CLASS III
advertisement

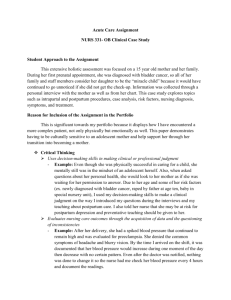
MODULE 3 THE NEWBORN POSTPARTUM ADAPTION • TRANSITION TO EXTRAUTERINE LIFE • NURSING ASSESSMENT OF THE NEWBORN • NEWBORN NEEDS AND CARE • POSTPARTUM ASSESSMENT • POSTPARTUM NEEDS AND CARE MODULE 3 PART 1A TRANSITION TO EXTRAUTERINE LIFE • RESPIRATORY – FETAL LUNG DEVELOPMENT – ALVEOLI – SURFACTANT – LECITHIN/SPHINGOMYELIN RATIO – FETAL BREATHING MOVEMENTS RESPIRATORY PHYSICAL (MECHANICAL) EVENTS – FLUID IN FETAL LUNGS ALMOST COMPLETELY EXPANDS LUNGS; AIR SPACES FILLED – PRODUCTION OF FLUID SHARPLY DECLINES 2-4 DAYS BEFORE LABOR – THORACIC SQUEEZE RESPIRATORY ADAPTION • AFTER BIRTH CHEST WALL RECOILS, CREATES NEGATIVE INTRATHORAIC PRESSURE; AIR IS SUCKED BACK INTO LUNG FIELDS, REPLACING FLUID • AFTER FIRST INSPIRATION, NEWBORN EXHALES, CREATING POSITIVE INTRATHORACIC PRESSURE MODULE 3 PART 1B TRANSITION TO EXTRAUTERINE LIFE RESPIRATORY ADAPTION • POSITIVE PRESSURE DISTRIBUTES INSPIRED AIR THROUGHOUT ALVEOLI • LUNGS CONTINUE TO EXPAND WITH EACH BREATH • REMAINING LUNG FLUID MOVES INTO INTERSTITIAL TISSUE CARDIOVASCULAR ADAPTION • BEFORE BIRTH – ARTERIALIZED BLOOD FROM PLACENTA – INTO FETUS THROUGH UMBILICAL VEIN AND PASSES RAPIDLY THROUGH LIVER INTO INFERIOR VENA CAVA – FLOWS THROUGH FORAMEN OVALE INTO LEFT ATRIUM TO AORTA AND ARTERIES OF HEAD WHY? CARDIOVASCULAR ADAPTION – PORTION BYPASSES LIVER THROUGH DUCTUS VENOSUS – VENOUS BLOOD FROM LOWER EXTREMITIES AND HEAD PASSES PREDOMINATELY INTO RIGHT ATRIUM, RIGHT VENTRICLE AND THEN INTO DESCENDING PULMONARY ARTERY AND DUCTUS ARTERIOSUS – THEREFORE, THE FORAMEN OVALE AND DUCTUS ARTERIOSUS ACT AS BYPASS CHANNELS CARDIOVASCULAR ADAPTION – THIS ALLOWS LARGE PART OF COMBINED CARDIAC OUTPUT TO RETURN TO PLACENTA WITHOUT FLOWING THROUGH THE LUNGS • AFTER BIRTH – INFANT’S FIRST BREATH INFLATES LUNGS—REDUCES PULMONARY VASCULAR RESISITANCE TO PULMONARY BLOOD FLOW CARDIOVASCULAR ADAPTION – DROP IN PULMONARY ARTERY PRESSURE – DECLINE IN RIGHT ATRIUM PRESSURE – INCREASED PULMONARY BLOOD FLOW RETURNED TO LEFT SIDE OF HEART INCREASES PRESSURE IN LEFT ATRIUM – THIS CHANGE CAUSES FUNCTIONAL CLOSURE OF FORAMEN OVALE CARDIOVASCULAR ADAPTION – DUCTUS ARTERIOSUS CONSTRICTS AS A RESULT OF ELEVATION OF SYSTEMIC VASCULAR PRESSURE ABOVE PULMONARY VASCULAR PRESSURE WHICH INCREASES PULMONARY BLOOD FLOW – INCREASE IN BLOOD OXYGENATION CONCENTRATION CAUSES MUSCULAR WALLS OF DUCTUS ARTERIOSUS TO CLOSE IN APRROX. 