UTI
advertisement

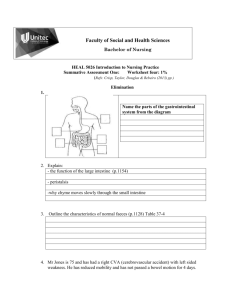
Urinary Tract Infection Michele Ritter, M.D. Argy Resident – Feb. 2007 Urinary Tract Infection Upper urinary tract Infections: Pyelonephritis Lower urinary tract infections Cystitis (“traditional” UTI) Urethritis (often sexually-transmitted) Prostatitis Symptoms of Urinary Tract Infection Dysuria Increased frequency Hematuria Fever Nausea/Vomiting (pyelonephritis) Flank pain (pyelonephritis) Findings on Exam in UTI Physical Exam: CVA tenderness (pyelonephritis) Urethral discharge (urethritis) Tender prostate on DRE (prostatitis) Labs: Urinalysis + leukocyte esterase + nitrites More likely gram-negative rods + WBCs + RBCs Culture in UTI Positive Urine Culture = >105 CFU/mL Most common pathogen for cystitis, prostatitis, pyelonephritis: Escherichia coli Staphylococcus saprophyticus Proteus mirabilis Klebsiella Enterococcus Most common pathogen for urethritis Chlamydia trachomatis Neisseria Gonorrhea Lower Urinary Tract Infection Cystitis Uncomplicated (Simple) cystitis Complicated cystitis In healthy woman, with no signs of systemic disease In men, or woman with comorbid medical problems. Recurrent cystitis Uncomplicated (simple) Cystitis Definition Diagnosis Dipstick urinalysis (no culture or lab tests needed) Treatment Healthy adult woman (over age 12) Non-pregnant No fever, nausea, vomiting, flank pain Trimethroprim/Sulfamethoxazole for 3 days May use fluoroquinolone (ciprofoxacin or levofloxacin) in patient with sulfa allergy, areas with high rates of bactrimresistance Risk factors: Sexual intercourse May recommend post-coital voiding or prophylactic antibiotic use. Complicated Cystitis Definition Diagnosis Females with comorbid medical conditions All male patients Indwelling foley catheters Urosepsis/hospitalization Urinalysis, Urine culture Further labs, if appropriate. Treatment Fluoroquinolone (or other broad spectrum antibiotic) 7-14 days of treatment (depending on severity) May treat even longer (2-4 weeks) in males with UTI Special cases of Complicated cystitis Indwelling foley catheter Try to get rid of foley if possible! Only treat patient when symptomatic (fever, dysuria) Leukocytes on urinalysis Patient’s with indwelling catheters are frequently colonized with great deal of bacteria. Should change foley before obtaining culture, if possible Candiduria Frequently occurs in patients with indwelling foley. If grows in urine, try to get rid of foley! Treat only if symptomatic. If need to treat, give fluconazole (amphotericin if resistance) Recurrent Cystitis Want to make sure urine culture and sensitivity obtained. May consider urologic work-up to evaluate for anatomical abnormality. Treat for 7-14 days. Pyelonephritis Infection of the kidney Associated with constitutional symptoms – fever, nausea, vomiting, headache Diagnosis: Treatment: Urinalysis, urine culture, CBC, Chemistry 2-weeks of Trimethroprim/sulfamethoxazole or fluoroquinolone Hospitalization and IV antibiotics if patient unable to take po. Complications: Perinephric/Renal abscess: Suspect in patient who is not improving on antibiotic therapy. Diagnosis: CT with contrast, renal ultrasound May need surgical drainage. Nephrolithiasis with UTI Suspect in patient with severe flank pain Need urology consult for treatment of kidney stone Prostatitis Symptoms: Diagnosis: Typical clinical history (fevers, chills, dysuria, malaise, myalgias, pelvic/perineal pain, cloudy urine) The finding of an edematous and tender prostate on physical examination Will have an increased PSA Urinalysis, urine culture Treatment: Pain in the perineum, lower abdomen, testicles, penis, and with ejaculation, bladder irritation, bladder outlet obstruction, and sometimes blood in the semen Trimethoprim/sulfamethoxazole, fluroquinolone or other broad spectrum antibiotic 4-6 weeks of treatment Risk Factors: Trauma