SAED Recert - Hamilton Health Sciences
advertisement

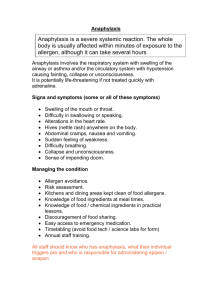
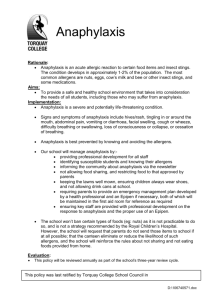
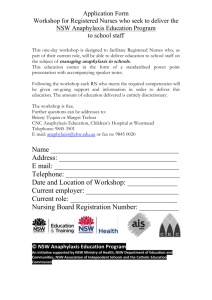
ANAPHYLAXIS Prepared by: South West Education Committee Anaphylaxis Protocol South West Education Committee SWEC MEMBERS Cambridge – Lori Smith Grey Bruce – Andy Whittemore Hamilton – Ken Stuebing, Tim Dodd Lambton – Judy Potter London – Tre Rodriguez Niagara – Greg Soto Windsor – Cathie Hedges RTN – Peter Deryk “The Power of 7” Base Hospital Programs Goal: One single certification for all of SouthWestern Ontario by Fall 2005!! Recert process same across SW this year. Notice, all paperwork will say SWEC. Some information may not be specific to Hamilton BH or Services in our area. Pictures for data base in one of the stations OBJECTIVES Review basic pathophysiology of Anaphylaxis Review Anaphylaxis. At the end of this session you should be able to describe and explain: Anaphylaxis and its’ treatment protocols. ANAPHYLAXIS An immediate, systemic, life-threatening allergic reaction associated with major changes in the cardiovascular, respiratory and cutaneous systems. – Prompt recognition and appropriate drug therapy are important to patient survival. Pathophysiology of anapnylactic shock. PATHOPHYSIOLOGY A, B, C, … Assess the patient’s… Airway (do they have one? Can they maintain it? Breathing (are they) Circulation (pulses) ECG (Is the monitor on?) ASSESSMENT What is the patients chief complaint? Possible anaphylaxis? If “NO” then assess treat & transport. If ‘YES” get a Hx. REVIEW Chief Complaint – One or more symptoms for which the patient is seeking medical care – Most chief complaints are characterized by: • • • • Pain Abnormal function A change in the patient's normal state An unusual observation made by the patient (e.g., heart palpitations) REVIEW Chief Complaint – Be alert to the possibility that a chief complaint may be misleading or that a problem may be more serious than the patient's chief complaint The patient – May not be exactly sure what is bothering him/her ANAPHYLAXIS If you suspect anaphylaxis then: Get a history of present illness (HPI). Be thorough, yet time efficient. REVIEW History of Present Illness (HPI) – Identifies the chief complaint and provides a full, clear, chronological account of the symptoms – A thorough HPI requires skill in: • Asking appropriate questions related to the chief complaint • Interpreting the patient's response to those questions ANAPHYLAXIS Assess/obtain the patients vitals. – Level of Consciousness – Blood Pressure – Pulse/ECG – Respiratory rate – Capillary refill – SpO2 reading – Skin ALLERGIES Did you ask about allergies? Did you look for a medical alert tag? If unconscious, check for a medic alert tag. ANAPHYLAXIS – S&S Wheezing Stridor Hypotension (systolic less than 90) Decreased LOC Airway compromise Edema Urticaria ( with at least one of the above) ANAPHYLAXIS ? Does your exam identify: Generalized urticaria? Generalized or local edema? What does Urticaria look like? U rticaria as a result of an allergic reaction. TUNNEL VISION Generalized urticaria!!! How is the patients airway? ANAPHYLAXIS - SOB On exam do you note/observe any of the following? Wheezing? Stridor? Shortness of breath? ANAPHYLAXIS - SOB If yes, then begin treatment. Remember urticaria must be accompanied with wheezing and/or stridor, etc. ANAPHYLAXIS - TREATMENT Oxygen–NRB @ 15 L/min. Epinephrine 1:1000 If 30 kg give 0.3 mg If 30 kg give 0.1 mg/10 kg rounding to nearest 0.05 mg. WHY EPINEPHRINE? Increases vascular smooth muscle tone (alpha agonist). Decreases tone in alveolar smooth muscle (beta agonist). ANAPHYLAXIS TREATMENT Reassess patient Be prepared to control their airway. BVM Suction ANAPHYLAXIS TREATMENT Repeat Epi x 1 if: Condition does not improve after 10 minutes. Patient deteriorates. ANAPHYLAXIS TREATMENT Remember OMITR Oxygen Monitor Intervention(s) Transport ASAP Reassess often SUMMARY If patient has self-administered, follow the rules for a second administration Following 1st Epi. If wheezing develops or is present consider the SOB protocol. Urticaria alone is not an indicator for Epi.! QUESTIONS?