File - (LMG) Project
advertisement
 Project")
Leadership, Management and Governance (LMG) Project
Inspired Leadership. Sound Management. Transparent Governance.
Cooperative Agreement Number AID-OAA-A-11-00015
SYNTHESIS PAPER ON EFFECTIVE GOVERNANCE FOR HEALTH
DATE: 30 June 2012
Submitted to:
Brenda A. Doe
Deputy Division Chief, Services Delivery Improvement Division
Room 3.6-123, Office of Population & Reproductive Health
Bureau of Global Health, USAID
1300 Pennsylvania Avenue, N.W., Washington, D.C. 20523
Submitted by:
Management Sciences for Health (MSH)
James A. Rice, Ph.D.
Project Director, Leadership, Management and Governance Project
In Collaboration with:
Implementing project partners include the African Medical and Research Foundation, International
Planned Parenthood Federation, Johns Hopkins University Bloomberg School of Public Health, Medic
Mobile, and Yale University Global Health Leadership Institute.
Acronyms
GEN-RH Global Exchange Network for Reproductive Health
LMG Leadership, Management and Governance Project
MSH Management Sciences for Health
OECD Organisation for Economic Co-operation and Development
USA United States of America
USAID Untied States Agency for International Development
WHO World Health Organization
Funding was provided by the United States Agency for International Development (USAID) under Cooperative Agreement
AID-OAA-A-11-00015. The contents are the responsibility of the Leadership, Management, and Governance Project and do
not necessarily reflect the views of USAID or the United States Government.
2 LMG Project Year 1
September 2011 – June 2012
Table of Contents
Abstract ......................................................................................................................................... 5
Introduction .................................................................................................................................. 7
Methods ......................................................................................................................................... 9
Quantitative survey ................................................................................................................... 9
In-depth interviews.................................................................................................................... 9
Results ......................................................................................................................................... 10
Quantitative survey ................................................................................................................. 10
Respondent profile ................................................................................................................ 10
Elements or practices of governing....................................................................................... 11
Enablers and impediments for effective governance ............................................................ 12
Linkages between effective governance, improved health services, and improved health of
individuals and the population .............................................................................................. 13
Relationships and interaction between leadership, management, and governance .............. 14
Subgroup analysis ................................................................................................................. 14
In-depth interviews.................................................................................................................. 14
Respondent demographics .................................................................................................... 14
Participant experiences of leading, governing and managing ................................................. 16
What is governance? ............................................................................................................. 16
Elements or practices of governance .................................................................................... 16
Effective governance in the context of health....................................................................... 17
Linkage between governance and health outcomes .............................................................. 18
Measuring governance .......................................................................................................... 18
Gender in governance ........................................................................................................... 19
Inter-relationship and interaction of leadership, management and governance ................... 20
Discussion.................................................................................................................................... 20
Limitations .................................................................................................................................. 21
Quantitative survey ............................................................................................................... 21
In-depth interviews ............................................................................................................... 22
Policy Implications ..................................................................................................................... 22
References ................................................................................................................................... 25
Appendix ..................................................................................................................................... 27
Figures ..................................................................................................................................... 27
Tables ...................................................................................................................................... 39
Subgroup Analysis .................................................................................................................. 60
Gender ................................................................................................................................... 60
Sectors ................................................................................................................................... 61
3 LMG Project Year 1
September 2011 – June 2012
Levels .................................................................................................................................... 61
Country where respondent works ......................................................................................... 62
Geographical regions: Asia, Africa, Latin America and Caribbean ..................................... 63
Respondents who govern vs. respondents who manage but not govern ............................... 64
Respondents who govern vs. respondents who lead but not govern..................................... 65
Survey instruments .................................................................................................................. 66
Quantitative survey ............................................................................................................... 66
In-depth interview protocol................................................................................................... 73
4 LMG Project Year 1
September 2011 – June 2012
Abstract
Background
Poor governance, overall and especially in the health sector, has contributed to poor health
outcomes in many low and middle income countries. There is evidence in the literature that
shows effective governance improves health outcomes. Published empirical literature on how
people who lead, govern and manage perceive governance in the context of health is very
limited.
Methods
We sought to understand governance, and what makes it effective in the context of health from
the perspective of people who lead, govern or manage the health sector or the health institutions
in low and middle income countries through a quantitative on-line survey of 477 respondents in
80 countries in addition to a qualitative survey of 25 key informants in 16 countries.
Results
Our salient survey findings are (1) Those who lead, govern and manage the health sectors and
health institutions are likely to define effective governance in terms of improvements in both the
health services and the health of individuals and populations. Many (more females than males)
see a clear link between governance in sectors other than health as having an effect on the health
of individuals and populations. (2) Leadership, management, and governance are highly interlinked and mutually reinforcing constructs in the context of health. Leaders are critical to the
governing process, and effective leadership is a prerequisite for effective governance and
effective management. (3) Including the governed in the governing process, steering and
regulation, collaboration across ministries, sectors and levels, and oversight were judged to be
highly significant elements of the governing process. (4) Competent leaders with ethical and
moral integrity, measurement and use of data, sound management, adequate financial resources
available for governing, openness and transparency, participatory decision making,
accountability to the citizens and clients, use of scientific evidence and effective governance in
sectors other than health, and governing using technology were judged as the top enablers of
effective governing in the context of health. (5) Governance needs to be gender aware, gender
responsive, and gender transformative in order to be effective.
Conclusion
Leaders who govern in low and middle income countries and who wish to achieve better health
outcomes for their constituents should, according to their peers, consider cultivating integrity,
transparency, accountability, leadership, community participation, intersectoral collaboration,
performance measurement, and gender responsiveness; and use technology as they foster these
attributes in their governing.
Keywords
Governance, governing, effective governance, governance for health, governing for health,
deterrents, enablers, practices, measuring governance, gender in governance, leadership,
management
5 LMG Project Year 1
September 2011 – June 2012
KEY MESSAGES
Effective governance in the context of health is governance that leads to improvements in
both the health services and the health of individuals and populations.
Leaders are critical to the governing process, and effective leadership is a prerequisite for
effective governance and effective management.
Including the governed in the governing process, steering and regulation, collaboration across
ministries, sectors and levels, and oversight were judged to be highly significant elements of
the governing process.
Top enablers of effective governing in the context of health include: competent leaders with
ethical and moral integrity, measurement and use of data, sound management, adequate
financial resources available for governing, openness and transparency, participatory decision
making, accountability to the citizens and clients, use of scientific evidence, and effective
governance in other sectors.
6 LMG Project Year 1
September 2011 – June 2012
Introduction
Poor governance, overall and especially in the health sector, has contributed to poor health
outcomes in many low and middle income countries. Our review of literature shows this link
between governance and health outcomes. Gupta et al. (2000) showed that levels of corruption
are clearly related to child mortality and other health outcomes, and a two-point improvement in
the integrity of government would reduce child mortality by 20%. Corruption was found to be
negatively associated with the quality of health services as proxied by the health staff’s
knowledge on required immunizations (Azfar, et al. 2001). A study of 64 countries found that
corruption lowered public spending on education, health and social protection (Delavallade
2006). Lindelow and Serneels (2006) in their focus group discussions with health workers and
users of health services found the failure of government policies and weak accountability
mechanisms as two of the four structural reasons for performance problems in the health sector.
Controlling for several variables including female education, income, urbanization, and distance
from the equator, Rajkumar and Swaroop (2008) showed that public health spending has a
greater effect on child and infant mortality the higher is the quality of government– measured
both as the absence of corruption and the quality of the bureaucracy.
There is further evidence that shows that effective governance improves health outcomes. Public
health spending lowers child mortality rates more in countries with good governance, and the
differences in the efficacy of public spending can be largely explained by the quality of
governance (Rajkumar and Swaroop 2008). Governance was strongly associated with under-five
mortality rate, and after controlling for possible confounding by healthcare, finance, education,
and water and sanitation, governance remained significantly associated with it (Olafsdottir et al.
2011). Probably the best evidence comes from the randomized field experiment conducted by
Björkman and Svensson (2009) in fifty rural communities of Uganda to see if community
monitoring of providers improves health outcomes. In the treatment group, a community, with
the help of a local community-based organization, monitored primary health care providers of
the public dispensary for a year using a citizen report card. At the end of one year, they found
that community monitoring had increased the quality and quantity of primary health care;
utilization of out-patient services was 20 percent higher in treatment communities; treatment
practices, examination procedures, and immunization coverage all improved; and perhaps most
importantly, there was a significant increase in weight of infants and as much as 33 percent
reduction in under-5 mortality in the treatment communities as opposed to the control
communities. In an experimental analysis, Barr et al. (2009) found that monitors are more
vigilant when they are elected by service recipients, and service providers perform better when
they are monitored by monitors so elected.
Since governance appeared to directly impact health system performance and health outcomes,
leadership and governance became salient during the past decade. Saltman and Ferroussier-Davis
(2000) had reviewed the concept of stewardship as a model of governance in the context of
World Health Report 2000 (Reinhardt and Cheng 2000) and defined it as a pursuit of policymaking that is both ethical and efficient. Different conceptual frameworks have been proposed
since then to define and measure governance in the context of health. Siddiqi et al. (2009) have
considered four existing frameworks: the World Health Organization’s domains of stewardship;
the Pan American Health Organization’s essential public health functions; the World Bank’s six
basic aspects of governance; and the United Nations Development Programme principles of good
7 LMG Project Year 1
September 2011 – June 2012
governance. Based on their review of existing frameworks, Siddiqi et al. proposed their Health
System Governance assessment framework that has 10 principles that underpin 63 broad
questions ranging from contextual and descriptive to process and outcome-related.
Recently, Veillard et al. (2011) revisited the concept of stewardship through a multidisciplinary
review of the literature and derived an operational framework comprising six functions of
stewardship for assessing the overall stewardship function of national health ministries.
Kickbusch and Gleicher (2011) advise combining whole-of-government and whole-of-society
approaches in their study conducted for the WHO Regional Office for Europe. They define smart
governance for health in terms of how governments approach governance challenges
strategically in five dimensions; by 1) governing through collaboration (how the state and society
co-govern), 2) governing through citizen engagement, 3) governing by a mix of regulation and
persuasion, 4) governing through independent agencies and expert bodies, and 5) governing by
adaptive policies, resilient structures and foresight. Mikkelsen-Lopez et al. (2011) proposed a
framework based upon a systems thinking approach, which is problem-driven and considers the
major health system building blocks at various levels in order to ensure a complete assessment of
a governance issue with a view to strengthen system performance and improve health.
