): The ratio of the volume of carbon dioxide produced
to the volume of oxygen consumed in respiration over a period of time.
Resting Energy Expenditure (REE): The resting daily energy expended in a fasted state
under a neutral environment (Sims & Danforth, 1986).
Limitations
1. Fitness level (measured by VO2 max) and its effects on REE were not controlled.
2. Physical activity levels were not controlled.
3. The REE coefficient of variation using indirect calorimetry is 3.6%
4. Diet interventions were not randomized and the order effects of dietary manipulation
were not controlled.
5. The study was not blinded. Therefore, the subjects and investigators were aware of the
daily treatments.
Delimitations
1. The impact of family influence was not monitored.
2. Subjects were limited to the Sacramento area.
3. Subjects were limited to females.
4. Subjects were limited to postmenopausal women between the ages of 43 & 81.
5. ECWM values were adjusted monthly prior to the beginning of each dietary
intervention period.
5
Assumptions
1. Subjects adhered to the pretest instructions prior to laboratory testing.
2. Each subjects’ REE test reflected their true REE.
3. Participants were honest about self-reported activity levels.
4. Subjects’ weight gain or loss is due to changes in an energy source from carbohydrate,
fat, or protein.
Hypotheses
1. Total caloric need (ECWM) will not change in response to a reduced dietary lipid
composition of an eucaloric diet.
2. A reduction in dietary lipid composition of an eucaloric diet will not alter body
composition.
3. A reduction in dietary lipid composition of an eucaloric diet will not alter REE
6
CHAPTER 2
Review of Literature
The prevalence of obesity in the adult population in American society has reached
epidemic proportions (World Health Organization, 1998). As a result of the obesity
epidemic, researchers around the world have begun to look at the effect of resting energy
expenditure and body composition. REE comprises 75% of our daily energy expenditure,
therefore researchers are looking to individuals to see a relationship between obesity and
lower resting metabolic rates, in hopes of prescribing a low-fat diet to induce weight loss
and a decrease in body composition. This chapter provides a description of resting energy
expenditure and reviews the effects of energy cost of weight maintenance and body
composition on a low-fat diet.
Resting Energy Expenditure Methodology
Resting energy expenditure (REE) is the number of calories utilized at rest and
makes up two-thirds of all the energy expended in one day. The term REE is commonly
used interchangeably with resting metabolic rate (RMR) and basal metabolic rate (BMR).
Resting energy expenditure represents the largest percentage of an individual’s daily
energy expenditure which is why many researchers have been interested in REE adaptive
responses to different dietary and physical activity interventions.
A reduction in body weight can be achieved by decreasing caloric intake or to
increase physical activity expenditure to induce a negative caloric deficit (Hill, 2006).
With dietary restriction, an appropriate and accurate caloric deficit must be calculated for
7
a successful weight loss program. This can be done with knowledge of an individual’s
REE. An accurate method to measure REE is utilizing indirect calorimetry (Compher,
Frankenfield, Keim, Roth-Yousey, 2006).
Effects of Fats and Carbohydrates on Resting Energy Expenditure
Brehm, Seeley, Daniels, D’Alessio (2003) designed a randomized, controlled trial
to determine the effects of a very low carbohydrate diet on body composition and
cardiovascular risk factors. Subjects were randomized to 6 months of either an ad
libitum very low carbohydrate diet or a calorie-restricted diet with 30% of the calories as
fat. Anthropometric and metabolic measures were assessed at baseline, 3 months, and 6
months. Fifty-three healthy, obese female volunteers (mean body mass index, 33.6 ± 0.3
kg/m2) were randomized; 42 (79%) completed the trial. Women on both diets reduced
calorie consumption by comparable amounts at 3 and 6 months. The very low
carbohydrate diet group lost more weight (8.5 ± 1.0 vs. 3.9 ± 1.0 kg; P < 0.001) and more
body fat (4.8 ± 0.67 vs. 2.0 ± 0.75 kg; P < 0.01) than the low fat diet group. Mean levels
of blood pressure, lipids, fasting glucose, and insulin were within normal ranges in both
groups at baseline. Although all of these parameters improved over the course of the
study, there were no differences observed between the two diet groups at 3 or 6 months.
Based on these data, a very low carbohydrate diet is more effective than a low fat diet for
short-term weight loss and may increase resting energy expenditure (Brehm, et al. 2003).
The energy to metabolize fats and carbohydrates may affect weight loss in this ad libitum
carbohydrate group and caloric restricted fat group. The possibility that differences in the
8
macronutrient composition of the diet alter energy expenditure bears further
investigation.
Volek, Sharman, Gómez, Judelson, Rubin, et al. (2004) looked to compare the
effects of isocaloric, energy-restricted very low-carbohydrate ketogenic (VLCK) and
low-fat (LF) diets on weight loss, body composition, trunk fat mass, and resting energy
expenditure (REE) in overweight/obese men and women. 15 healthy, overweight/obese
men and 13 premenopausal women were prescribed two energy-restricted (-500 kcal/day)
diets: a VLCK diet with a goal to decrease carbohydrate levels below 10% of energy and
induce ketosis and a LF diet with a goal similar to national recommendations
(%carbohydrate:fat:protein = ~60:25:15%). The authors discovered that dietary energy
was restricted, but was slightly higher during the VLCK (1855 kcal/day) compared to the
LF (1562 kcal/day) diet for men. Both between and within group comparisons revealed a
distinct advantage of a VLCK over a LF diet for weight loss, total fat loss, and trunk fat
loss for men (despite significantly greater energy intake). The majority of women also
responded more favorably to the VLCK diet, especially in terms of trunk fat loss. The
greater reduction in trunk fat was not merely due to the greater total fat loss, because the
ratio of trunk fat/total fat was also significantly reduced during the VLCK diet in men
and women. Absolute REE (kcal/day) was decreased with both diets as expected, but
REE expressed relative to body mass (kcal/kg), was better maintained on the VLCK diet
for men only. Individual responses clearly show the majority of men and women
experience greater weight and fat loss on a VLCK than a LF diet. This study shows a
clear benefit of a VLCK over LF diet for short-term body weight and fat loss, especially
9
in men. A preferential loss of fat in the trunk region with a VLCK diet is novel and
potentially clinically significant but requires further validation. These data provide
additional support for the concept of metabolic advantage with diets representing
extremes in macronutrient distribution (Volek et al. 2004).