12 HOURS CARDIOVASCULAR ADAPTION • CAUSE OF CLOSURE OF DUCTUS VENOSUS UNKNOWN • CLOSURE ALLOWS BLOOD TO FLOW TO THE LIVER – THOUGHT TO BE DO TO: • PRESSURE CHANGES AFTER CUTTING OF CORD • CARDIAC OUTPUT • MECHANICAL PRESSURE CHANGES Figure 3–11 Fetal circulation. Blood leaves the placenta and enters the fetus through the umbilical vein. After circulating through the fetus, the blood returns to the placenta through the umbilical arteries. The ductus venosus, the foramen ovale, and the ductus arteriosus allow the blood to bypass the fetal liver and lungs. MODULE 3 PART 1C TRANSITION TO EXTRAUTERINE LIFE CHEMICAL STIMULI • CHEMICAL: FIRST BREATH (GASP). CESSATION OF PLACENTAL BLOOD FLOW STIMULATES MEDULLA TO TRIGGER RESPIRATORY EFFORTS. • SURFACTANT REDUCES SURFACE TENSION OF LUNG MUCOSA AND ALLOWS EXHALATION WITHOUT LUNG COLLAPSE THERMAL STIMULI • THERMAL: SUDDEN CHILLING OF THE MOIST INFANT STIMULATES THE SKIN SENSORY RECEPTORS TO TRANSMIT IMPULSES TO THE RESPIRATORY CENTER, WHICH STIMULATES THE INITIATION OF BREATHING. • EXCESSIVE COLD MAY RESULT IN COLD STRESS SENSORY STIMULI • SENSORY: – TACTILE, AUDITORY, AND VISUAL STIMULI CAN HAVE AN EFFECT ON RESPIRATION (DRYING OF INFANT, SKIN TO SKIN CONTACT) HEMATOPOIETIC SYSTEM • AFTER BIRTH RBCS INCREASE, CELL SIZE DECREASES • HEMACRIT INCREASES 1-2 DAYS AFTER BIRTH AS A RESULT OF: – PLACENTAL TRANSFUSION – LOW FLUID INTAKE – DIMINISHED EXTRACELLULAR VOLUME DECREASED % OF NEUTOPHILS LEUKOCYTOSIS MODULE 3 PART 1D TRANSITION TO EXTRAUTERINE LIFE THERMOREGULATION • NEONATE MUST BALANCE HEAT LOSS AND HEAT GENERATION – HEAT IS GENERATED BY METABOLISM OF BROWN FAT HEAT LOSS THROUGH: – CONVECTION – RADIATION – CONDUCTION – EVAPORATION Figure 21–6 The distribution of brown adipose tissue (brown fat) in the newborn. Source: Adapted from Davis, V. (1980, November–December). Structure and function of brown adipose tissue in the neonate. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 9, 364. THERMOREGULATION EXPLAIN WHY NEWBORNSNEWBORNS HAVE DIFFICULTY WITH THERMOREGULATION RELATED TO: • SHIVERING • SUBCUTANEOUS FAT • BODY MASS AND WEIGHT THERMOGENESIS • HEAT PRODUCTION – INCREASED BMR – MUSCULAR ACTIVITY – NONSHIVERING THERMOGENESIS (NST) NEWBORNS CONSERVE HEAT WITH A FLEXED POSTURE THERMOREGULATION • RELATE THE PROCESS OF THERMOGENESIS IN THE NEWBORN AND THE MAJOR MECHANISMS OF HEAT LOSS TO THE CHALLENGE OF MAINTAINING NEWBORN THERMAL STABILITY. MODULE 3 PART 1E TRANSITION TO EXTRAUTERINE LIFE HEPATIC ADAPTION • IRON CONTENT STORED IN ______. • CARBOHYDRATE METABOLISM—LOW CARBOHYDRATE RESERVES • MAIN SOURCE OF ENERGY IS _______. • LIVER BEGINS TO CONJUGATE BILIRUBIN • LACK OF INTESTINAL FLORA RESULTS IN ? CONJUGATION OF BILIRUBIN • UNCONJUGATED BILIRUBIN ATTACHES TO GLUCURONIC ACID IN THE LIVER AND BECOMES CONJUGATED • THE CONJUGATED BILIRUBIN CAN NOW BE EXCRETED BECAUSE IT HAS CHANGED FROM FAT SOLUBLE TO LIVER SOLUBLE • TOTAL BILIRUBIN IS BOTH THE CONJUGATED AND UNCONJUGATED BILIRUBIN < 3MG/DL CONJUGATION OF BILIRUBIN • TYPES OF BILIRUBIN – CONJUGATED – UNCONJUGATED – TOTAL – UNCONJUGATED BILIRUBIN IS THE