Health Systems 20/20, a USAID-funded project, measured five dimensions of governance in the
health sector: information/assessment capacity, policy formulation and planning, social
participation and system responsiveness, accountability, and regulation. Brinkerhoff and Bossert
(2008) define good health governance in terms of roles and responsibilities and relationships that
are governed by; 1) responsiveness to public health needs and beneficiaries’ or citizens’
preferences while managing divergences between them; 2) responsible leadership to address
public health priorities; 3) the legitimate exercise of beneficiaries’/citizens’ voice; 4) institutional
checks and balances; 5) clear and enforceable accountability; 5) transparency in policymaking,
resource allocation, and performance; 6) evidence-based policymaking; and 7) efficient and
effective service provision arrangements, regulatory frameworks, and management systems.
Smith et al. (2012) present a cybernetic model of leadership and governance comprising three
fundamental functions: 1) priority setting, 2) performance monitoring and 3) accountability
mechanisms. In addition, there are frameworks that look at governance of a part of a health
system e.g. Good Governance in Medicines Framework of WHO (Anello 2008) and
Pharmaceutical Governance Model of USAID-funded Strengthening Pharmaceutical Systems
Project (SPS 2011).
Despite these advancements in the theoretical understanding of governance in the context of
health, there is very limited empirical literature on how people who lead, govern and manage in
low and middle income countries perceive effective governance in the context of health.
Systematically looking at governance in the context of health through the eyes of the people who
lead, govern and manage becomes important if the approaches, processes, models, interventions
and tools aimed at enhancing governance are to be firmly grounded in the perspectives of this
target population.
To add to the limited body of knowledge surrounding governance in health, we conducted a
quantitative survey of 477 health leaders, governors and managers from 80 countries and
qualitative in-depth interviews of 25 key health leaders, governors and managers from 16
8 LMG Project Year 1
September 2011 – June 2012
countries to assess their perceptions on effective governance in the contest of health. We report
the findings of these two surveys in this article.
Methods
The same set of research questions guided the quantitative and qualitative enquiries; these were:
what constitutes governance,
what constitutes effective governance,
what constitutes effective governance in the context of health,
what are the enablers and deterrents of governance,
how does governance relate to health system outcomes and health outcomes,
how is governance measured,
what are the gender issues involved in governance, and
how does governance, leadership and management interact in the context of health.
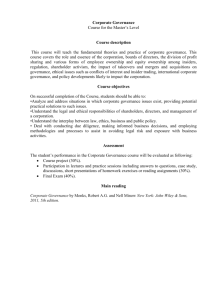
The two surveys sought perceptions and perspectives of the respondents on these questions. The
survey and interview instruments were created based upon a conceptual model of governance for
health depicted in Figure 1 in the Appendix. This governance model was derived from the
targeted literature review examined earlier in this paper as well as discussions with experts and
practitioners in the field, and also the findings of 2011 survey on governance for health. These
two instruments were extensively pilot-tested before administration. The New England
Institutional Review Board, via expedited review, approved the research protocol. The free and
informed consent of each key informant interviewees was obtained prior to the interview.
QUANTITATIVE SURVEY
The online survey was conducted between February 20 and March 24, 2012. The survey was
administered to the members of LeaderNet and the Global Exchange Network for Reproductive
Health (GEN-RH), two online communities of practice of health leaders, managers and those
who govern in the health sector. LeaderNet (http://leadernet.msh.org) is a global learning
community of managers who lead and leaders who govern in the health sector and in health
institutions. GEN-RH is a web-based network of individuals and organizations working in the
area of reproductive health. Management Science for Health (MSH) currently supports the two
communities of practice. A link to the survey instrument was sent via e-mail to approximately
6,000 health leaders, managers, and those who govern in public, private, and civil society sectors
in primarily low and middle income countries. The survey had 15 questions, and was
administered in English, Spanish, French and Portuguese. A total of 477 responses were received
from respondents who completed the survey in the following languages: English (274), Spanish
(122), French (66), and Portuguese (15). Survey response rate and other limitations are discussed
later in the paper. The survey data was analyzed using SAS (SAS Institute Inc., Cary, NC, USA).
IN-DEPTH INTERVIEWS
Using a purposeful sampling strategy, we recruited as our key informants people who lead,
govern, and manage the health sector (and other relevant sectors in a few instances) or the health
institutions in low and middle income countries who could provide insights into leading,
governing and managing as they relate to potential health outcomes. The informants were wellrespected health professionals in their countries and had no prior association with the
9 LMG Project Year 1
September 2011 – June 2012
organization (MSH) or the project (LMG Project) to which the researchers belonged. The
consenting informants were interviewed in person or on telephone by the principal investigator
or the associates using an open-ended interview guide (See Appendix). Seventeen (68%) of our
informants said they lead and govern, 5 (20%) informants said they lead and manage, and 3
(12%) said they lead. The goal was to interview those closely associated with the process of
governing. Those who lead and govern deliver governance decisions, and those who
predominantly lead and manage receive governance decisions. We tried to ensure that these
diverse perspectives are reflected in the study. The interview was semi-structured and an
informant was allowed to guide the conversation.
Interviews were conducted in Spanish 7 (28%) and in English 18 (72%). Spanish language
interviews were conducted by bilingual health services researchers. For analyses, all interviews
were transcribed and those interviews conducted in Spanish were translated into English. We
used bilingual interviewers in case of Spanish speaking interviewees and this may have increased
the likelihood of conceptual equivalence of issues thus reducing the potential for
misunderstanding and misinterpretation.
We generated an index of taxonomies, themes and subthemes based on our literature review,
findings of 2011 governance survey, discussion with experts, and patterns that emerged during
the key informant interviews. The text data resulting from interviews was coded by the two
researchers who compared their notes during and after the coding process. NVivo version 9 was
used for the data management and analysis. Analysis was an iterative process in which the
researchers collaborated to reach consensus on themes and sub themes at key points throughout
the research. Additional themes were added as they emerged. We searched the whole of the text
data for recurrent unifying concepts or statements while distilling themes and sub themes that
explain, predict, or interpret effective governance in the context of health and its link to health
system performance and health outcomes.
Results
QUANTITATIVE SURVEY
Respondent profile
A total of 477 leaders, managers and people who govern from 80 countries (See Table 1 in
Appendix) responded to the survey. Of the respondents, 60% were male and 40% were female.
The vast majority of respondents (88%) lived and worked in low and middle income countries.
By region, 48% of the respondents were from Africa, 35% from Latin America and the
Caribbean, 11% from Asia, and 6% from the USA, Canada, and Europe. When asked what sector
they work in, 50% of the respondents said that they work in the public sector, 27% in civil
society organizations, 15% in the private sector, and 8% in other sectors. By level of the health
system, 53% of the respondents work at the national level, 34% at the state level, and 41% at the
local level. The respondents could check multiple levels if they worked at multiple levels.
Seventeen percent (17%) work regionally with groups of nations. Less than 10% of the
respondents indicated they work at the global level.
10 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Viewed from the standpoint of the six WHO building blocks of health systems, most respondents
work within multiple health system building blocks with a focus on multiple service delivery
areas (See Figure 2 in Appendix). Each respondent was asked whether they lead, manage,
govern, and/or observe others govern: 85% reported that they lead, and 85% say they manage,
while only 32% reported that they govern. In addition, 85% stated that they observe others
govern (See Figure 3 in Appendix). About 30% of the respondents also stated that they lead,
manage, and govern. This indicates that there is a clear overlap among the roles of leading,
managing, and governing. No respondent stated he or she governs but does not manage or lead,
indicating that when governance is exercised it is done while leading and managing.
Respondents who govern also lead and manage. Respondents who manage also lead.
Elements or practices of governing
The survey sought to explore what governance means in practical terms for the respondents. In
other words, what do people who govern do to govern? The respondents were asked the degree
to which they consider each of the six practices indicated by an action verb in Table 2 and their
corresponding activities as part of the governing process. The action verbs were derived from the
targeted literature review and discussions with experts and practitioners in the field.
Table 2: Elements/Practices of governing
Practice
Steer
Regulate
Allocate
Include
Collaborate
Oversee
Activities
To identify a policy problem, to advocate policy, to set policy agenda, to have
a policy dialogue, to decide a strategic direction, to analyze policy options, to
make sound policies, and use continual learning in refining and adapting
policies for the future
To formalize policies through laws, regulations, rules of procedure, protocols,
standard operating procedures, or resolutions, etc.
To allocate responsibility of policy implementation and also authority and
resources to carry out that responsibility through any of the legally enforceable
instruments stated above
To communicate and engage with the governed, to provide information, to
promote dialogue, to engender trust, to allow representation, to establish
systematic feedback mechanisms, to respond to the feedback received, to
explain to the governed the changes made in response to their feedback, to
enable openness, transparency, and accountability, and to resolve conflicts
whenever they arise
To collaborate across levels (local, state or a province, national, regional and
global) and across sectors (public, private, and civil society), to design and
establish a process for such collaborations, to establish alliances, networks and
coalitions, to adopt whole-of-government and whole-of-society approaches,
and to persuade actors across sectors and across levels for joint action
To communicate expectations to the policy implementers, watch and appraise
the evaluation of implementation of policies, and use sanctions when necessary
11 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
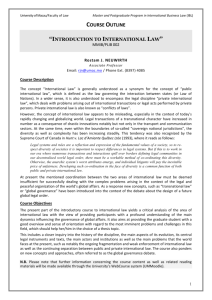
There is strong agreement among these respondents that “Include” and “Steer” are two
prominent governance practices (See Figure 4 below): fully 75% of the respondents stated that
both “Include” and “Steer” are a highly significant parts of the governing process. “Regulate,”
“Collaborate,” “Oversee,” and “Allocate” are also perceived as highly significant elements of the
governing process by 67%, 63%, 60% and 58% of the respondents, respectively. Ninety-two
percent of the respondents indicated that both “include” and “steer” are highly or moderately
significant elements of the governing process, while 89%, 88% 87% and 85% indicated the same
for “collaborate”, “regulate”, “allocate” and “oversee”, respectively.
Figure 4: Defining governing in practical terms (N=404)
100%
6%
5%
90%
80%
17%
8%
8%
21%
26%
8%
9%
is not a part of
governing at all
17%
70%
25%
29%
is a slightly significant
part of governing
60%
50%
40%
75%
is a moderately
significant part of
governing
75%
67%
30%
63%
60%
58%
20%
is a highly significant
part of governing
10%
0%
To include
To steer
To regulate
To collaborate
To oversee
To allocate
Enablers and impediments for effective governance
When queried about 15 potential enablers and impediments to effective governance for health
listed in the survey, the respondents indicated factors they thought enabled or deterred effective
governance, the top ten of which are stated in Table 3. According to the respondents, “governing
with ethical and moral integrity” and “competent leaders governing in the health sector” are the
two most important facilitators. The majority of the respondents saw governing with the enablers
in place leading to both improvements in health services and in health. Figures 5 and 6 in the
Appendix graphically display the survey responses on enablers and impediments for effective
governance.