Brehm, Spang, Lattin, Seeley, Daniels et al. (2005) reported that obese women
randomized to a low-carbohydrate diet lost more than twice as much weight as those
following a low-fat diet over 6 months. The difference in weight loss was not explained
by differences in energy intake because women on the two diets reported similar daily
energy consumption. They hypothesized that chronic ingestion of a low-carbohydrate diet
increases energy expenditure relative to a low-fat diet and that this accounts for the
differential weight loss. Fifty healthy, moderately obese (body mass index, 33.2 ± 0.28
kg/m2) women were randomized to 4 months of an ad libitum low-carbohydrate diet or an
energy-restricted, low-fat diet. Resting energy expenditure (REE) was measured by
indirect calorimetry at baseline, 2 months, and 4 months. Physical activity was estimated
by pedometers. The thermic effect of food (TEF) in response to low-fat and lowcarbohydrate breakfasts was assessed over 5 h in a subset of subjects. The lowcarbohydrate group lost more weight (9.79 ± 0.71 vs. 6.14 ± 0.91 kg; P < 0.05) and more
body fat (6.20 ± 0.67 vs. 3.23 ± 0.67 kg; P < 0.05) than the low-fat group. There were no
differences in energy intake between the diet groups as reported on 3-day food records at
the conclusion of the study (1422 ± 73 vs. 1530 ± 102 kcal; 5954 ± 306 vs. 6406 ± 427
kJ). Mean REE in the two groups was comparable at baseline, decreased with weight
loss, and did not differ at 2 or 4 months. The low-fat meal caused a greater 5-h increase in
10
TEF than did the low-carbohydrate meal (53 ± 9 vs. 31 ± 5 kcal; 222 ± 38 vs. 130 ± 21
kJ; P = 0.017). These results confirm that short-term weight loss is greater in obese
women on a low-carbohydrate diet than in those on a low-fat diet even when reported
food intake is similar. The differential weight loss is not explained by differences in REE,
TEF, or physical activity and likely reflects underreporting of food consumption by the
low-fat dieters (Brehm, et al. 2005).
Abbot et al., (1990) studied the effects of fat and carbohydrate on resting energy
expenditure. They determined a high-dietary fat intake may be an important
environmental factor leading to obesity in some people. The mechanism could be either a
decrease in energy expenditure and/or an increase in caloric intake. To determine the
relative importance of these mechanisms they measured 24-h energy expenditure in a
whole body calorimeter in 14 nondiabetic subjects and in six subjects with non-insulindependent diabetes mellitus, eating isocaloric, weight-maintenance, high-fat, and highcarbohydrate diets. In nondiabetics, the mean total 24-h energy expenditure was similar
(2,436 +/- 103 vs. 2,359 +/- 82 kcal/day) on high-fat and high-carbohydrate diets,
respectively. The means for sleeping and resting metabolic rates, thermic effect of food,
and spontaneous physical activity were unchanged. Similar results were obtained in the
diabetic subjects. In summary, using a whole body calorimeter, researchers found no
evidence of a decrease in 24 hour energy expenditure on a high-fat diet compared with a
high-carbohydrate diet.
11
Increase in Caloric Need on a Low-Fat Diet
A review by Bray and Popkin, 1998, found 28 intervention studies where subjects
were asked to reduce dietary fat without energy restriction. There was an average weight
loss of 1.6 g/day for each 1% reduction in dietary fat. The meta-analysis reports an
unpublished study by Astrup, indicating that in 15 of 16 identified studies, reducing
dietary fat led to a greater, yet modest decrease in body weight (2.5 kg, 95% confidence
interval 5 1.5–3.5 kg, P , 0.0001) compared with the control groups. There were
significant positive correlations between the reduction in dietary fat and amount of
weight loss (r = 0.37) and between initial body weight and weight loss (r = 0.52) (Bray &
Popkin, 1998). These results could be explained by the mechanism of a higher metabolic
cost to convert carbohydrate to lipid stores. Carbohydrates are more thermogenetic. The
energy cost to deposit dietary fat into adipose tissue is minimal, whereas dietary
carbohydrates must first be first converted to triglycerides for storage. This energy cost
may be the reason weight loss is observed on a low-fat, high-carbohydrate diet.
Horton, Drougas, Brachey, et al. (1995) overfed lean and obese men 50% of their
energy requirement either as CHO or fat. When the excess energy was provided as CHOcalories, CHO-oxidation and energy expenditure increased, with a net of 75-85% of the
excess energy used for storage. Fat overfeeding did not stimulate either fuel oxidation or
energy expenditure, resulting in the storage of 90-95% of the excess energy. Astrup et al.
(1994) demonstrated that when isocaloric diets containing 20%-fat verses 50%-fat are
administered, each for 3 days, there was a 4% increase in daytime energy expenditure on
the low-fat diet (8,090 kJ/d to 8,401 kJ/d) and an +11 g/day fat deposition. On the high-
12
fat diet day time energy expenditure did not change (8,034 verses 8,086 kJ/d) and the fat
deposition was larger (+19.6 gm/d). Interestingly these changes were observed only in
post-obese women, but not in the never-obese controls. There might be a change in
metabolism in obese verse non obese subjects, but this bears further investigation.