BREAKDOWN PRODUCT DERIVED FROM Hgb and is not in excretable form (FAT SOLUBLE) • BILIRUBIN IS TRANSPORTED IN BLOOD VIA ALBUMIN; BINDS WITH ALBUMIN FOR EXCRETION • BILIRUBIN IS TRANSFERRED INTO THE HEPATOCYTES IN THE LIVER PHYSIOLOGICAL JAUNDICE • VERY COMMON IN NEWBORNS • APPEARS AFTER FIRST 24 HRS OF LIFE • ACCELERATED DESTRUCTION OF FETAL RBCs – INCREASED AMOUNTS OF BILIRUBIN DELIVERED TO LIVER MAY BE CAUSED BY: – INADEQUATE HEPATIC CIRCULATION – DEFECTIVE UPTAKE OF BILIRUBIN FROM THE PLASMA – DEFECTIVE CONJUGATION OF BILIRUBIN MODULE 3 PART 1F TRANSITION TO EXTRAUTERINE LIFE GI ADAPTION • GASTROINTESTINAL ADAPTION – LACTOSE – PROTEIN – FAT – SUFFICIENT ENZYMES EXCEPT AMYLASE – CARDIAC SPHINCTER IMMATURE • DIGESTION AND ABSORPTION • ELIMINATION – MECONIUM – TRANSITIONAL STOOLS FLUID AND ELECTROLYTE ADAPTION URINARY ADAPTION • OVER 90% OF NEWBORNS VOID WITHIN 24 HOURS AFTER BIRTH • IF NO VOIDING BY 48 HOURS: – BLADDER ASSESSMENT • PAIN • RESTLESSNESS • DISTENTION FLUID AND ELECTROLYTE ADAPTION • LESS ABLE TO CONCENTRATE URINE • LIMITED TUBULAR REABSORPTION OF WATER • LIMITED EXCRETION OF SOLUTES • LIMITED DILUTIONAL CAPABILITIES IMMUNOLOGIC ADAPTION • PREGNANT WOMAN FORMS ANTIGENS IN RESPONSE TO ILLNESS—ACTIVE ACQUIRED IMMUNITY • IgG—ONLY IMMUNOGLOGULIN THAT PASSES THROUGH THE PLACENTA— RESULTING IN PASSIVE ACQUIRED IMMUNITY. TRANSFERRED PRIMARILY IN THE THIRD TRIMESTER IMMUNOLOGIC ADAPTION • IgM—USUALLY NOT PASSIVELY TRANSFERED – ELEVATED LEVELS MAY INDICATE FETAL ANTIGENIC ACTIVITY IN UTERO • IgA—PASSIVE ACQUIRED IMMUNITY VIA COLOSTRUM FUNCTIONS NOT FULLY UNDERSTOOD (RESEARCH: RESP., GI, EYES) MODULE 3 PART 1G TRANSITION TO EXTRAUTERINE LIFE PERIODS OF REACTIVITY AFTER BIRTH • FIRST PERIOD OF REACTIVITY • PERIOD OF INACTIVITY • SECOND PERIOD OF REACTIVITY NEUROLOGIC &SENSORY PERCEPTION FUNCTION • FACTORS AFFECTING NEONATE’S ORGANIZATION AND QUALITY OF MOTOR ACTIVITY – SLEEP-WAKE STATES – ENVIRONMENTAL STIMULI – CHEMICAL IMBALANCE – HYDRATION STATUS – RECOVERY FROM STRESS OF BIRTH BEHAVIORAL STATES OF NEWBORN • HABITUATION • ORIENTATION • SELF QUIETING ABILITY • AUDITORY • OLFACTORY • TASTING, TACTILE BEHAVIOR STATES OF NEWBORN • SLEEP STATES – DEEP OR QUIET – ACTIVE REM • ALERT STATES – DROWSY, SEMIDOZING – WIDE AWAKE (QUIET ALERT) – ACTIVE AWAKE (ACTIVE ALERT) – CRYING MODULE 3 PART 2A NEWBORN ASSESSMENT NEWBORN ASSESSMENT • GESTATIONAL AGE ASSESSMENT – EXTERNAL PHYSICAL CHARACTERISITICS – NEUROLOGIC/NEUROMUSCULAR DEVELOPMENT THIS WILL BE PERFORMED IN CLINICAL Figure 22–12 Classification of newborns based on maturity and intrauterine growth. Sources: Adapted from Lubchenco, L. O., Hansman, C., & Boyd, E., (1966). Intrauterine growth in length and head circumference as estimated from live births at gestational ages from 