Shoulder Impingement - Active Physical Therapy
advertisement

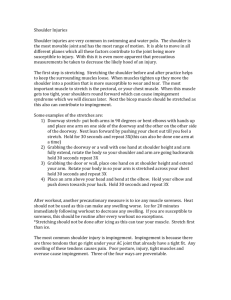
SHOULDER IMPINGEMENT PT Intervention Strategies By Parley Anderson, DPT Shoulder Impingement WHAT’S THE PROBLEM???????? https://www.youtube.com/watch?v=FAh_8erWyQw Shoulder Impingement and PT Treatment What does the Research Say? PHYSICAL THERAPY INTERVENTIONS Studies have shown that designing a specific evidence-based program for each patient is more effective and beneficial compared to a more cookie cutter approach using the same interventions for all patients with shoulder impingement (Ebuagh et al., 2010). Factors to be considered in prescribing interventions: Classify the impairments believed to be causative to the individual's pain and functional limitations. Create an impairment based restoration program. EXERCISES FOR SHOULDER IMPINGEMENT For an effective anterior shoulder stretch, place the hand over the head, shoulder in 90° of abduction and 90° of external rotation, and lean forward on a door frame (Ebuagh et al, 2010). Scaption with thumb- up exercise for strengthening. Y- exercise. Standing with the arms at the sides, move the shoulders into extension against resistance of an elastic band. Studies have shown better results in electromyographic activities for strengthening the trapezius muscle (Ebaugh et al, 2010). Eccentric Strengthening Exercises Full can scaption with a dumbbell (starting position must be pain-free). Eccentric external rotation using a dumbbell in sidelying position. (Studies show that adding eccentric exercises to traditional shoulder rehab protocols can increase strength and decrease pain (Maenhout et al, 2012; Bernhardsson et al, 2011.) PNF Paired with Trigger Point Release Trigger point release of the subscapularis Contract/relax of the subscapularis to move into greater external rotation PNF D2 flexion pattern This treatment was found to decrease pain and increase glenohumeral ER plus overhead reach (AlDajah & Unnikrishnan, 2014). PT and Shoulder Impingement: A New Approach My Physical Therapy Evaluation: History (DOI, MOI, Past Treatments, Surgery etc) Establish baselines: Pain levels/Location of Pain ROM (Active/Passive) Strength Special Test/Concordant Sign/Functional Test Develop Provisional Diagnosis Derangement Dysfunction Test Hypothesis (Apply Mechanical Forces/Strategies) Re-Assess Baselines Confirm/Deny Hypothesis Shoulder Impingement Derangement: Symptoms rapidly changeable (i.e can get better/worse quickly) Symptoms can be constant or intermittent ROM rapidly changeable Can be acute, sub-acute or chronic lesion Can become dysfunctions over time Rx: Reduce the derangement Directional Preference Anatomical Cause: Disruption of Joint Surfaces Encroachment of Meniscoids in joint space Shoulder Impingement Dysfunction: Symptoms (when present) are more consistent in nature Symptoms are more intermittent (no pain when tissue is on slack) ROM is consistent Pain is usually found at End Range (stretch short/tight tissue) Lesion must be 10-12 weeks or older (mostly chronic lesions) Rx: Remodel Tissue Anatomical Cause Joint adhesions/Contracture Maladaptive muscle shortening Scar tissue formation Shoulder Impingement Directional Preference Direction of motion/force that may do one or more of the following Reduce pain Restore motion Improve strength Improve function Improve concordant sign/special test Directional Preference Preferred treatment strategy for derangements May be painful to perform May be painless to perform May feel “good” to perform SHOULDER EXTENSION SHOULDER EXTENSION INTERNAL ROTATION INTERNAL ROTATION INTERNAL ROTATION HORIZONTAL ABDUCTION HORIZONTAL ADDUCTION https://www.wetransfer.com/downloads/2beb09622 bf9f050ac748092a7380c3c20150729111750/15be1f7b 5b748c974f7f08e6a856160320150729111750/f533eb REFERENCES AlDajah, SB. & Unnikrishnan, R. (2014). Subscapularis trigger release and contract relax technique in patients with shoulder impingement syndrome. European Scientific Journal (2014). 10(30): 408-416. Retrieved July 29, 2015, from ProQuest database. Berhardsson, S., Klintberg, IH., Wendt, GK. (2011). Evaluation of an exercise concept focusing on eccentric strength training of the rotator cuff for patients with subacromial impingement syndrome. Clinical Rehabilitation 25:69-78. Retrieved July 29, 2015, from ProQuest database. Ebaugh, D., Fleming, J, Seitz, A., (2010). Exercise protocol for the Treatment of Rotator Cuff Impingement Syndrome. Journal of Athletic Training, 45(5). 483-5. Retrieved July 29,2015, from ProQuest database. Maenhout, AG., Mahieu, NN., DeMuynck M., DeWilde, LF., Cools, AM. (2012). Does adding heavy load eccentric training to rehabilitation of patients with unilateral subacromial impingement result in better outcome? A randomized, clinical trial. Knee Surgery, Sports Traumatology, Arthroscopy (2013), 21:1158-1167. Retrieved July 29, 2015, from ProQuest database. Mckenzie Institue Shoulder Impingement p