No Increase in Caloric Need on a Low-Fat Diet
With some studies supporting an increase in ECWM on low-fat diets, there are
also several reports of no change. Roust, Hammel, & Jensen (1994) did not show any
change in body composition, overnight energy expenditure, REE or fat oxidation between
the 42%-fat (to stabilize weight) and 27%-fat diets in a 4 week intervention. This brief
dietary intervention could confound their interpretation. This study also did not use a
very low-fat diet, although the change was large. In addition, only the overnight REE, but
not the 24-hour total energy expenditure, were measured. Hill, Sparling, Shields, &
Heller, (1987) compared the effects of 60% CHO verses 60%-fat diets for 7 days each
and found that while there was no change in the energy expenditure, there was a change
in the nutrient oxidation, which reflected the dietary composition. Lean & James (1988)
investigated lean, obese and post-obese women on high CHO (3% fat and 45 % CHO)
versus low CHO (40% fat and 12% CHO) diets and found no significant difference in
total 24 hour energy expenditure between the diets or groups but a significantly higher
thermal effect of food on the high carbohydrate versus the low carbohydrate diet (5.8%
vs. 3.5%, respectively). Abbott et al. (1990) also found no difference in 24 hour energy
expenditures in 14 Pima Indians on a 20% versus 44% fat diet (2,436 + 103 vs. 2,359 +
82); however, an increase in the 24 hour RQ was noted with the shift from dietary fat to
13
dietary CHO. Again Abbott had a small number of subjects which may have limited the
statistical power to report a significant increase in the ECWM. Stubbs, William, Coward,
& Prentice (1995) demonstrated that when diets containing 20%, 40% and 60% fat were
compared, there was a direct relationship between the fat and energy intakes. While there
was no change in measured energy expenditure, 20%-fat and 40%-fat diets caused weight
loss, relative to the 60%-fat diet. Since weight loss leads to a lower lean body mass, this
may lower resting energy expenditure and limit weight loss reported. While these studies
did not show an increase in the ECWM on low-fat diets, this inconsistency in results may
be explained by differences in study design. Some differences in study designs included
different dietary composition, liquid diets versus solid foods (both amounts and types of
fats & carbohydrates used), different endpoints measured, small number of subjects in
some studies, and different subject composition (different ages, body compositions and
background diets).
Prewitt, Schmeisser, Bowen, Aye, Dolecek, Langenberg, Cole & Brace (1991)
showed that when 18 women were switched from a 37%-fat diet to a 20%-fat diet for 20
weeks, ECWM increased by 19% (7515 + 140 vs 9083 + 373 kJ/day) and these women
lost 2.8% body weight despite efforts to maintain weight. Leibel et al., (1995)
investigated diets rich in fat that may promote greater deposition of adipose-tissue
triglycerides than do isoenergetic diets with less fat. This possibility was examined by a
retrospective analysis of the energy needs of 16 human subjects (13 adults, 3 children)
fed liquid diets of precisely known composition with widely varied fat content, for 15-56
d (33 +/- 2 d, mean +/- SE). Subjects lived in a metabolic ward and received fluid
14
formulas with different fat and carbohydrate content, physical activity was kept constant,
and precise data were available on energy intake and daily body weight. Isoenergetic
formulas contained various percentages of carbohydrate as cerelose (low, 15%;
intermediate, 40% or 45%; high, 75%, 80%, or 85%), a constant 15% of energy as
protein (as milk protein), and the balance of energy as fat (as corn oil). Even with
extreme changes in the fat- carbohydrate ratio (fat energy varied from 0% to 70% of total
intake), there was no detectable evidence of significant variation in energy need as a
function of percentage fat intake.
Macronutrient Composition
Sacks, Bray, Carey, Smith, Ryan et al. (2009) randomly assigned 811 overweight
adults to one of four diets; the targeted percentages of energy derived from fat, protein,
and carbohydrates in the four diets were 20, 15, and 65%; 20, 25, and 55%; 40, 15, and
45%; and 40, 25, and 35%. The participants were offered group and individual
instructional sessions for 2 years. The primary outcome was the change in body weight
after 2 years in two-by-two factorial comparisons of low fat versus high fat and average
protein versus high protein and in the comparison of highest and lowest carbohydrate
content. The authors concluded that a reduced-calorie diet results in clinically meaningful
weight loss regardless of which macronutrients they emphasize (Sacks, et al. 2009).
Body Composition on a Low-Fat Diet
The idea of body weight regulation implies that a biological mechanism exerts
control over energy expenditure and food intake. This is a central tenet of energy
homeostasis. However, the source and identity of the controlling mechanism have not
15
been identified, although it is often presumed to be due to gastro-intestinal adipose
endocrine signaling areas of the brain governing appetite, satiety, and energy homestasis.
In a recent study, Blundell, Caudwell, Gibbons, Hopkins, Naslund, King, and Finlayson
(2011), using a comprehensive experimental platform, investigated the relationship
between biological and behavioral variables in two separate studies over a 12-week
intervention period in obese adults. All variables have been measured objectively and
with a similar degree of scientific control and precision, including anthropometric
factors, body composition, REE and accumulative energy consumed at individual meals
across the whole day. Results showed that meal size and daily energy intake (EI) were
significantly correlated with fat-free mass (FFM, P values < 0·02-0·05) but not
with fat mass (FM) or BMI (P values 0·11-0·45) (study 1, n=58). In study 2 (n=34), FFM
(but not FM or BMI) predicted meal size and daily EI under two distinct dietary
conditions (high-fat and low-fat). These data appear to indicate that, under these
circumstances, some signal associated with lean mass (but not FM) is related to selfselected food consumption. This signal may be postulated to interact with a separate class
of signals generated by FM. This finding may have implications for investigations of the
molecular control of food intake and body weight and for the management of obesity
(Blundell, et al 2011).
In a study by Noakes, Keogh, Foster, and Clifton (2005), researchers wanted to
evaluate the effects of a diet with a high ratio of protein to carbohydrate during weight
loss on body composition in overweight women. The subjects were randomly assigned to
1 of 2 isocaloric 5600-kJ dietary deficit interventions for 12 wk according to a parallel
16
design: a high-protein (HP) or a high-carbohydrate (HC) diet. One hundred women with a
mean (±SD) body mass index (in kg/m2) of 32 ± 6 and age of 49 ± 9 y completed the
study. Weight loss was 7.3 ± 0.3 kg with both diets. Subjects with high serum
triacylglycerol (>1.5 mmol/L) lost more fat mass with the HP than with the HC diet (
± SEM: 6.4 ± 0.7 and 3.4 ± 0.7 kg, respectively; P = 0.035). They concluded that an
energy-restricted, high-protein, low-fat diet provides nutritional and metabolic benefits
that are equal to and sometimes greater than those observed with a high-carbohydrate
diet. It is important to note that a limitation of this study is that a HP diet is the least
efficient macronutrient. These diets induced more weight loss initially due to fluid loss
but the body adjusts by retaining more body water and hence higher FFM.