26 to 42 weeks. Pediatrics, 37, 403–408; Battaglia, F. C., & Lubchenco, L. O. (1967). A practical classification of newborn infants by weight and gestational age. Journal of Pediatrics, 71, 159. PHYSICAL ASSESSMENT • DATA FROM OTHER SOURCES CAN INFLUENCE ASSESSMENT FINDINGS: – MATERNAL PRENATAL HISTORY – BIRTHING HISTORY – MATERNAL ANALGESIA/ANESTHESIA – TREATMENT GIVEN IMMEDIATELY AFTER BIRTH – GESTATIONAL AGE ASSESSMENT PHYSICAL ASSESSMENT • WEIGHT, LENGTH, CHEST, HEAD, ABDOMINAL MEASUREMENTS • VITAL SIGNS – TEMPERATURE, PULSE, RESPIRATION, BLOOD PRESSURE, PULSE OX WHAT ARE THE AVERAGE MEASUREMENTS FOR THE NEWBORN? PHYSICAL ASSESSMENT • HANDS OFF ASSESSMENT: OBSERVATION – NAME SIX AREAS YOU COULD OBSERVE WITH THE NEWBORN (HANDS OFF ASSESSMENT) PHYSICAL ASSESSMENT • HEAD – PROPORTIONALLY LARGER THAN BODY – SHAPE, SIZE, APPEARANCE – MOLDING – FONTANELLES – DEVIATIONS Figure 22–24 Cephalhematoma is a collection of blood between the surface of a cranial bone and the periosteal membrane. This is a cephalhematoma over the left parietal bone. Source: Potter, E. L., & Craig, J. M. (1975). Pathology of the fetus and infant (3rd ed.). Chicago: Year Book Medical Publishers. Reproduced with permission. Figure 22–25 Caput succedaneum is a collection of fluid (serum) under the scalp. Source: Photo courtesy of Mead Johnson Laboratories, Evansville, IN. MODULE 3 PART 2B NEWBORN ASSESSMENT PHYSICAL ASSESSMENT • SKIN – COLOR, TEXTURE, TURGOR DEVIATIONS – TELANGIECTATIC NEVI (STORK BITES) – MONGOLIAN SPOTS – ACROCYANOSIS – HARLEQUIN SIGN – JAUNDICE – ERYTHEMA TOXICUM – MILIA – MOTTLING PHYSICAL ASSESSMENT • EYES – TEARLESS CRYING – PERPHERAL VISION – CAN FIXATE ON NEAR OBJECTS – BLINKS IN RESPONSE TO BRIGHT LIGHT – PUPILLARY REFLEX PRESENT? PHYSICAL ASSESSMENT • NOSE – APPEARANCE – MIDLINE – PATENT NARES • EARS – PLACEMENT – SOFT, PLIABLE, READY RECOIL – DEVIATIONS MODULE 3 PART 2C NEWBORN ASSESSMENT PHYSICAL ASSESSMENT • NECK – APPEARANCE—SHORT WITH SKIN FOLDS – CLAVICLE – INSPECTION – REFLEXES—TONIC NECK, MORO • CHEST – APPEARANCE, SIZE, SHAPE – CIRCUMFERENCE – EXPANSION, RETRACTION – DEVIATIONS PHYSICAL ASSESSMENT • MOUTH – SYMMETRY OF MOVEMENT – REFLEXES—GAG, SWALLOWING, SUCKING – HARD/SOFT PALATE – EPSTEIN’S PEARLS – TONGUE—PROPORTION, COLOR, MOVEMENT, PLACEMENT DEVIATIONS PHYSICAL ASSESSMENT • HEART – LOCATION – PMI – RATE, RHYTHM – FUNCTIONAL MURMURS • ABDOMEN – APPEARANCE, SIZE, SHAPE – DIASTASIS RECTI, BOWEL SOUNDS – UMBILICAL CORD • BREASTS – DISTANCE BETWEEN NIPPLES, SHAPE – DEVIATIONS PHYSICAL ASSESSMENT • BLADDER • FEMORAL PULSES • INGUINAL AREA • BLADDER • GENITALS – MALE—PENIS, SCROTUM, TESTES, MEATUS – FEMALE—MONS, CLITORIS, LABIA MAJORA, MINORA, DISCHARGE – DEVIATIONS PHYSICAL ASSESSMENT • BUTTOCKS, ANUS – SYMMETRY – ANUS