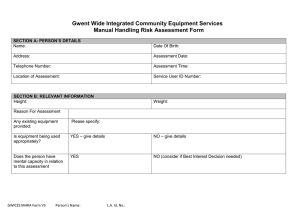
Gwent Wide Integrated Community Equipment Services
Manual Handling Risk Assessment Form
SECTION A: SERVICE USER AND ASSESSOR DETAILS
Name:
Address:
Telephone Number:
SSID/ NHS Number:
Date Of Birth:
Assessment Date:
Assessment Time:
Location of Assessment: (If different to Address)
Name of Assessor:
Designation:
Organisation/Department:
Contact Number:
SECTION B: CLIENT LOAD
Height:
Stature:
Reason For Assessment
Weight:
Small
Any existing equipment:
Are carers present at time
of assessment and using
existing equipment
appropriately?
Mental Capacity
MHRAF
YES (please specify and check
condition)
Medium
Tall
NO
YES
NO
YES
NO (consider Best Interest Decision tool)
Status
1
Relevant Medical
Condition
2
Pain Status
3
History of Falls
4
5
Hearing / Vision
Speech (include
language,
communication)
Skin conditions
including tissue
viability
Seizures / involuntary
movements
Postural stability
(include sitting,
standing, balance,
head control)
Muscle tone/
contractures
Attachments /
Prosthetics
Continence
Cognitive /
behavioural (include
capacity issues)
Day / Night Variations
6
7
8
9
10
11
12
13
MHRAF
Comments
SECTION C: TASKS
Status
1
Ability to weight bear
Hazards Identified
YES
NO
2
Mobility
YES
NO
3
Bed - In and Out
YES
NO
4
Bed - Up and Down
YES
NO
5
Bed - Turning
YES
NO
6
Bed - Sitting
YES
NO
7
Chair – Sit to Stand
YES
NO
8
Chair – Repositioning
YES
NO
9
Toileting
YES
NO
10
Personal Care and Dressing
YES
NO
11
Bathing/Showering
YES
NO
12
Stairs/Steps
YES
NO
13
Other
YES
NO
MHRAF
Comments
SECTION D: ENVIRONMENT
Status
1
Space Constraints (for handler and
equipment movement)
2
Hazards Identified
YES
NO
Are the floor coverings appropriate to
allow ease of movement of equipment to
be used? (i.e. corridors / thresholds)
Furniture, i.e. height, suitable for
equipment?
Access (e.g. to bed, bath, W/C and
passage ways)
YES
NO
YES
NO
YES
NO
5
Access to Property e.g. Stairs/Steps
YES
NO
6
Equipment power supply
YES
NO
7
Sleeping in room with a gas fire?
YES
NO
8
YES
NO
9
Is the temperature, Humidity and Lighting
adequate?
Pets at property?
YES
NO
10
Small Children at property?
YES
NO
11
Other
YES
NO
3
4
MHRAF
Comments
SECTION E: CARER/HANDLER
Name of Carer Present
Status
Comments
Have named informal/formal carers received
appropriate demonstrations of use of
equipment?
YES
NO
Is special training required for equipment to be
issued? (in addition to foundation training)
YES
NO
Is special equipment and or clothing required?
(i.e. gloves, apron)
YES
NO
Are the carers at risk of poor posture during the
task? (bending, twisting, stooping, reaching ,
etc.)
YES
NO
Are there specific hazards to those with existing
health problems (or pregnancy)?
YES
NO
MHRAF
SECTION F: RISK REDUCTION PLAN
Concern/Difficulty/Hazard Identified
Action Required
Clinical Reasoning
By Whom
Date Completed
Review Date
Have other options been considered and rejected, if so, please state reasons
1.
2.
3.
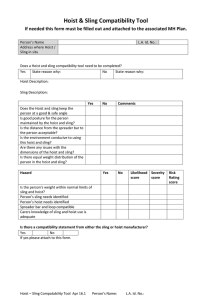
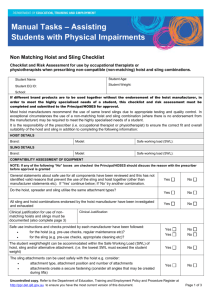
SECTION G: HOIST AND SLING COMPATIBILITY TOOL
Does a Hoist and sling compatibility tool need to be completed?
YES
State reason why:
HOIST AND SLING ASSESSMENT
Equipment Assessed With
Hoist:
MHRAF
Make/Model/Size
NO
State reason why:
(If No, go to Handling Plan)
Sling :
HOIST AND SLING EVALUATION
Yes
No
Comments
Does the Hoist and sling keep the person at a good &
safe angle
Is good posture for the person maintained by the hoist
and sling?
Is the distance from the spreader bar to the person
acceptable?
Spreader bar and loop compatible
Is there a compatibility statement from either the sling or hoist manufacturer?
YES
If yes please attach to this form.
Signature
Occupational Therapist:
Print name:
Signature:
Organisation/Department:
Designation:
Date:
MHRAF
NO
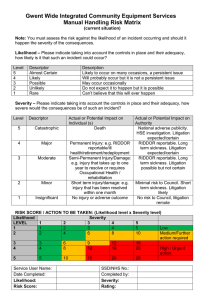
Gwent Wide Integrated Community Equipment Services
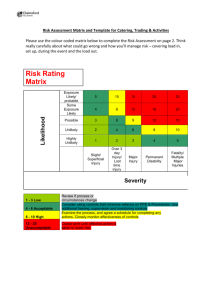
Manual Handling Risk Matrix
(current situation)
Note: You must assess the risk against the likelihood of an incident occurring and should it happen the severity of the consequences.
Likelihood – Please indicate taking into account the controls in place and their adequacy, how likely is it that such an incident could occur?
Level
5
4
3
2
1
Descriptor
Almost Certain
Likely
Possible
Unlikely
Rare
Description
Likely to occur on many occasions, a persistent issue
Will probably occur but it is not a persistent issue
May occur occasionally
Do not expect it to happen but it is possible
Can’t believe that this will ever happen
Severity – Please indicate taking into account the controls in place and their adequacy, how severe would the consequences be of such an
incident?
MHRAF
Level
Descriptor
Actual or Potential Impact on Individual (s)
5
Catastrophic
Death
4
Major
Permanent Injury: e.g. RIDDOR reportable/ill
health/retirement/redeployment
3
Moderate
2
Minor
1
Insignificant
Semi-Permanent Injury/Damage: e.g. injury that
takes up to one year to resolve or requires
Occupational Health / rehabilitation
Short term injury/damage: e.g. injury that has been
resolved within one month
No injury or adverse outcome
Actual or Potential Impact on
Authority
National adverse publicity. HSE
investigation. Litigation
expected/certain
RIDDOR reportable. Long term
sickness. Litigation
expected/certain
RIDDOR reportable. Long term
sickness. Litigation possible but
not certain
Minimal risk to Council. Short
term sickness. Litigation likely
No risk to Council, litigation
remote
RISK SCORE / ACTION TO BE TAKEN: (Likelihood level x Severity level)
MHRAF
Likelihood
LEVEL
1
2
1
1
2
2
2
4
3
4
3
4
6
8
5
5
10
Severity
3
3
6
4
4
8
5
5
10
9
12
12
16
15
20
15
20
25
Service User Name:
Date Completed:
SSD/NHS No.:
Completed by:
Likelihood:
Risk Score:
Severity:
Rating:
Low
Medium/Further action
required
High / Urgent action
 0
0