Summary
In summary, the literature suggesting that low-fat, high-carbohydrate (CHO) diets
promoting weight loss are supported by the thermogenic effect of low-fat, high-CHO
diets. In fact, for weight loss purposes low-fat intake is as effective and more satisfying
when compared to diets maintaining the usual fat intake and restricting the amount of
food. While the energy cost of depositing dietary fat in the adipose tissue is minimal,
dietary CHO needs to be first converted to triglycerides for storage. The energy cost of
this process is approximately 25% of the energy obtained from CHO (Hegsted et al.,
1993). Therefore, when the same amount of energy is as CHO, instead of fat, 25% less
energy is deposited in the adipose tissue. In most studies reviewed, macronutrient
composition had no effect on REE. When body composition was effected, it was noticed
in the obese population. This might indicate that changes in metabolism are occurring in
17
an obese verses non obese population. Given the biochemical basis for an increase in
energy expenditure with high-CHO, low-fat diets, further research is needed to establish
the reason for such controversy in the literature.
18
CHAPTER 3
Methodology
The purpose of this study was to examine the effects of dietary fat restriction on
the energy intake required to maintain body weight, and weight loss (ECWM). The study
also investigated resting energy expenditure (REE), and body composition, including
FM, FFM, and BF, in post menopausal women.
Subjects
Sixty-four healthy post menopausal women were recruited to the study after
signing the informed consents approved by the Institutional Human Investigation
Committee of the University of California, Davis. All participants were examined by the
principal investigator and chemistry-20 panels were obtained during fasting. Individuals
with diabetes mellitus, liver or kidney disease, or who had plasma triglyceride above 2.82
mM/L or LDL-cholesterol above 4.26 mM/L were excluded. Menopause was defined by
at least 9 months history of amenorrhea or surgical removal of both ovaries. Only women
who were menopausal or taking continuous hormone replacement therapy were included.
Women on cyclical hormone replacement were excluded. Twenty-four women used
hormone replacement; 14 estrogen only, and 10 combination of estrogen and
progesterone. The dose of the hormones and all the other medications or supplements
remained unchanged throughout the study. The physical activity levels were maintained
and monitored by activity questionnaires. Four women were excluded from the study
during the controlled feeding phase due to non-compliance. Eight women failed to
19
complete the four month protocol. The remaining 56 (age = 58.4 ± 7.7 years, Mean+S.D.)
completed the entire study. Upon re-evaluation of the study, complete data was obtained
from 38 subjects (age = 59.2 ± 9.1, Mean+S.D.).
Experimental Design
Four cohorts of 16 participants were enrolled every 4 months. Each cohort went
under 3 dietary interventions over a 4 month period. Dietary interventions were
administered in a sequential order. Pre and post testing were administered at the
beginning and end of each dietary intervention.
Dietary Intervention
Dietary intervention involved a 4-month long eucaloric controlled-feeding which
provided all the food. The study was designed to reduce the fat intake stepwise to 15% of
the daily energy intake. Participants’ diet prior to the study was defined as “the habitual
diet.” The habitual diet was determined by having participants keep a 7 day food diary,
which was reviewed with a dietitian. For the eucaloric controlled-feeding, participants ate
their dinners, 5 days a week at the study site, and received their breakfasts, lunches,
snacks and weekend meals in pre-packaged form as take-outs. The food was prepared in
7-day menu cycles in the study kitchen. The ingredients were weighed to the nearest
gram. The trays were inspected to assure complete consumption of the food. Participants
were required to return any unconsumed food and record any foods eaten not provided by
the study. They were to call the study coordinator immediately if any food was lost or
missing which would be replaced. After entering the study participants consumed a 35%fat diet during the first four weeks. The goal was to bring all the participants to the same
20
fat intake level and adjust the energy intake to maintain weight as a preparation to low-fat
diet phases. During this period, the initial energy intake was individualized based on each
subject’s resting energy expenditure (measured by indirect calorimetry) and multiplied by
a factor based on their physical activity level (estimated by physical activity
questionnaire). The physical activity questionnaire was a sheet of paper that asked
subjects to document their physical activity each week. Subjects were weighed 5 times
each week and the energy content of the diet was adjusted when weight varied by more
than 1 kg, from the entry level, in order to maintain the initial body weight. After
stabilizing the weight and energy intake during the 35%-fat period, participants were
switched to a diet containing 25%-fat for six weeks, and then 15%-fat for another six
weeks. Participants kept daily records of any additional dietary intake of uneaten foods.
Non-compliance was defined as more than 1% of calories altered from the experimental
diet on more than one occasion. Alcohol was not included in the diet. One alcoholic drink
per week was permitted as long as the intake was recorded in the food diary. The
majority of women did not consume any alcohol. Food from an entire week during each
diet period was homogenized and sent to the Hazelton Laboratory (Madison, WI) for
analysis. Actual fat contents of the diets were reported as 31%, 23% and 14%, and
carbohydrate contents as 53%, 60%, and 67%, respectively. This was compared to
analysis of the 7-day diet cycles analyzed by a registered dietitian on both Nutrition Data
System (NDS 93, University of Minnesota) and Nutritionist IV.
21
Body composition
Bioelectrical impedance (BIA) was used to assess body composition and provide
values for FFM and FM. BIA is a simple, inexpensive, and noninvasive method of
measuring body composition (Gallagher & Song, 2003; Segal, Van Loan, Gitzgeral,
Hodgdon & Van Itallie, 1988). BIA assessed body composition in the past absorptive
state by passing 800 μA alternating current at 50 kHz from the right hand to the
ipsilateral foot while the subject remained supine (Biostat 1500, British Isles,
BioAnalogics-HMS1000, Beaverton, OR). Sigal et al. (1998) found that the estimation of
FFM by BIA was reliable, and the precision of the measurement increased when
population specific equations were used. Heyward & Wagner (2004) suggest the use of
the following equations published by Segal et al. (1988): FFM [FFM = 0.00091186 x
height2 (cm2) – 0.001466(impedance) + 0.2999 x body weight (kg) – 0.07012 x age
(years) + 9.37938], FM [FM = weight (kg) – FFM], and percent body fat [percent body
fat = FM (kg)/weight (kg) x 100]. The multiple correlation coefficient between
densitometrically determined FFM which predicted by BIA is 0.93 and the standard error
of estimate (SEE) was 1.95 kg for FFM (Chapman, Bannerman, Cowen, & Maclennan,
1998). The correlation between densitometrically determined percent body fat and
predicted percent body fat was 0.91 and the SEE was 3.18% (Segal et al., 1988).