12 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Table 3: Top ten enablers and deterrents of effective governance
#
1
2
Deterrent
Ineffective leadership
Corruption
3
Ineffective management
4
5
Inadequate transparency
6
Inadequate systems to collect, manage,
analyze and use data
7
8
9
Inadequate accountability
Inadequate participation of community/
citizens/ clients/ consumers/ patients
Political context
Inadequate checks and balances
10 Inadequate financial resources for
governance
#
1
Enabler
Governing in health sector with ethical
and moral integrity
2 Competent leaders governing in health
sector
3 Governing in health sector with a definite
policy on measurement, data gathering,
analysis, and use of information for policy
making
4 Sound management of health sector
5 Adequate financial resources available for
governing in health sector
6 Governing in health sector in open and
transparent manner
7 Governing in health sector with
client/community participation in decision
making process
8 Governing in health sector with
accountability to citizens/clients
9 Governing in health sector based on
scientific evidence
10 Good Governance in sectors other than
health
Linkages between effective governance, improved health services, and improved health of
individuals and the population
The survey sought to understand how the respondents defined effective governance in the
context of health (See Figure 7 in Appendix). Fully 75% of the respondents answered that
effective governance in the context of health is governance that leads to both an improvement in
health services and the health of individuals and populations.
The linkage between effective governance and improved health services
The respondents were further asked to indicate the extent to which effective governance in the
health sector leads to specific health service outcomes (See Figure 8 in Appendix). In order of
importance, the respondents indicated that effective governance leads “to a large extent” to the
following health service outcomes: services become effective (78%); access to and coverage of
the service increase (77%); clients are satisfied (77%); services become efficient (75%); and
services become sustainable (75%). Respondents perceive a very strong link between effective
governance and improvements in quality of health service.
The linkage between effective governance and improved health of individuals and the population
When asked to indicate the extent to which effective governance in the health sector leads to
health gains by individuals and populations, 95% perceived that effective governance has either a
large or moderate effect on health status (See Figure 9 in Appendix).
13 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
The linkage between effective governance in sectors other than health and improved health of
individuals and the population
Respondents also linked the health of individuals and populations to effective governance in
other sectors. Approximately 93% of the respondents stated that effective governance in sectors
other than health leads to a large or moderate extent to better health of individuals and
populations (See Figure 10 in Appendix).
Relationships and interaction between leadership, management, and governance
The perception of the influence of leadership on governance and management is clear.
Leadership is perceived as pre-eminent among the three concepts and influencing the other two.
More than 90% of the respondents agreed or strongly agreed that; 1) leadership influences
governance, 2) leadership influences management, and 3) effective leadership is a pre-requisite
for effective governance (See Figure 11 in Appendix).
Subgroup analysis
A subgroup analysis across gender, sectors (public, private, civil society), levels (local, state,
national and global), country where respondent works (non-OECD vs. OECD), geographical
region (Asia vs. Africa vs. Latin America and Caribbean), those who govern vs. those who
manage but don’t govern, and those who govern vs. those who lead but don’t govern was
performed to see if there are similarities and differences across these subgroups. A detailed
discussion of these can be found in the Appendix. The survey responses clearly had more
similarities than differences on most of the aspects of governing. Minor differences are
nevertheless interesting to note. For example, female respondents were more likely to perceive
‘inclusiveness’ and ‘oversight’ as significant elements of governing. This difference in
perception was statistically significant at 95% confidence level. There were no statistically
significant differences in the way male and female respondents defined hindrances in effective
governance for health, the exception being that women were more likely to identify poor
governance outside the sector of health and the political, historical, and cultural context as
significant impediments to effectively governing for health.
IN-DEPTH INTERVIEWS
Respondent demographics
Self-reported characteristics of the key informants (See Table 4) reveal a predominant
representation from the civil society and public sector. The informants represent 16 countries
form the three regions, i.e., Africa, Asia and Latin America. Africa has the strongest
representation among the informants. This was purposeful and by design. Two in every three of
the informants work at national level, 4% at local level and 12% in an institutional setting. Sixtyeight percent of the informants lead and govern, 20% lead and manage, and 12% lead but neither
govern nor manage. We found that our informants are a highly educated set of people. The
informants are likely to have multiple degrees and from multiple academic disciplines. Seventytwo percent (72%) of the informants have degrees in medicine or medical/surgical specialties,
56% have degrees in public health, 20% in other social sciences, 16% in management, and 16%
in other academic disciplines (one informant each with a degree in science, agriculture, law and
teaching). Medicine and public health combination predominates (44%) and is followed by
14 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
medicine and management (16%). Three respondents had medical degrees alone, and one had a
public health degree alone.
Differences in informant characteristics were noted by region. Overall, women informants
constituted 32% of all the informants. There were more men (7) than women (6) in the
informants from Africa. Women were under-represented in the informants from Latin America
and there were no women respondents from Asia.
Table 4: Participant demographics (n=25)
Characteristic
Gender
Female
Male
Sector
Civil Society
Private Sector
Government
Public Sector/Multi-Sector Governing Bodies
(Country Coordinating Mechanisms or CCMs)
Region
Latin America
Africa
Asia
Countries
Number (%) in each category
8 (32%)
17 (68%)
13 (52%)
1 (4%)
8 (32%)
3 (12%)
7 (28%) (5 Male and 2 Female)
13 (52%) (7 Male and 6 Female)
5 (20%) (5 Male)
Latin America [Bolivia, Colombia, Ecuador,
Guatemala, Mexico, and Nicaragua (2)],
Africa [Kenya (8), Lesotho, Nigeria, Tanzania,
Uganda, and Zanzibar],
Asia [India (2), Lebanon, Oman, and Pakistan]
Language of the interview
English
18 (72%)
Spanish
7 (28%)
Levels where the respondents work
International
4 (16%)
National
17 (68%)
Local
1 (4%)
Institutional
3 (12%)
LMG composition
Those who lead and govern
17 (68%)
Those who lead and manage
5 (20%)
Those who lead
3 (12%)
Note: All categories are mutually exclusive and percentages add up to 100.
15 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
PARTICIPANT EXPERIENCES OF LEADING, GOVERNING AND
MANAGING
What is governance?
Many informants, in many different ways, indicated that governance is a process of making
decisions, and a process of assuring that decisions are implemented. One typical response was,
— “The two key ingredients of governance are, firstly, making a decision for a group of people
and then secondly, finding out whether it worked.” Through making these decisions,
expectations are defined and processes are determined by which an institution is run. Another
ingredient of the definition of governance according to many of the informants was its purpose
which they described as ‘to achieve results’ or ‘to achieve certain goals’ or ‘to accomplish a
vision’. Governance is the exercise of authority and has a political dimension to it. In the
political context, governance is also framed as a democracy issue. A number of informants stated
that governance goes hand-in-hand with leadership. Informants are aware that governance is a
generic term and it takes place in almost all sectors and at all levels — “when we talk about
governance in health, we must remember that we also have governance in agriculture, we have
governance in an environment, and so on.” Governance is done differently in private for-profit,
nonprofit, and public sectors. For example, there may be a collective responsibility to make a
governance decision as in a non-profit hospital board, while in the public sector it may be a
single person who governs; for example, a Minister of Health governs the Ministry of Health, or
it could be a collective body like the Cabinet of Ministers that governs.
Elements or practices of governance
Including the governed in the governing process emerged as a key practice of governing.
Listening to people, involving them in decision making, persuading them, being responsive to
their needs and issues, giving feedback to them, reconciling the different views and the different
positions, bringing together stakeholders/beneficiaries/customers/utilizers of service in the
governing process to achieve results was how the informants typically described this practice of
governing. Making sure that there are systems in place to ensure accountability, transparency and
community participation while governing was the most frequently voiced theme throughout the
interviews.
Collaboration across sectors (public, private for-profit and nonprofit) and ministries (ministry of
health and ministries other than health) and across levels (institutional, local, state, national and
international) was described as a key practice of governing. Several informants cited examples of
inter-sectoral and intra-sectoral collaboration involving several departments and ministries.
These collaborations resulted in successful health interventions and helped achieve the desired
health outcomes. Many respondents voiced the utility of having a forum where such
collaboration could take place on a regular basis. This would enhance the outreach to the
different sectors and levels, and to keep the collaborators interested in a task. This practice was
frequently mentioned in the context of the government or public sector governance.
Steering or policy-making was one of the most frequently voiced practices of governing. Policy
formulation was mentioned as an important element of the governance process. Many
informants stated this practice in terms of setting the big picture, setting up a direction for the
16 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
institution, and making policies in people’s interest based on evidence. Some informants stated
that they are using incentives to steer the health system in the desired direction.
Allocation emerged as one of the significant practices of governance. Smart resource allocation,
referred to by one informant as “distribution with logic” or placing money properly irrespective
of political gain, is perceived to be a part of the governance process. To allocate responsibility of
policy implementation and also authority and resources to carry out that responsibility effectively
was seen by many informants as a significant part of governing process. As with other practices,
the informants focused on the linkage of this practice with the end result. For example, one
informant said, — “prudent application of resources such that at the end we get the desired
results.” Resource mobilization for the organization was also mentioned as one key practice of
governance.
Oversight is another key element of the governance process that is carried out to assure
implementation. The informants clearly perceived the oversight role of the governing body or the
persons is ensuring that the management is doing what it needs to do to deliver the long term
strategy of the institution. Oversight by the leadership and the key actors within the government
health services was perceived as very critical in ensuring good governance principles within the
public health system. Informants felt that rewarding those who perform well and sanctioning
those who do not was part of governing. The need for financial oversight was highlighted by
many of the informants.
Regulation, a majority of the informants felt, was a significant element of governing process. To
formalize policies through laws, rules, regulations, protocols, standard operating procedures, or
resolutions appeared a recurring theme while discussing practices of governance. They saw this
practice as — “setting into motion transparent and credible processes which are difficult to
undermine.” A strong regulatory system based on merit and a strong capability to develop
standards - were both thought to lead to a situation where “politicians would have a lesser
influence.”
See Table 5 in the Appendix for themes and representative quotes on elements/practices of
governing.
Effective governance in the context of health
While defining effective governance in the context of health, the informants were fully aware of
its linkage with the quality of health services and health outcomes. The informants felt that
effective governance in the context of health is the governance that leads to both an improvement
in health service and the health of individuals and populations, and this impact is its defining
feature. “To achieve results” was probably the most common theme heard across all the domains
of this enquiry. Results achieved testify that the governance was effective. Transparency,
accountability and participation and inclusion were the predominant and recurring themes when
the informants discussed effective governance. Ethical and moral integrity, focus and vision, and
efficiency and equity were other important themes that emerged again and again in this context.
Table 6 below and Table 7 in the Appendix state the themes and representative quotes on
effective governance in the context of health. The informants gave many examples of effective
governance and many examples of poor governance from their experience which are described in
Table 8 in the Appendix. Deterrents and enablers of effective governance were broadly similar to
17 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
what we found through our quantitative survey. See Tables 9 and 10 in the Appendix for themes
and representative quotes on deterrents and enablers of effective governance.
