Granuloma formation?

Understanding granuloma formation in TB using different mathematical and biological scales
Denise Kirschner, Ph.D.
Dept. of Microbiology/Immunology
Univ. of Michigan Medical School
Outline of Presentation
• Introduction to TB immunobiology
• Studying the host-pathogen interaction
• Experimental Methods
• ODE model, 2-compartmental model, metapopulation model, agent-based model
• Granuloma Structure and Function
• Results
• Compare dynamics and bifurcation parameters for each approach
Mycobacterium tuberculosis
• 1/3 of the world infected
• 3 million+ die each year
• no clear understanding of distinction between different disease trajectories:
Exposure
70%
30%
No infection
5%
Infection
95%
Acute disease
Latent disease
5-10%
Reactivation
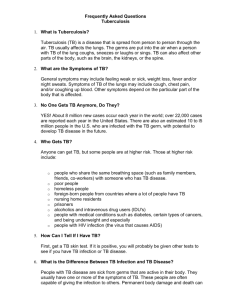
HUMAN GRANULOMA- snap shot
Cell mediated immunity in
M. tuberculosis
infection
• What elements of the host-mycobacterial dynamical system contribute to different disease outcomes once exposed?
• Hypothesis: components of the cell mediated immune response determine either latency or active disease (primary or reactivation)
• Wigginton and Kirschner J Immunology 166:1951-1976,
2001
Cellmediated
Immunity:
Activated
M
F s
Humoralmediated immunity
cytokines and T cells : green=upregulation, red=downregulation black=production,
Experimental Approach
• Build a virtual model of human TB describing temporal changes in broncoalveolar lavage fluid (BAL) to predict mechanisms underlying different disease outcomes
• Use model to ask questions about the system
Methodology for TB Model
• Describe separate cellular and cytokine interactions
• Translate into mathematical expressions
• nonlinear ordinary differential equations
• Estimate rates of interactions from data
(parameter estimation)
• Simulate model and validate with data
• Perform virtual experiments
Variables tracked in our model:
• Macrophages: resting, activated, chronically infected
• T cells: Th0, Th1, Th2
• Cytokines: IFNg, IL-4, IL-10, IL-12
• Bacteria: both extracellular and intracellular
• Define 4 submodels
Parameter Estimation: inclusion of experimental data
• Estimated from literature giving weight to humans or human cells and to species
M. tuberculosis over other mycobacteria
• Units are cells/ml or pg/ml of BAL
• Sensitivity and Uncertainty analyses can be performed to test these values or estimate values for unknown parameters
Example: estimating growth rate of M. tuberculosis
• in vitro estimates for doubling times of
H37Rv lab strain within macrophages ranged from 28 hours to 96 hours
• In mouse lung tissue, H37Rv estimated to have a doubling time of 63.2 hours
• We can estimate the growth rates of intracellular vs. extracellular growth rates from these values (rate=ln2/doub. time )
Model Outcomes: Virtual infection within humans over 500 days
• No infection - resting macrophages are at their average value in lung (3x10 5 /ml)
(negative control)
• Clearance - a small amount of bacteria are introduced and infection is cleared (PPD-)
• latent TB (a few macrophages harbor all may miss them in biopsy)
• Active, primary TB
What determines these different outcomes?
*Detailed Uncertainty and Sensitivity
Analyses on all parameters in the system
Latin Hypercube Sampling
Partial Rank Correlation
Varying T cell killing of infected macrophages
Total T cells
Total bacteria
Factors leading to different disease outcomes-Model 1
• Production of IL-4
• Rates of macrophage activation, deactivation and infection
• Rate T cells lyse infected macrophages
Rate extracellular bacteria are killed by activated macrophages
• *Production of IFNg from NK and CD8 cells
Virtual Deletion and
Depletion Experiments:
• Deletion: mimic knockout (disruption) experiments where the element is removed from the system at day 0. Ask: what parameters contribute to achieving latency?
• Depletion: mimic depletion of an element by setting it to zero after latency is achieved. Ask: what maintains latency after it has been achieved?
Depletion Experiments
• IFNg : progress to active disease within
500 days
• IL-12: still able to maintain latency; much higher bacterial load
• IL-10:
IL-10 Depletion
Multiple Compartments- spatial component within the immune system
Site of infection- lung
Lymph nodes- site of adaptive immunity
Trafficking between sites
Specialized cells: Dendritic cells
Immune priming
Activation and differentiation
Marino, S and Kirschner, D. The Role of Dendritic cells in the
Human Immune Response to Mycobacterium tuberculosis in the lung and lymph node.
Journal of Theoretical Biology, (in press), 2004 . – and another submitted.
Factors leading to different disease outcomes-Model 2
•
•
• Rates of macrophage activation, deactivation and infection
Rate T cells lyse infected macrophages
Production of IFNg from NK and CD8 cells
• DC-T cell interaction rates, IL-12 prod. rate, DC turnover rate, DC migration rate
• Growth Rate of extracellular bacteria
• Rate new Th0 cells migrate out of LN to inf. site
Importance of A Spatial
Response at the site:
•
•
Granuloma formation?
• Cells respond to chemotatic signals
• Other?
Granuloma function?