PATENT – GLUTEAL FOLDS • EXTREMITIES, TRUNK – RANGE OF MOTION, FLEXION, EXTENSION – DEVIATIONS PHYSICAL ASSESSMENT • EXTREMITIES – ARMS/LEGS: EQUAL IN LENGTH, SPONTANEOUS JOINT MOVEMENT, FLEXED WHEN QUIET, SYMMETRICAL MOVEMENT – HANDS/FEET: CORRECT # OF FINGERS, TOES, PALMAR, PLANTAR CREASES MODULE 3 PART 2D NEWBORN ASSESSMENT PHYSICAL ASSESSMENT • HIPS – ABDUCT TO MORE THAN 60 DEGREES – EQUAL KNEE HEIGHT – BARLOW, ORTOLANI MANEUVER • SPINE – C-SHAPED – FLAT, STRAIGHT – CORRECT # OF VERTEBRAE – TRUNCAL INCURVATION – DEVIATIONS Figure 22–34 A, Congenitally dislocated right hip in a young infant as seen on gross inspection. B, Barlow’s (dislocation) maneuver. Baby’s thigh is grasped and adducted with gentle downward pressure. Dislocation is palpable as femoral head slips out of acetabulum. C, Ortolani’s maneuver puts downward pressure on the hip and then inward rotation. If the hip is dislocated, this maneuver forces the femoral head over the acetabular rim with a noticeable “clunk.” NEUROLOGICAL ASSESSMENT • GENERAL PHYSICAL CHARACTERISTICS • OBSERVABLE BEHAVIORS: – STATE OF ALERTNESS, CRY – RESTING POSTURE – QUALITY OF MUSCLE TONE, MOTOR ACTIVITY PHYSICAL ASSESSMENT • NEUROMUSCULAR – SYMMETRICAL MOVEMENT – HEAD LAG • REFLEXES – – – IMMATURITY/DAMAGE TO THE CNS IS CHARACTERIZED BY A VARIETY OF CHANGES IN REFLEXES PROTECTIVE FEEDING MODULE 3 PART 2E NEWBORN ASSESSMENT PHYSICAL ASSESSMENT MORO BABINSKI ROOTING SUCKING PRONE CRAWL TONIC NECK STEPPING BLINKING, YAWNING, COUGHING, SNEEZING, DRAWING AWAY FROM PAIN NEUROLOGICAL ASSESSMENT ABNORMAL FINDINGS INCLUDING FLACCIDITY, TREMORS, FEEDING DIFFICULTIES, AND ASYMMETRY OF MOVEMENTS MAY INDICATE NEUROLOGICAL DAMAGE AND NEED FURTHER EVALUATION. WHAT MAY BE THE POSSIBLE CAUSES MAY BE RELATED TO THE ABOVE FINDINGS? MODULE 3 PART 3 ADMISSION PRODEDURES, NEEDS AND CARE ADMISSION PROCEDURES • WHY DO WE PERFORM A PHYSICAL & GESTATIONAL ASSESSMENT WITHIN TWO HOURS OF BIRTH? • STABLE VITAL SIGNS • CLEAR AIRWAY • NEUTRAL THERMAL ENVIRONMENT • PROPHYLACTIC VITAMIN K Figure 23–3 Injection sites. The middle third of the vastus lateralis muscle is the preferred site for intramuscular injection in the newborn. The middle third of the rectus femoris is an alternate site, but its proximity to major vessels and the sciatic nerve requires caution in using this site for injection. ADMISSION PROCEDURES • PROPHYLACTIC EYE TREATMENT • ASSESSMENT OF NEONATAL DISTRESS • FIRST FEEDING • PARENT NEWBORN ATTACHMENT NURSING CARE OF NEWBORN • MAINTENANCE OF CARDIOPULMONARY FUNCTION • THERMOREGULATION • ADEQUATE HYDRATION • SKIN INTEGRITY • SAFETY PROMOTION—PREVENTION OF COMPLICATIONS • CIRCUMCISION NURSING CARE OF THE NEWBORN • PARENT TEACHING – EXPECTED INFANT BEHAVIORS – GROWTH AND DEVELOPMENT PARAMETERS – SAFETY ISSUES – NEWBORN SCREENING/IMMUNIZATIONS – NEWBORN CARE – NEWBORN FEEDING NURSING CARE OF THE NEWBORN • ENHANCING PARENT-INFANT ATTACHMENT • PARENT TEACHING – PHYSICAL CHARACTEISTICS OF NEWBORN – BONDING PROCESS – SLEEP/WAKE CYCLES – COMFORTING TECHNIQUES MODULE 3 PART 4 NEWBORN NUTRITION NUTRITIONAL NEEDS OF NEWBORN • • • • • • • CALORIES PROTEIN FAT CARBOHYDRATES VITAMINS, MINERALS FLUID REQUIREMENTS WEIGHT GAIN BREAST FEEDING • ADVANTAGES – IMMUNOLOGIC – NUTRITIONAL – PSYCHOSOCIAL – CONVENIENCE • DISADVANTAGES – MEDICAL CONTRAINDICATIONS – MATERNAL MEDICATIONS – CONTAMINANTS IN BREAST MILK BREAST FEEDING – EXCLUSION OF FATHER – DIFFICULT TO MAINTAIN WITH MOTHER WORKING OUTSIDE THE HOME • COMPOSITION OF BREAST MILK – COLOSTRUM – TRANSITIONAL MILK – MATUREMILK – FOREMILK – HINDMILK FORMULA FEEDING • ADVANTAGES – PARENTS CAN SHARE FEEDING – EASIER FOR MOTHER WHO WORKS OUTSIDE THE HOME • DISADVANTAGES – FORMULAS PREPARATION – EXPENSE – ALLERGIC REACTIONS TO FORMULA – LACK OF IMMUNOLOGIC PROPERTIES MODULE 3 PART 5 POSTPARTUM ADAPTION POSTPARTUM PHYSICAL ADAPTIONS • • • • • • • INVOLUTION OF THE UTERUS CHANGES IN FUNDAL POSITION LOCHIA CERVICAL AND VAGINAL CHANGES PERINEAL CHANGES ABDOMEN GASTROINTESTINAL POSTPARTUM PHYSICAL ADAPTIONS • • • • • • URINARY TRACT VITAL SIGNS BLOOD VALUES WEIGHT LOSS POSTPARTAL DIAPHORESIS “AFTERPAINS” POSTPARTUM PSYCHOLOGIC ADAPTIONS • MATERNAL ROLE – TAKING IN PERIOD – TAKING HOLD PERIOD – BINDS IN PERIOD • MATERNAL ROLE ATTAINMENT – ANTICIPATORY STAGE – FORMAL STAGE, INFORMAL STAGE – PERSONAL STAGE DEVELOPMENT OF PARENT INFANT ATTACHMENT POSTPARTUM PSYCHOLOGIC ADAPTION • INITIAL BEHAVIOR – TOUCHING – EN FACE POSITION – SENSE OF SMELL – CONNECTEDNESS • ACQUAINTANCE PHASE • PHASE OF MUTUAL REGULATION • RECIPROCITY POSTPARTUM PSYCHOLOGIC ADAPTION • POSTPARTUM “ BLUES’’ • POSTPARTUM DEPRESSION • POSTPARTUM PSYCHOSIS CULTURAL INFLUENCE IN POSTPARTUM PERIOD • NON-WESTERN CULTURES EMPHASIZE POSTPARTUM PERIOD • • • • FOOD AND LIQUIDS AFTER BIRTH HOT-COLD BALANCE ROLE OF GRANDMOTHER ROLE OF FATHER MODULE 3 PART 6 POST PARTUM ASSESSMENT POSTPARTUM ASSESSMENT • • • • • • • • VITALS SIGNS, BREATH SOUNDS B U B B L E H POSTPARTUM ASSESSMENT • CULTURAL ASSESSMENT • PSYCHOLOGIC ADAPTION • ATTACHMENT ASSESSMENT • EDUCATION AND TEACHING POSTPARTUM NURSING CARE • PROMOTION OF PHYSICAL WELL BEING – UTERINE STATUS – VS – CARDIOVASCULAR STATUS – ELIMINATION PATTERNS – NUTRITIONAL STATUS – SLEEP/REST – COMFORT PROMOTION POSTPARTUM NURSING CARE • EDUCATIONAL NEEDS • PARENT INFANT ATTACHMENT • RUBELLA IMMUNITY • PREVENT DEVELOPMENT OF ANTIGENS • TREAT ANEMIA POSTPARTUM NURSING CARE • COMFORT MEASURES – PERINEAL DISCOMFORT – AFTERPAINS – IMMOBILITY – DIAPHORESIS – SUPPRESION OF LACTATION – PROMOTION OF REST