Table 6: Effective governance: Predominant themes
Impact on health service and health of people
Transparency
Accountability
Participation
Inclusion
Ethical and Moral Integrity
Focus and Vision
Efficiency and Equity
Linkage between governance and health outcomes
Some informants felt that effective governance is a necessary but not a sufficient condition to
achieve good health for people. However, the majority of the informants expressed that
governance is critical for achieving good health outcomes for individuals and especially for
populations. They hinted at mechanisms through which governance translates into these good
health outcomes. As one informant said, —“we work better because the employees are more
motivated. They love their work and then of course a motivated and a happy worker works
better. The health workers come to work on time, they offer quality care and the patient outcome
is wonderful because these workers are available and that they give their best and the patients get
well.” Another noted, — “when you have poor governance in healthcare, it translates into less of
health promoting, health maintaining and disease prevention interventions within communities
and; when that happens, obviously the diseases that could potentially have been prevented
allowing communities to remain healthier for long, are not being prevented.”
The informants are cognizant of the influence of governance in the sectors other than health
sector on health outcomes. The impact of effective governance on health service and health is
perceived as its defining feature by the majority of the informants. The informants have indicated
that the effect of governance on health is mediated through its impact on health service or health
care in case of governance in health sector and through the social determinants of health in case
of governance in sectors other than health. The informants have described the impact of
governance on health service in terms of enhanced equity and access, effectiveness, efficiency,
affordability, sustainability, and timeliness. On the whole, the informants saw effective
governance as crucial to effective healthcare service delivery. See Table 11 in the Appendix for
themes and representative quotes on the linkage between governance and health outcomes.
Measuring governance
The informants suggested three ways to measure governance — measuring processes of effective
governance, measuring outcomes, and measuring long term impact (See Table 12 below). The
majority was in favor of measuring outcomes. Within the theme of measuring outcomes, there
were two sub themes — measuring attributes of health service, and measuring health outcomes
resulting from effective governance interventions. Many expressed that both the process and
outcomes should be measured. A minority of the informants felt that long term impact is a true
measure of effective governance. The informants substantiated what they said with concrete
examples of the measures (See Table 13 in Appendix).
18 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Table 12: Measuring governance: Themes and sub themes
Themes
Process
Outcomes
Both process and outcomes
Impact
Sub themes
Process
Health service attributes
Health outcomes
Process
Health service attributes
Health outcomes
Health impact
Impact beyond health
An overwhelming majority of the informants asserted that effective governance must be
measured by the result it has been able to produce in terms of improvement in health service and
the health of individuals and populations. A typical comment was, — “I think it is fundamental
to be able to show results.” There was a sole dissenting voice, — “does it [effective governance]
translate into good health? I’m not sure. Somebody has to show me conclusive evidence.”
Another informant underlined the importance of external evaluation of governance. Further, the
informants said that perspective of the measurer is a key in determining measures of governance.
See Table 13 in Appendix for themes and representative quotes on measuring governance.
Gender in governance
We examined the responses of the informants on gender in governance in four domains,
beginning with the gender issues related to women in boardrooms or governing positions, and
then increasingly broadening the scope of domains with gender issues related to women in health
workforce, and finally the issues related women as users of health care. The final domain of our
enquiry was what could be done on the issues surfaced by the informants. We adapted and used
the Rao Gupta (2000), Gupta et al. (2003) and IGWG (Caro 2009) defined gender approaches for
our analysis of the positions taken by the informants or the situations described by them.
1. Blind or gender neutral (gender does not influence how decisions are made)
2. Exploitative (maintains gender inequalities and stereotypes)
3. Accommodating (gender aware and accommodating but they do not seek to challenge the
status quo)
4. Responsive (clearly responsive to different needs based on gender)
5. Transformative (seek to transform gender relations and promote equity as a means of
achieving more sustainable health outcomes)
We received a range of informant responses from essentially gender blind to those seeking
gender transformation in different domains. Overall and on average, across all the domains we
found the perspective of 14 (56%) of our informants gender responsive, the perspective of 4
(16%) of our informants gender transformative, the perspective of 3 (12%) gender
accommodating, the perspective of 2 (8%) gender blind, and the perspective of 2 (8%) gender
exploitative. Those who expressed a gender exploitative perspective said things like — “gender
is culturally oriented. Culture is more important in the context of gender.” or “gender is context
dependent.” They appeared to be tolerant of maintaining gender inequalities or stereotypes if
culture defined them. The informants with gender blind perspective typically said, — “we would
also like competencies to be there as well” or “to me it doesn’t matter which gender one belongs
September 2011 – June 2012
19 L M G P r o j e c t Y e a r 1
to as long as they have the skills, the knowledge and the qualifications to be involved in any
aspect of health delivery.”
The gender responsive perspective was by far the predominant perspective narrated effectively in
the responses. The informants with gender transformative perspective advocated measures like
affirmative action, or special dispensation. The need for gender awareness, gender
responsiveness, and gender transformation in governance was heard from the overwhelming
majority of the informants. See Table 14 in the Appendix for representative quotes.
Inter-relationship and interaction of leadership, management and governance
Three themes clearly emerged from the responses of the 25 informants. First, leadership,
management and governance are interdependent, intricately linked, and reinforce each other. All
three roles interact in a balanced way to serve a purpose or to achieve a desired result. Second,
there is a clear overlap between the roles of leading, managing, and governing. Nevertheless,
each of the roles is relevant. Third, leaders are critical to the governing process. Effective
leadership is a prerequisite for effective governance and effective management. See Table 15 in
the Appendix for representative quotes.
Discussion
To our knowledge, this is one of the few surveys on perceptions and perspectives of the people
who lead, govern and manage in the heath sector and in health institutions in low and middle
income countries on governing and governance. We were able to collect and analyze
perspectives of 500 health leaders, managers and governors primarily from low and middle
income countries. There was a remarkable congruence between the findings of the qualitative
and quantitative components of our survey. We found from the respondents’ perspective,
leadership, management and governance are interdependent, intricately linked, and reinforce
each other. All three roles interact in a balanced way to serve a purpose or to achieve a result.
There is a clear overlap between the roles of leading, managing, and governing. Nevertheless,
each of the roles is relevant. Leaders are critical to the governing process, and effective
leadership is a prerequisite for effective governance and effective management.
Governance to our respondents is a process of making decisions, and a process of assuring that
decisions are implemented. For our respondents, governing has a purpose. Governance has
distinct political and technical dimensions. The respondents identified a clear set of governing
practices. Governing is steering and regulating for a purpose. Governing for our respondents is
raising and allocating resources and allocating responsibility for a purpose. Governing is
oversight. Governing is collaboration across settings and across sectors to achieve a purpose.
Governing, to them, is being inclusive.
Our informants defined effective governance in the context of health as the governance that leads
to both an improvement in health service and the health of individuals and populations. Other
defining features of effective governance our informants perceive are transparency,
accountability, participation, inclusion, ethical and moral integrity, focus and vision, and
efficiency and equity. Our informants have identified what impedes and what enables effective
20 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
governance in the context of health. We heard from them effective governance is a necessary but
not a sufficient condition to achieve good health for people. Nevertheless, it is critical for
achieving good health outcomes for individuals and especially for populations. The informants
are cognizant of the critical influence of governance in the sectors other than health sector, and
the social determinants of health on health outcomes. Our informants have experienced the
impact of governance in health sector on health service through enhanced equity and access,
effectiveness, efficiency, affordability, sustainability, and timeliness of the health service.
The informants suggested three ways to measure governance — measuring processes of effective
governance, measuring outcomes, and measuring long term impact. Measuring outcomes, i.e.
measuring attributes of health service, and measuring health impact resulting from effective
governance interventions was the recurring theme, and was preferred over measuring process
alone.
Our informants largely perceived governance in their settings basically as male dominated and
relegating women’s issues, i.e. issues faced by women in health work force and women as users
of service, to the background. The need for gender awareness, gender responsiveness, and gender
transformation in governance was heard from the overwhelming majority of the informants.
They suggested multiple ways in which gender could be integrated in governance such as
collecting disaggregated data; instituting a gender policy integrating gender perspectives in
health; increasing proportion of women in leadership and governance roles; establishing a
gender-sensitive implementation process that considers different needs of men and women;
establishing quotas and affirmative action coupled with empowerment measures; reinforcing a
safe, harassment free environment by upholding strict codes of conduct and zero tolerance for
discrimination; creating a comprehensive agenda to overcome discrimination and segregation;
and giving voice to all those affected by a policy.
Limitations
Quantitative survey
The low response rate of 8% is a limitation of the survey given that response rates to an internet
survey are typically in the range of 20-30%. The low response rate is partly explained by the fact
that the regularly contributing active membership of our universe of about 6,000 health sector
leaders is quite small. The active membership of the LeaderNet is approximately 10%, and the
Global Exchange Network for Reproductive Health was dormant for about a year prior to this
survey. The low response rate is also mitigated by the finding that 80% of those who responded
completed all of the questions in the survey. There are other limitations to the survey. First,
although the survey resulted in 477 responses from 80 countries and 5 continents, there is
inadequate representation of Asia in the survey responses. Second, the two on-line communities
of practice are supported by MSH and hence their members are familiar with the MSH’s
approach to leadership and management. Because MSH’s work in governance is newer and its
approach is still evolving, the survey responses on governing are unlikely to have been biased by
earlier familiarity with the MSH’s approach on the two constructs of leadership and
management. Finally, the responses are based on perceptions and opinions of practicing health
sector leaders and are not the findings of an experiment.
21 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
In-depth interviews
Our qualitative study has several limitations. Our participants may not be representative of all
those who lead, govern and manage the health sector or the health institutions of low and middle
income countries. With regard to gender, women are grossly under-represented in governing
positions in the international health context, whereas our study with 32% women respondents
may not be representative. Women may have been over-represented in our study. The study had
under-representation from the corporate and public sector, and over-representation form the civil
society sector. In addition, only 16 of about 150 low and middle income countries are
represented in the study. Those who lead, manage, and govern at state and local and institutional
levels are also under-represented.
Overall
The study results are perceptions and opinions and are not findings of a social experiment. The
researchers also had a bias in favor of the power of effective governance to achieve better health
outcomes, which may have influenced survey instruments and interpretation of results. In
addition, we did not explore the political dimension of governing in any substantive way. Our
exploration is largely technical. The study does not at all address the perspective of those who
are governed. These limitations should be considered when weighing the credibility of the
findings, the transferability of the lessons learned, and the scope and focus of future studies.
Policy Implications
This is one of the first studies of its kind in the international health setting and has important
implications for practice and policy in the context of resource-scarce and difficult-to-govern
environments of the low and middle income countries. The study findings have a potential to
inform the governance enhancement interventions in their health systems. Overall, the
governance improvement interventions suggested by the key informants fall within the following
areas: strengthening leadership and management; promoting integrity, measurement,
accountability, openness, transparency, participation, and gender responsiveness; and building
governance capacity.