Sexual abstinence Dehydration Urethritis Chlamydia trachomatis Frequently asymptomatic in females, but can present with dysuria, discharge or pelvic inflammatory disease. Send UA, Urine culture (if pyuria seen, but no bacteria, suspect Chlamydia) Pelvic exam – send discharge from cervical or urethral os for chlamydia PCR Chlamydia screening is now recommended for all females ≤ 25 years Treatment: Azithromycin – 1 g po x 1 Doxycycline – 100 mg po BID x 7 days Neisseria gonorrhoeae May present with dysuria, discharge, PID Send UA, urine culture Pelvic exam – send discharge samples for gram stain, culture, PCR Treatment: Ceftriaxone – 125 mg IM x 1 Cipro – 500 mg po x 1 Levofloxacin – 250 mg po x 1 Ofloxacin – 400 mg po x 1 Spectinomycin – 2 g IM x 1 You should always also treat for chlamydia when treating for gonnorhea! Question #1 An 18-year old woman presents with urinary frequency, dysuria, and lowgrade fever. Urinalysis shows pyuria and bacilli. She has never had similar symptoms or treatment for urinary tract infection. Question # 1 What category of UTI does this patient have? Does this patient require further testing? Would you treat this patient, and if so, with what and how long? Question # 2 An 18-year old woman present with her third episode of urinary frequency, dysuria, and pyuria in the past 4 months. Question # 2 What further questions do you have for this patient? What type of UTI does this patient have? What testing might you perform in this patient? How would you treat her, and for how long? Question #3 A 24-year old woman presents with fever, chills, nausea, vomiting, flank pain and tenderness. Her temperature is 40°C, pulse rate is 120/min., and blood pressure is 100/60 mm Hg. Question # 3 What further studies do you want in this patient? How would you treat this patient? What might you do if she does not improve after 3-4 days? Question # 4 A 78-year old female presents with an indwelling foley catheter and pyuria. Question # 4 What would you do for this patient at this time? How might your work-up/management change if she was having fevers and confusion? Question # 5 58-year old man presents with his first episode of urinary frequency and dysuria. Urinalysis shows pyuria and bacilli. Question # 5 What type of UTI does this patient likely have? How would you treat this man, and for how long? What activities would put this patient at risk for UTI? Question # 6 A 28-year old male had a sexual encounter with a prostitute while on a business trip in Seattle 1 week ago. After returning home, he noted a burning sensation on urination and a yellow discharge in his underwear. Microscopic examination of the discharge reveals 4+ leukocyte esterase, and the following gram stain. Question # 6 Question # 6 Which of the following is the best course of action for this patient? a) Give the patient a prescription for doxycycline, 100 mg po BID for 7 days Give the patient two prescriptions for ofloxacin 300 mg po QDay for 7 days, one for him, and one for his wife. Administer ceftriaxone – 125 mg IV x 1 and Azithromycin – 1 g po x 1, draw blood for a VDRL and HIV – antibody arrange for his wife to be examined and treated. Administer a single dose of Ceftriaxone – 125 mg IV x 1, and ciprofloxacin – 500 mg po x 1 draw blood for a VDRL and HIVantibody, and arrange for his wife to be examined and treated. Administer a single dose of cefixime – 400 mg, draw blood for a VDRL and arrange for his wife to be examined and treated. b) c) d) e) Final thoughts! Antibiotic choice and duration are determined by classification of UTI. Biggest bugs for UTI are E. Coli, Staph. Saprophyticus, Proteus mirabilis, Enterococci and gram-negatives Don’t use moxifloxacin for UTI! Chlamydia screening is now recommended for all women 25 years and under since infection is frequently asymptomatic, and risk for PID/infertility is high!