22
Physical Activity
For the duration of the study, exercise activity was kept constant and monitored
by a physical activity questionnaire that asked subjects to document the physical activity
they participated in daily. At baseline and during the 8 months of the study, each subject
kept a daily diary of activity type, duration, intensity, and frequency. The study
coordinator (a registered dietitian and exercise physiologist) reviewed these diaries
monthly. If there was any deviation from initial activity levels, the study coordinator
counseled the subject to resume her normal activity, which was fully accomplished.
Deviations in activity during the study primarily resulted from illness or changes in the
weather, which did not last for prolonged periods of time before the women resumed
their previous activity level (1 week). During the course of the study, there were no
significant changes in exercise activity.
Assessment of Resting Energy Expenditure and Respiratory Quotient
The subjects were asked to arrive in lightweight, indoor clothing. Light blankets
were made available to those that requested them. Prior to testing, subjects rested for 30
minutes while lying on a treatment table in a thermoneutral environment that was quiet
and dimly lit. During this time, subjects refrained from listening to music, watching
television, readying, or other activities.
REE was measured in the fasting state, before breakfast, after 30 minutes of rest.
REE was collected for 10 minutes by continuous indirect calorimetry with a ventilated
hood system (Applied Electrochemistry/Thermox, Pittsburgh, PA). The gas analyzer was
calibrated before each procedure with a calibration gas of 16% O2, 4% CO2, and balance
23
N2. The pneumotach was calibrated and VO2 and VCO2 were measured each minute. As
suggested by Compher el al. (2006), the initial five minutes were discarded. Five minutes
of steady state were averaged and used to derive REE. Steady state was defined as a
period of five consecutive minutes during which the coefficient of variation (CV) for
VO2 and VCO2 were < 10% (Compher et al., 2006). The VO2 and VCO2 during the
steady state with the lowest CV were then used to calculate REE with the Weir equation
(Weir, 1949). The Weir equation is as follows: REE (kcal/min) = [(1.1(VCO2/VO2)]+3.9)
x VO2] (Weir, 1949).
Data Analysis
Data were expressed as means + standard deviations (SD). The dependent
variables REE, RER, and body composition values were analyzed with respect to dietary
intervention by analysis of variance with repeated measures. Significant main effects or
interactions were analyzed by Tukey’s Post-hoc test. A P-value of <0.05 was considered
statistically significant. All the analyses were carried out using Statistica 5.5 for windows
(StatSoft Inc, Tulsa, OK).
24
CHAPTER 4
Results
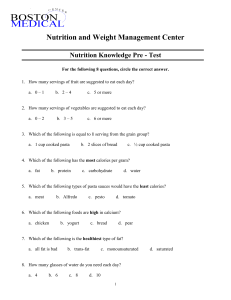
Resting Energy Expenditure and Respiratory Quotient
The primary question of this study was if there was an effect of dietary fat intake
on resting energy expenditure during a eucaloric intervention. REE did not significantly
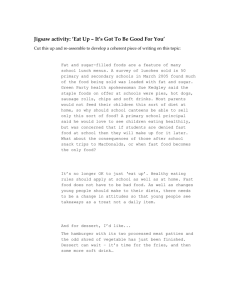
change with respect to dietary intervention (p=.979) (Figure 1). There was a trend for
respiratory exchange ratio to increase with a reduction in lipid composition of the
eucaloric diets (p=.067) (Figure 2).
Changes in Nutrient Intake
Although the controlled-feeding phase was designed by calculated, computer
generated analysis to deliver 35%, 25% and 15% of the energy intakes from fat,
laboratory and chemical analysis of the diet showed that the actual dietary fat intakes
were 31%, 23% and 14% respectively. The corresponding carbohydrate intakes were
53%, 60%, and 67% of the daily energy (Table 2).
Energy and Dietary Fat Intake
At the entry, the self-reported energy intake was 6896+ 1726 kJ, while at the end
of the 31%-fat period the energy intake required for weight maintenance was 8724 +
1281 kJ, or 116+16 kJ per kg. The difference between the actual and self reported energy
intakes represented an under-reporting of 1828+445 kJ/day. The magnitude of underreporting correlated weakly with the degree of obesity (r = 0.309, p < 0.04).
25
Body weight correlated strongly with ECWM (r = 0.77, p < 0.0001). The initial
self reported dietary fat intake had a stronger relationship with the body weight (r =
0.321, p < 0.01) than with the poor relationship it had with self reported energy intake (r
= 0.263, p < 0.05). In addition, when compared with lean women, obese women
consumed higher amounts of fat (36.6+6.6% vs 29.4+6.7%, p < 0.0005). Taken all
together, these findings suggested that self-reported food records are more useful in the
assessment of dietary fat intake than the energy intake.
Energy Cost of Weight Maintenance
During the eucaloric feeding as dietary fat decreased from 31 % to 23% to 14 %,
the energy cost of weight maintenance increased from 8724+1281 kJ, to 8946+ 1310 kJ,
and to 9122+ 1365 kJ, respectively. These increases were significant ( +223+400 kJ, p <
0.02 and +398+638 kJ, p < 0.0001 ). At the end of the metabolic feeding phase 29
women required an increase in the energy intake ( +770+592 kJ), and 20 women did not
(-154+269 kJ). All the obese subjects belonged to the first group (+895+528 kJ).