The study contributes to defining in practical terms governing in the context of health. About
90% of the respondents defined governing in terms of inclusion and collaboration. This finding
tells us that the respondents are aware of the deterrents of effective governance and would
welcome support in these areas. Based on this study, the USAID-funded Leadership,
Management and Governance Project consortium partners have jointly identified practices of
effective governance (described in Table 16) that the project is using in its leadership,
management and governance enhancement work in the health sectors and the health institutions
of the low and middle income countries.
This study finds that the leadership, management and governance are intricately inter-linked and
reinforce each other. Effective leadership is a driver of change. A leadership, management or
governance intervention that considers this interaction and inter-relationship is more likely to be
effective. Leaders are the agents of change, and visionary and ethical leadership is the key in
22 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
enhancing governance. Leaders who govern in low and middle income countries and who wish
to achieve better health outcomes for their constituents should, according to their peers, consider
cultivating integrity, measurement, transparency, participation, accountability, gender
responsiveness, and using technology as they cultivate these attributes in their governing. The
international community in turn should support such leaders who are struggling to make a
difference in governance and through governance in health.
Table 16: Practices of effective governance identified in the USAID-funded Leadership,
Management and Governance Project
Governance practices Principles
Accountability
CULTIVATE
ACCOUNTABILITY Transparency
Legal, ethical
Foster a facilitative
and moral
decision-making
behavior
environment based on Accessibility
systems and structures Social justice
that support
Moral capital
transparency and
Oversight
accountability
Legitimacy
ENGAGE
STAKEHOLDERS
Identify, engage and
collaborate with
diverse stakeholders
representing the full
spectrum of interested
parties
Participation
Representation
Inclusion
Diversity
Gender equity
Conflict
resolution
23 L M G P r o j e c t Y e a r 1
Governing actions
1. Establish, champion, practice and enforce codes of
conduct that uphold the key governance principles
and demonstrate the legitimate authority of the
governance decision-making processes.
2. Embed accountability into the governing institutions
by creating mechanisms for the sharing of
information and by rewarding behaviors that
reinforce the key governance principles.
3. Make all reports on finances, activities, and plans
available to the public, and share them formally with
stakeholders, staff, public monitoring bodies, and the
media.
4. Set an expectation that other stakeholders share
similarly.
5. Establish oversight and review processes (internal
and external monitoring and evaluation by
committees; judicial board) to continuously assess
the impact and appropriateness of decisions made.
6. Establish a formal consultation mechanism (open
forums, special status at meetings, etc.) through
which constituencies may voice concerns or provide
other feedback.
7. Sustain a culture of integrity and openness that
serves the public interest.
1. Empower marginalized voices, including women, by
giving them a place in formal decision-making
structures.
2. Ensure appropriate participation of key stakeholders
through fair voting and decision-making procedures.
3. Create and maintain a safe space for the sharing of
ideas, so that genuine participation across diverse
stakeholder groups is feasible.
4. Provide an independent conflict resolution
mechanism accessible by all stakeholders and
interested parties.
5. Elicit, and respond to, all forms of feedback in a
timely manner.
6. Build coalitions and networks, where feasible and
September 2011 – June 2012
7.
SET SHARED
DIRECTION
Develop a collective
vision of the ‘ideal
state’ and a process
for designing an
action plan, with
measurable goals, for
reaching it
Stakeholder
alignment
Leadership
Management
Advocacy
1.
2.
3.
4.
5.
6.
7.
STEWARD
RESOURCES
Steward resources
responsibly, building
capacity
Financial
Accountability
Development
Social
responsibility
Capacity
building
Country
ownership
Ethics
Resourcefulness
Efficiency
Effectiveness
1.
2.
3.
4.
5.
6.
24 L M G P r o j e c t Y e a r 1
necessary, and strive for consensus on achieving the
shared direction across all levels of governance.
Establish alliances for joint action at whole-ofgovernment and whole-of-society levels.
Oversee the process for developing and
implementing a shared action plan to achieve the
mission and vision of the governed (organization,
community, or country).
Advocate on behalf of stakeholders’ needs and
concerns, as identified through the formal
mechanisms above; making sure to include these in
defining the shared direction.
Document and disseminate the shared vision of the
‘ideal state.’
Oversee the process of setting goals to reach the
‘ideal state.’
Set up accountability mechanisms for achieving
goals that have been set, using defined indicators to
gauge progress toward goal achievement.
Advocate for the ‘ideal state’ in higher levels of
governance, other sectors outside of health, and other
convening venues with a role to play in its
realization.
Oversee the process of realization of the shared goals
and the desired outcomes.
Champion the acquisition and deployment of
resources to accomplish the organization’s mission
and plans.
Protect and invest wisely those resources entrusted in
the governing body to serve stakeholders and
beneficiaries.
Collect, analyze and use information and evidence
for making decisions on the use of resources,
including human, financial and technical resources,
and align resources in the health system and its
design with health system goals.
Determine, and execute, a strategy for building the
health sector’s capacity to absorb resources and
deliver services that are of high quality, appropriate
to the needs of the population, accessible, affordable,
and cost-effective in their consumption of scarce
resources.
Advocate for using resources in a way that
maximizes the health and well-being of the public
and the organization, and invest in communication
that puts health on the policy making agenda.
Inform and allow the public opportunities to monitor
raising, allocation, and use of resources, and
realization of the outcomes.
September 2011 – June 2012
References
Anello E. 2008. Elements of a framework for good governance in the public pharmaceutical
sector. In: A framework for good governance in the pharmaceutical sector. GGM model
framework. Working draft for field testing and revision. Geneva: World Health Organization
Department of Essential Medicines and Pharmaceutical Policies, pp. 19-30. Online at:
http://www.who.int/medicines/areas/policy/goodgovernance/GGMframework09.pdf, accessed 13
June 2012.
Azfar O, Kähkönen S, Meagher P. (2001). The Philippines: Consequences of Corruption. In:
Conditions for Effective Decentralized Governance: A Synthesis of Research Findings. IRIS
Center, University of Maryland, pp. 67-73.
Barr A, Lindelow M, Serneels P. 2009. Corruption in public service delivery: An experimental
analysis. Journal of Economic Behavior & Organization, 72(1), pp. 225-239.
Björkman M, Svensson J. 2009. Power to the People: Evidence from a Randomized Field
Experiment on Community-Based Monitoring in Uganda. The Quarterly Journal of Economics,
124(2), pp. 735-769.
Brinkerhoff DW, Bossert TJ. 2008. Health Governance: Concepts, Experience and Programming
Options. Submitted to the U.S. Agency for International Development. Washington, DC: Health
Systems 20/20.
Caro, D. 2009. The Gender Integration Continuum. In: A Manual for Integrating Gender Into
Reproductive Health and HIV Programs: From Commitment to Action. 2nd edn. Washington,
DC: The Interagency Gender Work Group (IGWG), pp. 9-18. Online at:
http://www.igwg.org/igwg_media/manualintegrgendr09_eng.pdf, accessed 13 June 2012.
Delavallade C. 2006. Corruption and distribution of public spending in developing countries.
Journal of Economics and Finance, 30(2), pp. 222-239.
Gupta GR, Whelan D, Allendorf, K. 2003. Integrating gender into HIV/AIDS programming and
policies. In: Integrating Gender into HIV/AIDS Programmes: A Review Paper. Geneva,
Switzerland: World Health Organization Department of Gender and Women’s Health, pp. 26-41.
Gupta S, Davoodi H, Tiongson E. 2001. Corruption and the provision of healthcare and
education services. In: Jain A (ed). The Political Economy of Corruption. 1st edn. London and
New York: Routeledge, pp. 111-141.
Kickbusch I, Gleicher, D. 2011. Smart governance for health and well-being. In: Governance for
health in the 21st century: a study conducted for the WHO Regional Office for Europe.
Copenhagen: World Health Organisation Regional Office for Europe, pp 43-68.
Lindelow M, Serneels P. 2006. The performance of health workers in Ethiopia: Results from
qualitative research. Social Science & Medicine, 62(9), pp. 2225-2235.
25 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Mikkelsen-Lopez I, Wyss K, De Savigny D. 2011. An approach to addressing governance from a
health system framework perspective. BMC International Health and Human Rights, 11(1), pp.
13.
Olafsdottir A, Reidpath D, Pokhrel S, Allotey P. 2011. Health systems performance in subSaharan Africa: governance, outcome and equity. BMC Public Health, 11(1), pp. 237.
Rajkumar AS, Swaroop V. 2008. Public spending and outcomes: Does governance matter?
Journal of Development Economics, 86(1), pp. 96-111.
Rao Gupta, G. 2000. Approaches for Empowering Women in the HIV/AIDS Pandemic: A
Gender Perspective. Paper presented at the Expert Group Meeting on The HIV/AIDS Pandemic
and Its Gender Implications, November 13–17, 2000. Windhoek, Namibia. New York: United
Nations Division for the Advancement of Women, World Health Organization (WHO), Joint
United Nations Programme on HIV/AIDS (UNAIDS). Online at:
http://www.un.org/womenwatch/daw/csw/hivaids/Gupta.html, accessed 13 June 2012.
Reinhardt UE, Cheng T. 2000. The world health report 2000 - Health systems: improving
performance. Bulletin of the World Health Organization, 78(8), pp. 1064-1064.
Saltman RB, Ferroussier-Davis O. 2000. The concept of stewardship in health policy. Bulletin of
the World Health Organization, 78(6), pp. 732-739.
Siddiqi S, Masud TI, Nishtar S et al. 2009. Framework for assessing governance of the health
system in developing countries: Gateway to good governance. Health Policy, 90(1), pp. 13-25.
Smith PC, Anell A, Busse R et al. 2012. Leadership and governance in seven developed health
systems. Health Policy, 106(1), pp. 37-49.
Strengthening Pharmaceutical Systems (SPS). 2011. Pharmaceuticals and the Public Interest:
The Importance of Good Governance. Submitted to the U.S. Agency for International
Development by the SPS Program. Arlington, VA: Management Sciences for Health, pp. 7-16.
Veillard JHM, Brown AD, Bariş E, Permanand G, Klazinga NS. 2011. Health system
stewardship of National Health Ministries in the WHO European region: Concepts, functions and
assessment framework. Health Policy, 103(2–3), pp. 191-199.