• ‘wall off’ infection – bacterial spread
• Minimize tissue damage
• Provide a localized environment for cell to cell interactions
Host response to M.tbdevelopment of granuloma:
DTH/Th1 response
Large necrotic
Small solid
Spatio-temporal models of granuloma formation
• Metapopulation Model
• (Drs. S. Ganguli & D. Gammack)
• Agent based model
• (Drs. J. Segovia-Juarez & S. Ganguli)
• PDE model- tracked only innate immunity and early macrophage response (Dr. D. Gammack)
• Gammack D, Doering C, and Kirschner D. Macrophage response to
Mycobacterium tuberculosis infection. Journal of Mathematical
Biology. Vol 48( 2) February 2004, Pages: 218 - 242
.
•Metapopulation Modeling
• Ganguli S, Gammack D, and Kirschner D .
A metapopulation model of granuloma formation in the lung during infection with M. tuberculosis.
(Submitted)
Discrete Spatial Model of Granuloma Development
• Partition space: nxn lattice of compartments
• Model diffusion between compartments
• movement based on local differences (gradient)
• Probabilistic movement
• Model interactions within compartments
• Existing temporal model n 2 Systems of ODEs
10mm x10mm
Modeling diffusion
Example:
• Chemokine C diffuses out from a source
C
Modeling diffusion
Example:
• Chemokine C diffuses out from a source
• Diffusion of macrophages M is biased towards higher concentrations of C
C
M
Metapopulation model: simulation of containment
•
•
Factors leading to different disease
• outcomes-Model 3
Rates of macrophage activation, deactivation and infection
Rate T cells lyse infected macrophages Rate extracellular bacteria are killed by activated macrophages
Growth rate of extracellular bacteria
• Rate of recruitment of Macrophages and T cells via chemokine
• Rate that activated macrophages and T cells move about the infection site
• Rate of chemokine diffusion
•Agent Based Modeling
• Jose Segovia-Juarez, Suman Ganguli and D.
Kirschner. An agent based model of granuloma formation in the lung during infection with M. tuberculosis (submitted).
Model Agents
DISCRETE ENTITIES
• Cells
• Macrophages in different states: Activated,
Resting, Infected and Chronically infected
• Effector T cells
CONTINUOUS ENTITIES
• Chemokine
• Extracellular mycobacteria
Macrophage state diagram
Model Framework: lattice with agents and continuous entities
Vascular sources of cells
Rules: an example
Resting macrophage phagocytosis
Rules: an example
Macrophage activation by T cells
Granuloma formation-solid
Resting macrophages
Infected macrophages
Chronically infected m.
Activated macrophage
Bacteria
T cells
Necrosis
Granuloma formation-necrotic
Resting macrophages
Infected macrophages
Chronically infected m.
Activated macrophage
Bacteria
T cells
Necrosis
Granuloma formation- clearance
Resting macrophages
Infected macrophages
Chronically infected m.
Activated macrophage
Bacteria
T cells
Necrosis
2x2 mm sq.
Adaptive Immunity: T cell arrival delay to infectionsite
Panel A: parameters that lead to containment
Panel B: parameters that least to disseminative disease
How robust are the simulations with stochastic elements?
Factors determining successful granuloma formation-Model 4
•
•
•
Rate of recruitment of Macrophages and T cells via chemokine
Rate that activated macrophages and T cells move about the infection site
Rate of chemokine diffusion
Intracellular bacteria load that converts macrophages chronically infected
Number of times it takes to count region as necrotic
Number of initial resting macrophages
Can we determine granuloma function from form?
Results indicate that how the granuloma forms and is maintained can determine whether infection is contained or spreads locally within the lung
This is dependent on a number of factors:
Crowding of cells within the granuloma
This does not allow for T cells to penetrate and activate macrophages
Necrotic regions containing bacteria
This walls off bacteria from macrophages and spread
Can we predict the human outcome?
*How do we extrapolate from a single granuloma to predict infection outcome?
*Emile et al(1997) in J. of Path.
Identified 14 patients with BCG-disease each of whom had either latent, suppressed infection or acute disease. All granulomas were distinct and uniform within the two groups (solid or caseated)
Present work- expanding our ABM studies
Collaborating with studies on NHP models of TB
Exploring specific role of cytokines and specific cellular subsets in granuloma formation
Heterogeneous lattice representing the lung environment
3-D representation of the granuloma
Kirschner Lab
• Jose S.-Juarez, PhD
• David Gammack, PhD
• Simeone Marino, PhD
• Suman Ganguli, PhD
• Ping Ye, PhD
• Seema Bajaria, MS
• Ian Joseph
• Christian Ray
• Stewart Chang
• Dhruv Sud
• Joe Waliga
Acknowledgments
NIH and The Whitaker Foundation
•Collaborators: JoAnne Flynn (Pitt)
•John Chan (Albert Einstein)
Present Work- cellular level
• Include in the temporal BAL model:
• CD8+ T cells and TNFa ( D. Sud)
• IL-10 as a regulator of the immune response (S. Marino)
Present Work: intracellular level
• Temporal specificity by M. tuberculosis inhibiting antigen presentation in macrophages (S. Chang)
• The balance of activation, killing and iron homeostasis in determining M. tuberculosis survival within a macrophage (Christian Ray)