Changes in Weight
During the eucaloric phase, weight and body composition slightly (~% approx.)
decreased with each feeding. There was a significant difference in body weight between
baseline and after the 35% fat diet (p=0.0003), no significant change between the 35%
and 25% fat diet (p=0.218), and no significant change between the 25% fat diet and the
15% fat diet (p=0.156) (Figure 3).
26
Percent Body Fat, Fat Mass, and Fat Free Mass
There was a significant reduction in body fat, fat mass, and fat free mass after the
35% fat eucaloric feeding (p=0.033, 0.0008, 0.0001) respectively. There was no
significant difference between the 25% fat (p=0.297, 0.224, 0.419) and 15% fat feeding
(p=0.079, 0.147, 0.177) (Figure 4, 5, 6).
27
Table 1.
Changes in weight, percent body fat, daily energy intake, resting energy expenditure,
respiratory quotient, fat mass and fat free mass during eucaloric restriction of dietary fat
intake (Mean + S.D., n = 38).
WEIGHT (kg)
BODY FAT
ENERGY INTAKE
35%-FAT
25%-FAT
15%-FAT
78.9+22.8*
78.6+22.7
78.4+23.0*
30.3+9.4
30.1+9.4
29.8+9.7
8724+1281
8946+1310*
9122+1365*
1414.7+283.9
1426.7+328.8
1423.7+299.6
(kJ/day)
REE (kcal)
RER
0.82+0.09
0.83+0.07
0.84+0.07
FAT MASS
25.8+15.0*
25.5+15.0
25.3+15.2*
FAT FREE MASS
53.1+8.3*
53.0+8.4
53.0+8.4*
Note. (*) indicates significantly different between groups, P<0.05.
Table 2.
28
Differences in analysis of dietary energy, fat, and carbohydrate of the same 7 day menu
cycles by Hazelton Laboratories, Nutritionist IV, and Nutrition Data Systems.
35% Fat Menu
Hazelton
Energy
Fat
Carbohydrate
Protein
Cholesterol
Fiber
(kJ)
(gm)
(gm)
(gm)
(mg)
(gm)
1571
52.9
205.7
68.6
161
14.3
1665
63.7
208.9
68.2
202
13.8
1748
67.9
205.6
78.7
322
12.1
Energy
Fat
Carbohydrate
Protein
Cholesterol
Fiber
(kJ)
(gm)
(gm)
(gm)
(mg)
(gm)
1500
38.6
224.3
65.7
134
17.2
1603
45.2
238.7
68.1
157
17.7
1747
44.2
263.9
79.2
166
12.4
Laboratories
Nutrition Data
Systems
Nutritionist IV
Hazelton
Laboratories
Nutrition Data
Systems
Nutritionist IV
29
Hazelton
Energy
Fat
Carbohydrate
Protein
Cholesterol
Fiber
(kJ)
(gm)
(gm)
(gm)
(mg)
(gm)
1629
25.7
272.9
77.1
120
17.1
1607
27.1
274.9
73.9
138
19.1
1749
31.4
286.4
86.7
286
12.6
Laboratories
Nutrition Data
Systems
Nutritionist IV
30
1600
*
1550
*
Resting Energy Expenditure (kcal)
*
1500
1450
1400
1350
1300
1250
Baseline
35% Fat
25% Fat
15% Fat
Dietary Intervention
Figure 1. Effects of Resting Energy Expenditure (REE) with dietary fat restriction. (*)
indicates not significantly different from baseline , P>0.05.
31
0.88
*
0.87
0.86
*
*
Respiratory Quotient (RQ)
0.85
0.84
0.83
0.82
0.81
0.80
0.79
0.78
Baseline
35% Fat
25% Fat
15% Fat
Dietary Intervention
Figure 2. Effects of Respiratory Exchange Ratio (RER) with dietary fat restriction.
(*) Indicates trend, P=0.06.
32
90
88
*
*
*
86
84
Body Weight (kg)
82
80
78
76
74
72
70
68
Baseline
35% Fat
25% Fat
15% Fat
Dietary Intervention
Figure 3. Effects of Body Weight (BW) with dietary fat restriction. (*) indicates
significantly different from baseline, P<0.05.
33
57
*
*
*
56
Fat Free Mass (%)
55
54
53
52
51
50
49
Baseline
35% Fat
25% Fat
15% Fat
Dietary Intervention
Figure 4. Effects of Fat Free Mass (FFM) with dietary fat restriction. (*) indicates
significantly different from baseline, P<0.05.
34
34
32
*
*
*
30
Fat Mass (%)
28
26
24
22
20
18
Baseline
35% Fat
25% Fat
15% Fat
Dietary Intervention
Figure 5. Effects of Fat Mass (FM) with dietary fat restriction. (*) indicates significantly
different from baseline , P<0.05.
35
0.35
0.34
*
*
*
0.33
Body Fat (%)
0.32
0.31
0.30
0.29
0.28
0.27
0.26
0.25
Baseline
35% Fat
25% Fat
15% Fat
Dietary Intervention
Figure 6. Effects of Body Fat (BF) with dietary fat restriction. (*) indicates significantly
different from baseline , P<0.05.
36
CHAPTER 5
Discussion
This study was designed to evaluate the effects of dietary fat intake while
controlling ECWM and to investigate the effects of dietary fat restriction among postmenopausal women. Our results demonstrate that a restriction in fat intake increases the
ECWM. Dietary fat restriction has no effect on REE or RER, and decreases were found
in FM, FFM, and BF despite a large significant increase in ECWM calories.
We observed that as dietary fat intake decreased from 31% to 23% and to 14%,
the daily energy requirement increased by 223+400 kJ and 398+638 kJ. At the end of the
31%-fat diet daily energy requirement was 8724 kJ, providing 2706 kJ from fat. When
the fat intake was reduced to 23% and 14% respectively, relative contribution of fat
calories decreased to 2007 kJ and 1221 kJ per day. When compared to the 23%-fat and
14%-fat diets, 31%-fat diet provided 698 kJ and 1483 kJ more energy from fat. These
findings are supported by previous research that found carbohydrates that are used to
synthesize lipid are 25% less efficient (Hegsted et al., 1993). One could speculate that a
person could consume 25% more calories in CHO than fat without gaining weight. If
these differences in fat-calories can be replaced with an equivalent amount of CHO
calories, the increases in energy requirement would be 233 kJ/day during the 23%-fat,
and 494 kJ/day during the 14%-fat diets. These predicted values were similar to the
actual increases in caloric intake seen in our study. Another antidotal observation is that
all the women who required an increase in caloric intake to maintain ECWM were obese.