26 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Appendix
FIGURES
27 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Conceptual Model of Governance for Health
Transparency
Accountability
Effective
utilization of
Measurement of
performance
Health Finances
Society
Better
health
outcomes
for the
society
Gender
Responsiveness
Use of
performance data
Human
Resources
Information
Use of evidence
Health Service
Medicines
Cultivate
accountability
Effective
Use of
technology
Effective
Management
Engage
stakeholders
Health
Leaders
Set shared
direction
Equitable
Efficient
Inclusion and
Participation
G
Trust and
Legitimacy
Effective
governance
decisions
Responsive
Sustainable
Steward
resources
Safe
Collaboration
with
Ethical and moral
integrity
Private sector
Effective
Health promotion
Not for profits
CSOs and NGOs
28 L M G P r o j e c t Y e a r 1
Other ministries
that influence
September 2011 – June 2012
health
Disease prevention
Primary
Secondary
Tertiary
Treatment and cure
Figure 1: CONCEPTUAL MODEL OF GOVERNANCE FOR HEALTH
(On the preceding page)
30 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Neglected tropical diseases
Chronic diseases
Clinical and curative medicine
Tuberculosis
Malaria
Nutrition
Child health
Maternal health
Family planning and Reproductive health
83% 81%
HIV/AIDS
Medical products, vaccines and
technologies
Health systems financing
73%
Human resources for health
Health information system
Health service delivery
Leadership and governance
Figure 2: Focus of work of the respondents (n=477)
84%
79% 77%
76%
70%
63%
52%
58% 57%
47% 47%
35%
27%
Figure 3: Whether the respondents govern, observe others govern, manage or
lead
85%
85%
85%
Do you observe
others govern?
Do you manage?
Do you lead?
32%
Do you govern?
31 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Figure 5: Enablers of effective governance and their link to the improvements in
the health service and the health (n=387)
100%
90%
7%
8%
9%
11%
80%
11%
12%
11%
13%
10%
16%
12%
14%
5%
24%
10%
14%
12%
18%
18%
20%
19%
27%
70%
25%
22%
28%
60%
33%
does not lead to
improvement in
a health service
or health
leads to an
improvement in
a health service
50%
40%
83%
81%
77%
76%
74%
74%
70%
69%
30%
58%
58%
56%
54%
42%
20%
10%
32 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Governing in a free media environment
Governing using technology
Governing with checks and balances
Good Governance in sectors other than health
Governing based on scientific evidence
Governing with accountability to citizens/clients
Governing with client/community participation in
decision making
Governing in open and transparent manner
Adequate financial resources available for
governing
Sound management of health sector
Governing with measurement, data collection,
analysis, and use
Competent leaders governing in health sector
Governing with ethical and moral integrity
0%
leads to an
improvement in
health of
individuals and
populations
leads to an
improvement
both in a health
service and
health of
individuals and
populations
33 L M G P r o j e c t Y e a r 1
10%
Inadequate use of technology for governance
20%
Restricted media freedom
50%
Historical, social and cultural context
51%
Policies not based on scientific evidence
60%
Poor governance in sectors other than health
57% 55%
Inadequate financial resources for governance
30%
Inadequate checks and balances
70%
Political context
79%
Inadequate participation of community / citizens
85% 83%
Inadequate systems to collect, manage, analyze and use
data
40%
Inadequate accountability
80%
Inadequate transparency
90%
Ineffective management
100%
Corruption
Ineffective leadership
Figure 6: Deterrents of effective governance (n=387)
3% 4% 3% 5% 4% 5%
7%
8%
12%
11%
12%
does not
11%
13% 14%
16%
22% impede at all
22%
21% 24%
18%
27%
34%
30% 38%
38%
37% 39%
impedes
slightly
40% 41% 45%
73% 70%
67%
is a moderate
impediment
47% 44%
43%
is one of the
32% 31%
29%
top
impediments
0%
September 2011 – June 2012
Figure 7: Defining effective governance in the context of health (n=408)
75%
18%
7%
0%
Governance leading Governance leading Governance leading None of the preceding
to improvements in
to improvement in
to improvement in
both, health service
health of the
health service
and health of the
individuals and the
individuals and the
populations
populations
34 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Figure 8: Perception of the respondents on the linkage of effective governance
in health sector with the quality of health service (n=380)
2%
5%
4%
3%
2%
19%
18%
19%
21%
23%
5%
9%
not at all
22%
29%
slight
78%
77%
77%
75%
75%
72%
moderate
60%
65%
35 L M G P r o j e c t Y e a r 1
Health care becomes safe
Waiting times are reduced
Service becomes more equitable
Service becomes efficient
Service becomes sustainable
Access to and coverage of the
service increase
Clients are satisfied
to a large
extent
Service becomes effective
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
September 2011 – June 2012
Figure 9: Perception of the respondents on the linkage of effective governance
in health sector with health gain by individuals and populations (n=377)
70%
60%
59%
52%
50%
42%
40%
36%36%
36%
a large
moderate
30%
slight
19%
20%
10%
not at all
9%
5%
4%
1%
1%
0%
Better health
36 L M G P r o j e c t Y e a r 1
Client satisfaction
Financial risk
protection
September 2011 – June 2012
Figure 10: Perception of the respondents on the linkage of effective governance
in sectors other than health sector to the better health of individuals and
populations (n=379)
62%
31%
7%
1%
There is no link There is a slight
There is a
There is a large
at all
link
moderate link
link
37 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
73%
30%
69%
64%
38 L M G P r o j e c t Y e a r 1
60%
54%
12%
12%
25%
54%
32%
49%
6%
24%
12%
20%
48%
8%
9%
18%
16%
28%
43%
30%
42%
Effective governance is a prerequisite for effective leadership.
29%
6%
Effective management is a prerequisite for effective leadership.
10%
6%
Management influences leadership.
70%
6%
Effective management is a prerequisite for effective governance.
25%
3%
5%
Management influences governance.
80%
8%
Governance influences leadership.
90%
2%
Effective governance is a prerequisite for effective management.
76%
21%
3%
4%
Governance influences management.
22%
2%
4%
Effective leadership is a prerequisite for effective management.
40%
1%
2%
Effective leadership is a prerequisite for effective governance.
100%
Leadership influences management.
Leadership influences governance.
Figure 11: Perception of the respondents on the interaction of leadership,
management and governance (n=370)
9%
30%
32%
50%
10%
strongly
disagree
18%
disagree
60%
32%
neutral
agree
40%
strongly
agree
0%
September 2011 – June 2012
TABLES
Table 1: Number of respondents, by region and by country in the quantitative survey
Africa
Latin America and
Caribbean
Country
1. Peru
2. Bolivia
3. Haiti
4. Brazil
5. Ecuador
6. Guatemala
#
37
17
15
13
11
11
1.
2.
3.
4.
5.
6.
7.
8.
9.
Asia
Country
Nigeria
Kenya
Ethiopia
Burkina Faso
Rwanda
Ghana
#
43
37
22
11
10
9
Uganda
Côte d'Ivoire
Tanzania,
United
Republic of
10. Democratic
Republic of
the Congo
9
8
8
7.
8.
9.
Mexico
Nicaragua
Dominican
Republic
11
11
6
7
10. El Salvador
5
11. Sudan
6
11. Paraguay
4
12. Botswana
13. Mozambique
4
4
12. Guyana
13. Honduras
14. Niger
4
15. South Africa
16. Namibia
4
3
14. Trinidad
and Tobago
15. Belize
16. Panama
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
3
3
2
2
2
2
2
2
1
1
1.
2.
3.
4.
5.
6.
7.
8.
9.
27.
28.
29.
30.
31.
32.
Total
Senegal
Sierra Leone
Burundi
Cameroon
Egypt
Lesotho
Malawi
Mali
Comoros
Congo,
Republic of
the
Guinea
Madagascar
Morocco
Swaziland
Togo
Seychelles
17. Argentina
18. Colombia
Country
Afghanistan
India
Pakistan
Philippines
Cambodia
Bangladesh
#
13
10
6
5
3
2
Europe, Australia and
North America
Country
1. France
2. Spain
3. Switzerland
4. Albania
5. Armenia
6. Bosnia And
Herzegovina
7. Netherlands
8. Poland
9. Ireland
Fiji
Israel
Japan
1
1
1
1
10. Luxembourg
1
1
11. Australia
1
3
3
10. Korea,
Democratic
People’s
Republic of
11. Micronesia
(Federated
States of)
12. Nepal
13. Singapore
1
1
12. Canada
13. United States
of America
3
14. Thailand
1
2
2
15. Timor-Leste
16. United Arab
Emirates
17. Yemen
1
1
1
1
156
1
50
1
1
1
1
1
1
215
# stands for the number of survey respondents from a country.
39 L M G P r o j e c t Y e a r 1
#
4
2
2
1
1
1
September 2011 – June 2012
1
1
1
2
13
31
Table 5: Elements/Practices of governance
Themes
To include
To
collaborate
To steer
Representative quotes
1. The government has to make sure that people do participate effectively and they
have a space for providing their views in regards to quality of services being
provided and whether they are satisfied with what has been done or whether they
have any proposals for improvement. I think we have to provide such avenues. We
in a way then will be contributing to improvements in the health of our population.
2. Leadership involves the governed.
3. Look at the needs of the people; plan on how to achieve them and define the best
models and ways to achieve the same that is satisfactory both in the eyes of the
leaders and in the eyes of the people.
4. You must listen to what’s happening. You must be willing and able to
accommodate.
5. Ability to persuade
6. to involve more people, persuade more people and train more people
7. governance consists of a set of skills, but most of all, these skills have to do with
the ability to reconcile the different views, the different positions, the different
epistemologies and ideologies that exist in order to deal with a specific issue, and
to be able to lead the resolution of a public issue
8. to explain exactly what happened
9. We bring together and include stakeholders/beneficiaries/customers/utilizers of
service in the process to achieve results.
10. Being responsive to whatever the local needs and issues are
1. we should be able to have a forum where we are able to exchange ideas widely
2. an effective coordination among the key players…if we talk about the health
service…… the players within the health departments, the NGOs, health service
providers, everybody who is taking part
3. outreaching to the different sectors, and to try to keep them interested in a task
4. have inter-sectoral and intra-sectoral collaboration with the involvement of several
departments
5. To say “strong” doesn't mean it should be centralist. I really believe in multiple
service networks where the public and private sectors achieve a mixture, there is no
perfect mixture, but they achieve a balance where even though the Government
must control, the Government must leave way to the private sector in order to
enable it to fulfill its role.
6. I really believe in multiple service networks where the public and private sectors
achieve a mix, there is no perfect mix, but they achieve a balance where the
Government may control, yet the Government must leave a space to the private
sector for it to fulfill its role.
1. bring strategic planning to the institution…..one of their key roles is in setting the
big picture…sort of a direction for the institution
2. They set policies.
3. working with management to set their policy and strategy
4. governance is about being able to organize yourself in such a way that leads in a
particular direction
5. Governance can be defined in terms of policy making which is in people’s interest
but based on fairly good evidence
6. We are counting more on incentives in our contracts to steer the system, to steer
them towards more cost effective care.
7. You have to know where you want to go so you can set a course. Think of what
steps one after another, you have to take to get there. Sometimes you are winning,
at other times you are losing, sometimes it's a win-win, sometimes it is negotiate
40 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
To
regulate
To
allocate
To oversee
and sometimes it is enforce.
1. to set up …….rules that people are supposed to follow
2. you need a fairly good regulating system down the line, not one which is witchhunting but which is capable of detecting fraud and capable of cracking down on it
but most importantly you need to take preemptive measures by setting into motion
transparent and credible processes which are difficult to undermine
3. what we are trying to strengthen our regulation capability to develop standards and
to develop a merit system we regulate....... we have the laws and decrees that
should be implemented regarding patient safety in different domains
4. Governance is really rules by which an institution operates. These rules and
processes help one to be efficient.
1. prudent application of resources, managing resources such that at the end we get
the desired results
2. they approve those plans for what we want to do in the course of a given year and
approve the budgets that go with them and they make sure that the actual resources
that are needed are made available to the level of the health system where you want
these policies to be implemented
1. providing oversight of what it is that the management does to ensure that they are
delivering the best possible results for the institution, for the organization, for the
stakeholders, for the communities we are there to serve, and for the governments
that we partner with
2. provide oversight in terms of where we as an organization want to go, our vision
and mission, policies, strategy, the bigger picture relating to that and then oversight
to management, with regards to how it is that we are doing in terms of achieving or
delivering on that vision and mission. They would have responsibility to oversee
our finances that we are using the finances that are entrusted to us in the way that
we ought to be using them. They would have a responsibility to make sure that as
management we are abiding by whatever policies they set and also the laws of the
respective countries that we operate in
3. the role of the governance is to oversee that management are doing what they need
to do to deliver on their long term strategy for the institution
4. Rewarding those who perform well. If they are not rewarded adequately, then
there could be a possibility that these people also fall back and they behave
differently.
5. monitor the implementation of the decisions taken/monitoring what 16 departments
were doing
6. looking at maternal health, child health, nutrition as broad areas in which lack of
progress has frequently been attributed to … issues that are of direct relevance to
oversight and accountability
7. Elements that are critically needed to implement good governance in health
systems are first and foremost linked to accountability at the grassroots level, then
secondly to oversight capacity.
8. who is monitoring, and who is watching
9. setting up systems in terms of monitoring progress, intermediate outcomes and
impact assessment
10. we have responsibility to oversee our finances so that we are using the finances
that are entrusted to us in the way that we ought to be using them
41 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Table 7: Effective governance
Transparency, Accountability and Participation
1. We can’t have sustainable families if there is no accountability between the family
members and transparency in the relationships. If one member of the family is being left
out on key matters that relate to the family then it doesn’t work well. Similar is the case
with governing.
2. Focus and accountability are critically important. Accountability not only within the
health system but also of the political leadership is important. Transparency would be
important and certainly accountability to constituencies would be very important. So, I
think those two things are extremely important; transparency, and accountability.
Governance in that context is transparency, accountability, evidence based
implementation and being responsive to the community needs.
3. Do things in a way that avoids corruption. Practices where authority and institution are
accountable, efficient, and effective and then in taking decisions it’s a participatory and
transparent process and of course, it’s responsive. For me these are the key elements that
one should look out for when you are talking about good governance.
4. Making sure that we do have the systems in place to ensure accountability, transparency
and community participation in development processes….health services..........making
sure that we do have necessary tools, guidelines and manuals in place to be able to
monitor the processes in line with the governance principles……the other action is joint
review……making sure that we involve all the key actors at all levels of the process from
identification, designing, implementation, monitoring and evaluation….ensuring that all
the key actors do participate.
5. Accountability, transparency, rules, regulations, people’s duties and people’s rights are
all important in this process.
6. An effective governance first, it has to be cost effective, it has to use the resources well, it
has to be accountable. It has to be, as I said, fair and equitable. It has to be transparent.
For me, these aspects are very important and also, it has to really be responsive and it has
to be according to the need of the communities and the people who need that decision.
7. There are three key principles of effective governance. The principle of accountability,
the principle of transparency and the principle of participation. And when we talk about
accountability, accountability on resources that are being used for various interventions in
relation to provision of health services, accountability in terms of making appropriate use
of those resources to deliver what is expected to and then on the issue of transparency we
are talking about sharing of information and making everything known by all the key
actors and the issue of participation, how do we engage the different actors in the
purposes as they relate to provision of health services.
8. It is a governance structure which will allow change to occur, which will allow thoughts
of open and free minds to be put on the table. It’s governance which is facilitating rather
than constraining.
9. Mechanisms and institutions involved allow for accountability, for transparency, for
effectiveness in the delivery of services. For example, if we’re talking about health
services, then effectiveness in the delivery of health services, efficiency, equity and also
allowing citizen’s voice in the process become important.
10. One which gives the beneficiary a voice to participate in decisions and the monitoring of
the services. One which is accountable, one which is transparent, one which is effective,
and efficient.
11. Involves participation in that you’re drawing in all the groups that need to be there.
42 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
12. is connected with the democracy
13. The effective governance is the one that would have a listening structure; that is
participatory; governance that is dynamic in which you’ll be able to include diverse
people, and diverse ideas; governance in which you have room for review; and
governance that is not dictatorial. Governance that would allow representation.
Governance that would enhance management productivity. Governance that listens to the
people.
14. An effective process of governance requires a lot of dialogue, a lot of discussion and
debate.
15. When people participate, when people are involved, well, we know what they want, what
they are looking and searching for and if people are not involved, we simply don’t
know….when people participate in these processes, I believe that there is a high impact
on users’ satisfaction.
16. Need to consider the groups including the women, the youth and the poor, you have to
protect and hear them particularly the poor, weak, youth, and those who are vulnerable.
You must find the ways of taking their issues on board. This is really important.
17. Any governance needs to be participative. You need to get the views of everybody; the
young, the women, the men, the civil society and the government, the communities and
everybody. The decision made – has to be responsive to the needs of the people.
Decision has to be also fair– but it has to be also effective. It has to be transparent so that
you can be questioned about it and you can be asked to respond.
18. Governance is effective when it is transparent especially at higher levels.
Efficiency and equity and overall impact on health
1. Effective governance in the health sector is one that facilitates the delivery of effective
and efficient health services and provides the oversight that’s required to make sure that
health service delivery is as it is intended and is making a difference for the people and
that it’s delivered in the most cost effective way possible and it contributes to a
significant improvement in the quality of services that are rendered.
2. The board was clear on what their role is, what they need to do and they were prepared to
do that.
3. The resources we are responsible for in public institution must bear results and they must
be properly targeted because they are not endless resources.
4. To distribute resources with logic. To place the money in its proper place irrespective of
any political gain.
5. Making people have access to high-quality health services, and services are accessible to
everyone.
6. Where there is transparency, less bureaucracy and less hierarchy and power is in balance
7. Governance is effective when the decisions in the end are useful to people. No
governance can be called effective if it does not leave an impact. Outcomes for people are
important rather than outputs.
Focus and vision
1. Focus and accountability are critically important.
2. To be results oriented and to be focused in terms of targets.
3. They were able to influence things because they kept very proper focus.
Ethical and moral integrity
Governance can be defined in terms of policy making in people’s interest but based on
good evidence. Effective governance is context sensitive, culturally compatible and
43 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
equity promoting. There is a clear lack of corruption. Decisions are made in public
interest with commitment to public good. Of particular importance is focus on equity.
Being ready to be held accountable for policies and programs, being open to evaluation,
providing information as freely as possible in the public domain, to me, that’s good
governance. Efficiency is also important in terms of ensuring that whatever services have
been promised are effectively delivered and delivered at a prudent cost. There has to be a
cost effectiveness consideration and a value for money consideration, all of these
attributes go into good governance. If you can have a tertiary health care which is popular
which yields good results of care, good for some people who require healthcare but then
if you’re diverting the major part of your health budget to that and ignoring primary
healthcare completely, then that’s not good governance. So we’ll have to look at good
governance in many dimensions.
44 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Table 8: Examples of effective governance and poor governance
Examples of effective governance
An informant, who leads, manages and governs from within the government, had a first-hand
experience of using governance strategies for improving the health outcomes in their contracting
with the NGOs —“We tell them, according to the contract, we are not assessing you according to
the quantity of services you are providing in the primary health center. We are not assessing you
according to outputs. We are assessing you according to the improvement of the health status of
the community; in other words, according to outcomes, according to the impact of your
intervention on the health of the community. ”
Yet another informant, leading and governing now for more than two decades within the
government, described the key to the success of their birth spacing program. The key was
participation. The informant described — “The planning was good, the whole-of-the-government
including the Ministry of Finance was involved. Other organizations such as women’s
associations and mass media were very supportive. It was good for the families, the mothers and
the children. The kids got proper attention. Health of the mothers and the children improved. The
total fertility rate was reduced from a pre-program level of 8.4 to a post-program level of 4.”
An informant cited an example of a province while describing how governance mattered for
HIV/AIDs outcome — “Take the example of the State of …….. in this country. In fact the first
HIV/AIDS infection was reported from this state. Prevalence started rising, it reached almost one
per cent which is a concentrated epidemic. Right from the beginning, the state has used
innovative approaches in setting up systems addressing this issue and in using the funds allocated
by the national program to effectively implement the program in the state. They have devised a
system of governance whereby they can spend funds they get from national government very
effectively albeit quickly. They have also developed a governance architecture which has a very
strong representation of not just government but also civil society. Because leadership is
important they put a senior level state official in charge of the program, which you won’t find in
other states. Beginning 1994 and in about eight to nine years this state has shown that they could
level out the infection rate and indeed they were the first in the country to control the epidemic”.
Examples of poor governance
Examples of poorly governing entities were quoted whose governing suffered because of “the
issues of corruption, issues of misuse of power, issues with the non-performance”, or the entity
did not have resources under its authority – resource allocation decisions were made elsewhere.
Corruption by far emerged as one of the top determinant of poor governance. Perhaps an
informant represented many informants when he said — “I feel shame for the actions of others
because I have a feeling that in this country, certain notions, such as, “honesty” have been
changed. An honest person now is considered to be a fool, a fool who does not enrich rapidly
even when possible to do so. In my family, one of the rules is - something that my father taught
me and that I always take with me from my grandparents - that it does not matter that you don't
make a fortune soon but what matters is that you can sleep at night. And for you to sleep at night,
you have to be sure that you did not steal from anybody. And if this money that is being misused,
not to say “steal”, is money that comes from the people, the sin is worse.”
Poor governance to some informants was like drifting or “like losing the compass”. Governing
entities were seen as weak because they lacked the competent leaders who had a capacity to
facilitate participation or for that matter capacity to govern. Poor governance was seen to result
into exodus of the key people and decline in the quality of care provided.
Poor governors failed to take the management to task for allowing wastefulness in the health
45 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
facility, and had no particular sense of targeting of their resources. They were not effective
‘hirers and firers’ of the top managers — “Currently, in the public sector for example, you mess
in one institution, you’re transferred. What happens is the problem is transferred to another
place. Moving them around is poor governance.” Another informant gave a similar example—
“The government does not care and keeps changing health officials like pawns on a chess board
and the programs don’t work”.