37
This could suggest that obese may process macronutrients differently than normal weight
post-menopausal women.
Our study clearly demonstrated an increase in the ECWM in proportion to the
amount of fat reduction and increase in CHO. While our study failed to demonstrate any
change in REE, this suggests that the increase in energy expenditure must occur during
the day and likely post-prandially. Further controlled research looking at 24-hour energy
expenditures with post-prandial values compared, more variations in fat intake, with
whole foods and a variety of genetic backgrounds need to be done to fully explain the
inconsistencies seen in this area. Brehm et al., (2003) did not find any differences in
REE when comparing a high fat to high carbohydrate diet. They concluded that the
macronutrient makeup of a diet does not affect REE. However, we feel there is sufficient
evidence to support both an increase in the ECWM and when consumed ad-libitum a
decreased caloric intake due to the lower nutrient density with very low-fat diets leading
to the weight loss associated with low-fat diets.
Previous studies have suggested the importance of RER adjusting for the
oxidative rates in metabolism (Rising, Tataranni, Snitker, Ravussin, 1996). Although
there was not a significant change in RER (p=.067), we observed a trend. After the first
eucaloric feeding, RER dropped to correlate with the amount of fat in the diet. As we
decrease the amount of fat, RER increased to match the fat oxidative rates. This trend
was expected to show the body’s adjustment to the amount of fat and carbohydrate being
oxidized. This supports that low fat diets require more energy to maintain body weight.
38
This is important because if we utilize less fat and our metabolic rates decrease with age,
it can contribute to an increase in obesity (Rising et al., 1996).
While we tried to maintain body weight and control for body composition using a
eucaloric diet, decreases in FFM, FM, and BF were observed. FFM decreased from
baseline to the end of the 15% fat intervention by 0.6% which was significant (p=.001).
FM similarly decreased by 1.3% along with a decrease of 0.8% in BF. This demonstrates
that by decreasing the proportion of fat to carbohydrate macronutrients it allows subjects
to eat more and still lose weight. While we increased the intake of calories to prevent
further weight loss to maintain body weight, the decrease in body composition was
significant. Therefore, there must be a mechanism to explain the change in weight. Our
first prediction is that we did not account for the efficiency of macronutrients in the diet.
It is more costly for the body to process carbohydrates. This energy difference equates to
about 25% of carbohydrates consumed that must be broken down and metabolized in
order to be stored as lipid in the body. This increase cost of metabolizing carbohydrates
may represent the amount of weight loss that occurred in our study. There could have
also been an error in calculating the eucaloric diet, or an error in calculating the
additional calories needed to maintain body weight, or physical activity might not have
been monitored accurately. All of these factors could lead to an error in maintaining body
composition.
Future Research
There are some areas of our study that could be improved. Our study was very
well controlled for diet by sending our food samples to Hazelton Laboratory to be
39
analyzed. The most important implication for future studies is to look at post prandial
values. We collected resting energy expenditure after 12 hours fasting. With the results of
our study indicating that there is not a significant change in REE, differences could be
occurring during the day post prandially. Also, it is important to note that by maintaining
a eucaloric diet, we did not control for how the calories are being processed
metabolically. This could explain the predicted mechanisms of the weight loss that
occurred in our study. Additionally physical activity levels could have been monitored
directly than by a recall survey questionnaire. While we obtained physical activity logs
from the subjects to account for the calories being burned, directly monitored physical
activity would be more accurate . We could also improve our body composition data
collection. In this study we used BIA to calculate body composition. The new gold
standard is the DEXA (Dual-energy x-ray absorptiometry). While it is extensively used
for the assessment of body composition and is considered valid and reliable, it is large
and expensive. Another area our study could improve is the length of the study. The first
dietary intervention was 4-weeks, the second was 6-weeks, and the last dietary
intervention was 6-weeks. Although this may be sufficient time, additional long term
studies might yield different results.
Conclusion
In summary, the present study supports that low-fat intake increases the ECWM,
causes less efficient storage of energy, and decreases in body weight. However, there are
other benefits of low fat caloric diet. High fat intake increases the risks for coronary
artery disease and certain types of cancer, both related to and independent of obesity
40
(Wadden, Foster, Stunkard, Conill, 1996). On the other hand, low-fat intake can improve
risk factors for coronary artery disease, such as dyslipidemia, and results in weight loss
without food deprivation. Therefore, it seems prudent to suggest restriction of dietary fat
especially in the obese population.
In obese post-menopausal women, an ECWM diet containing a decreased fat-tocarbohydrate ratio may enhance weight loss and significantly increase energy
expenditure. Macronutrient composition of the diet, an important determinant of
metabolic efficiency can indirectly induced weight loss by inducing a negative caloric
balance. Further studies that carefully control for the macronutrient metabolic efficiency
and ECWM will elucidate the efficacy of low fat diets on REE and weight loss in normal
versus obese post-menopausal women.
41
REFERENCES
Abbot W.G.H., Howard, B.V., Ruotolo, G., Ravussin, E. (1990). Energy expenditure in
humans: effects of dietary fat and carbohydrate. American Journal of Physiology,
258: E347-51.
Amenorrhoea. (n.d.) Mosby's Medical Dictionary, 8th edition. (2009). Retrieved
from http://medical-dictionary.thefreedictionary.com/amenorrhoea
Astrup, A., Buemann B., Christensen, N.J., Madsen, J. (1994). 24-hour energy
expenditure and sympathetic activity in postobese women consuming a
high-carbohydrate diet. American Journnal of Physiology, 226, E592599.
Barrett-Connor, E., Friedlander N.J. (1993). Dietary fat, calories, and the risk
of breast cancer in postmenopausal women: a prospective populations
based study. Journal of American Coll Nutrition, 12, 390-9.
Blundell, Caudwell, Gibbons, Hopkins, Naslund, King, and Finlayson, (2011).
Body Composition and appetite: fat-free mass (but not fat mass of
BMI) is positively associated with self-determined meal size and daily
energy intake in humans. British Journal of Nutrition, 107(3):445-9.
Bray & Pompkin, (1998). Dietary fat affects obesity rate. American Journal of
Clinical Nutrition, 68(6): 1157-73.
42
Brehm, Seeley, Daniels, D’Alessio, (2003). A randomized trial comparing a
very low carbohydrate diet and a calorie-restricted low fat diet on body
weight and cardiovascular risk factors in healthy women. Journal of
Clinical Endocrinology and Metabolism, 88(4):1617-23.
Brehm, Spang, Lattin, Seeley, Daniels et al. (2005). The Role of Energy
Expenditure in the Differential Weight Loss in Obese Women on Low-Fat
and Low-Carbohydrate Diets. Journal of Clinical Endocrinology and
Metabolism, 90 (3): 1475.
Chapman, Bannerman, Cowen, & Maclennan, (1998). The relationship of anthropometry
and bio-electrical impedance to dual-energy X- ray
absorptiometry in elderly men and women. Age and Ageing, 27: 363 –
367.
Compher, Frankenfield, Keim, Roth-Yousey, (2006). Best practice methods to
apply to measurement of resting metabolic rate in adults: a systematic
review. Journal of the American Diet Association, 106(6):881-903.
Cunningham, JJ. (1980). A reanalysis of the factors influencing basal metabolic
rate in normal adults. American Journal of Clinical Nutrition, 33:23722374.
Gallagher & Song, (2003). Evaluation of body composition: practical guidelines.
Primary Care. 30(2):249-65.
43
Hegsted, D.M., Ausman, L.A., Johnson, J.A., Dallal, D.E. (1993). Dietary fat and
serum lipids: an evaluation of the experimental data. American Journal of
Clinical Nutrition, 57: 875-83.
Heyward V.H., Wagner, D.R. (2004). Applied Body Composition Assessment.
Champaign, IL: Human Kinetics. pp. 87–98.
Hill, JO. (2006). Understanding and addressing the epidemic of obesity: an energy
balance perpective. Endocrine Reviews, 27(7), 750-761.
Hill, Sparling, Shields, & Heller, (1987). Effects of exercise and food restriction
on body composition and metabolic rate in obese women. The American
Journal of Clinical Nutrition, 46(4), 622-630.
Horton, Drougas, Brachey, et al. (1995). Fat and carbohydrate overfeeding in
humans: different effects on energy storage. American Journal of Clinical
Nutrition, 62, 19–29.
Lean M.E.J., James W.P.T., (1988). Metabolic effects of isoenergetic nutrient
exhange over 24 hours in relation to obesity in women. International
Journal of Obesity; 12, 15-27.
Leibel, R.L., Hirsch J., Appel, B.E., Checani, G.C. (1992). Energy intake required to
maintain body weight is not affected by wide variation in diet composition.
American Journal of Clinical Nutrition, 55, 350-5.
Lissner, L., Levitsky, D.A., Strupp, B.J., Kalkwarf, H.J., Roe, D.A. (1987). Dietary
fat and the regulation of energy intake in human subjects. American Journal of
Clinical Nutrition, 46, 886-92.
44
Martin, L.J., Su, W., Jones, P.J., Lockwood, G.A., Tritchler, D.L., Boyd, N.F.
(1996). Comparison of energy intakes determined by food records and
doubly labeled water in women participating in a dietary-intervention
trial. American Journal of Clinical Nutrition, 63, 483-90.
Noakes, Keogh, Foster, and Clifton, (2005). Effect of an energy-restricted, highprotein, low-fat diet relative to a conventional high-carbohydrate, low-fat
diet on weight loss, body composition, nutritional status, and markers of
cardiovascular health in obese women. American Journal of Clinical
Nutrition, 81(6) 1298-1306.
Prewitt, Schmeisser, Bowen, Aye, Dolecek, Langenberg, Cole & Brace, (1991).
Changes in body weight, body composition, and energy intake in women
fed high- and low-fat diets. American Journal of Clinical Nutrition, 54,
304-310.
Rising, Tataranni, Snitker, Ravussin, (1996). Decreased ratio of fat to
carbohydrate oxidation with increasing age in Pima Indians. Journal of the
American College of Nutrition, (3):309-12.
Roust, Hammel, & Jensen, (1994). Effects of isoenergetic, low fat diets on energy
metabolism in lean and obese women. American Journal of Clinical
Nutrition, 60, 470-475.
Sacks, Bray, Carey, Smith, Ryan et al. (2009). Comparison of Weight Loss Diets with
Different Compositions of Fat, Protein and Carbohydrates. New
England Journal of Medicine. 360:859-873.
45
Segal, Van Loan, Fitzgerald, Hodgdon & Van Itallie, (1988). Lean body mass
estimation by bioelectrical impedance analysis: a four- site crossvalidation study. American Journal of Clinical Nutrition, 47, 7-14.
Stubbs, William, Coward, Prentice, (1995). Convert manipulation of the ratio of
dietary fat to carbohydrate and energy density: effect on food intake and
energy balance in free-living men eating ad ibitum. American Journal of
Clinical Nutrition, 62:330-7.
Volek, Sharman, Gómez, Judelson, Rubin, Watson, Sokmen, Silvestre, French &
Kraemer (2004). Comparison of energy-restricted very low-carbohydrate
and low fat diets on weight loss and body composition in overweight men
and women. Nutrition and Metabolism, 1:13 doi:10.1186/1743-7075-1-13.
Wadden, Foster, Stunkard, Conill, (1996). Effects of weight cycling on the
resting energy expenditure and body composition of obese women.
International Journal of Eating Disorders; 19: 5-12.
Weir, J.B. de V. (1949): New methods for calculating metabolic rate with special
reference to protein metabolism. Physiology. 109, 1—9.
World Health Organization, (1998). Obesity: Preventing and Managing the
Global Epidemic (World Health Organization, Geneva).