46 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Table 9: Deterrents of effective governance
Themes
Inadequate
transparency
Inadequate
participation
Inadequate
accountability
Corruption
Ineffective
leadership
Inadequate
financial
resources for
governance
Representative quotes
1. If you make the system more transparent, engaging in the favoritism or
corruption becomes difficult.
2. The contract with the hospital is signed by the minister, so he may favor
one hospital over another or one NGO over another. So this is where
transparency matters and limits his improper decision– when he knows
that the public sees what he is doing.
If you don’t have buy in from people, then it’s a policy just for yourself.
1. What we have is lack of accountability, a lot of corruption, a lot of
“don’t care” attitude in most of our people entrusted with the
responsibility.
2. Effective governance of the health system within a country is dependent
upon who the whistleblowers are, who are the people who hold the other
people’s feet to the fire? That’s the role of academia, researchers, that’s
the role of media, that’s the role of civil society organizations, and
NGOs.
1. I don’t think there is anything which can be held up as a gold standard of
governance where you can’t even point a finger at those elements. We
have to compare between various shades of governance.
2. It appears that corruption is a major issue. I mean, wherever you go
people talk about how problematic the whole issue of transfers of
personnel is, how problematic the whole issue of procurement of drugs
and the equipment is so I think in terms of health services, I think
corruption is a very big issue though it’s not widely talked about. It’s
only when scandal breaks out the people talk about it but it’s a widely
known fact that the services are riddled with corruption; petty corruption
often but corruption nevertheless.
3. The greatest bane of health in ….(a country)…. is corruption and the
poor governance.
4. Personal and institutional interests prevail over the public good.
1. It is the fact that people who are in leading positions think they have the
absolute truth. They cannot admit that they are wrong and that the idea
that has just been told is much better than theirs.
2. If the chief minister of a province is not focused at the right priority, you
can do whatever you like, my friend, and nothing will change. If a
politician decides that she wants to spend the money building statutes of
elephants then you and I can do whatever we like and nothing is going to
change.
1. The major obstacles are political obstacles and of course financial
constraints.
2. If you want to procure at government level; for example, procurement of
health products, you have to follow the principles as articulated in the
national procurement law and regulations but then it involves a certain
cost, for example, to advertise widely, you have to do the evaluation and
these involve costs and sometimes the limited resources could be a
47 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Lack of
governance
competencies
Ineffective
management
Lack of
vision or
focus
Policies not
based on
scientific
evidence
Data and
information
inadequacy
Political
context
hindrance in observing these transparency principles.
1. Do people fully understand what they are doing when sitting in the
governing council? I went through training for being an effective
director and in that training I realized that many people are called to be
the director of a company and they have no idea what their actual role is
or how much trouble they can get into for being a director and not
knowing what their role is.
2. When someone is placed in the position of one who governs and they are
not adequately prepared for it, something like this happens a lot in our
cases like I’m a medical doctor and so I’ve been put in a position of one
who governs. I’m not trained as an administrator, or in the issues that
have to do with the administration, finances and human resource
management that I’m not adequately trained in to govern in the district or
to be in charge in the district. There is a lot of inadequacy in training.
1. We also had inadequate number of people with necessary skills in
monitoring and evaluation, because when you implement you need to
have a strong system for monitoring and evaluation to be able to track
progress in whatever plan that you need to achieve, but when you don’t
have adequate people in that line, then it becomes a bit challenging.
There is another problem with the decentralized structures at the
grassroots level and as much as we wanted to ensure active engagement
of the community in our programs, we’ve been facing with the challenge
of weak capacity at the local government levels because they don’t have
adequate skills to facilitate many of the key functions that are required to
facilitate the grassroots engagement in national development processes.
2. Capacity is weak at the local government level.
3. A well governed health department should be free of excessive
bureaucracy and hierarchy.
Health is not a political priority.
Look at maternal health, child health, and nutrition as broad areas in which lack
of progress has frequently been attributed to lack of evidence based policy
making.
There is not enough information to effectively govern.
1. The political leadership doesn’t have the maturity to see that this is an
important issue. Health is an issue which has a direct bearing on the lives
of people. That maturity that you will not find in the most of the political
class in some of the poorly governed states and that makes all the
difference.
2. In any case when the minister as a politician intervenes, this is to do a
favor, to break the rules, things like that.
3. The political interference is a major hindrance to our work.
4. This is very important and also, when you are aware that some
48 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Historical,
social and
cultural
context
1.
2.
3.
4.
5.
interventions are very cost effective and then, you have political leader’s
decision to allocate resources to less cost-effective interventions.
We have a culture of not wanting to confront the problem very directly.
It’s always sort of you want to go around the problem.
People want to jump queues, people want to cut corners, and people
don’t want to follow due process.
People don’t want to change.
Decisions have to be based on beliefs and culture to be successfully
implemented.
I believe that another one is jealousy. When we see that one person
emerges and creates something that is worth, those who are below rather
than helping him to go up, or go up all together, instead they pull him
down for him to fall, and a lot of good ideas and good intentions stay put.
Jealousy is a serious issue.
49 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Table 10: Enablers of effective governance
Themes
Openness and
transparency
Representative quotes
1. It could be part of a general or societal decay in values but I think we
need to bring sunlight into the mix. People should be able to know
and see what is happening. The other thing i.e. the right information
has to be helpful to some extent and people are demanding
information and that also comes into play. I think more transparent
we make the process the better it is and as the saying goes, sunlight
is the best disinfectant because the more open you make things the
better they become.
2. We should build systems which are transparent, predictable and
rational and keep them open to public scrutiny and then the chances
of such systems being tampered with will substantially reduce.
3. By making the system more transparent, the margin of maneuver for
the minister becomes tight.
Client/community
1. We believe that participation is a strategic element to achieve the
participation
objectives, especially in health.
2. I think partly it is important to have people engaged in the
governance if not in terms of actual design and participation in the
delivery of programs, at least in terms of monitoring of programs and
having people holding the system accountable is important.
3. The participation is important and we have different committees in
the ministry that have prerogatives, such as accreditation, registration
of drugs and marketing of drugs. These committees include people,
representatives from the Order of Physicians, Order of Pharmacists
and the academia. What facilitates my work is when I include
people, and other stakeholders in the decision making process. This
helps the administration to find solutions to problems and when your
stakeholders are participating in decision making, they comply more
easily to implement whatever you plan or whatever regulations you
make.
Accountability to Elements that are critically needed to implement good governance in health
citizens/clients
systems are first and foremost linked to accountability at the grassroots
level.
Ethical and moral The “honesty” issue is critical because while there is corruption, no system
integrity
can operate well.
Competent
leadership
To know with certainty what you want and to that end, you have to analyze
and review all possibilities and to know where you will really focus or on
what you will focus. Firstly, to be crystal clear in what you want. Secondly,
to have determination, courage, bravery, discipline, consistency to focus and
to work hard on what you want and to be really consistent with that. Thirdly,
to be able to negotiate, to provide inspiration, to move, to line up, to
persuade others, to show them the way and to be sufficiently convincing and
clear for the people to believe in you. This kind of leadership facilitates
effective governance.
50 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Good
Governance in
sectors other than
health
Adequate
financial
resources for
governance
Building
governance
competencies
Sound
management
Vision
Scientific
evidence
Free media
environment
1. The health issues appear everywhere; that is, building a road is a
health issue. … a multi-dimensionality exists in connection with
health, because dealing with the health issue from health (health
ministry alone or health sector alone) is dealing with illness instead
of health.
2. To see that things are interconnected and that health will not solve its
problems per se only in the health sector but that other sectors need
to be involved as they are related
Governance doesn’t come in cheap. It is expensive.
1. Some of them were medical doctors, they hadn’t had any
management training, they hadn’t had any participatory training, we
realized it was not solely our fault, they lacked a skill, so we put
them into training and gave them the skill and thereafter things
started improving.
2. There are those who will distinguish themselves as excellent
managers, yet they are doctors. That’s fine, but on the mainstream,
you won’t find those people. They chose a career and they hardly
shift to learn governance or management skills and we should
respect that but those who distinguish themselves in these skills, they
must carry forward the management and governance of those
institutions.
Most managers at the district level have undergone health systems training,
and it helped. The teamwork is important, as well as the ability to followthrough and to control the manner in which this delegating is done.
You can lose your direction but never the objective.
Decisions have to be evidence based. We need to look at what research is
available, what studies have been done which can aid in the decision making
process.
1. One has to ensure firstly that there is a challenge to any position
which is inappropriate which can be raised in the public domain, not
just the media but also by the general public so that those who
govern know that they are being watched.
2. If you can actually get the people on your side and get the media on
your side to some extent….the role of the media is very important in
governance.
51 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Table 11: Linkage with health system performance and health outcomes
Impact on Health
1. This is very critical particularly in health services because a lapse in governance and
follow up is not simply like a mechanical or an engineering lapse. It has big effects and it
may cost life. So it is very critical and as much as it is one of the sensitive areas. For
those who are working in the medical world, it’s a wakeup call. The health sector
governance should be taken with a level of seriousness that ensures that there is not such
a lapse. Then it will make things work the best for the patients.
2. I would say that governance plays a very significant part in the variation of the
HIV/AIDS prevalence rates across the states. Governance may not be the only factor; it
has a very significant impact on the state of the epidemic in the states.
3. When efficient and effective services were provided, children became healthy and
women did not die during childbirth.
4. Bad governance is at the root of not reaching health goals – there is no accountability, no
transparency and no rights. Good governance is required to reach these goals.
5. In our primary healthcare contracts with NGOs, we have developed this new culture of
accountability; accountability to work for improving the health of the community.
Impact on Health Service
I think effective governance is crucial to effective healthcare service delivery. I’d say, very
definitely it matters and yes, it very definitely makes a difference.
Equity and
1. If there is bad governance and the people are not able to access services
access
or even if they are accessing services, these services are not of expected
quality, then you could easily see whether or not the governance system
is making a difference.
2. I’ve seen services expanded to community level and improvement of the
health facilities.
3. It makes a big difference. If there is effective governance and systems
are in place, people are able to access healthcare cheaply, they are able to
access healthcare without any discrimination, they don’t have to have to
travel 15 to 30 kilometers to get to the nearest dispensary.
Effectiveness Care will be delivered more effectively and more efficiently from a well
governed healthcare delivery entity.
Efficiency
1. Efficient, in the sense that care is delivered in the manner that minimizes
the wastage that so often happens in healthcare service delivery. Efficient
meaning that we use the minimum resources required to be able to
deliver a good quality healthcare service.
2. Less resources being applied in a better way, and in the long term to
achieve better effects on population.
Sustainability Service becomes sustainable.
Timeliness
Its impact is that there is no negligence of patients. The services are provided
much faster. Quick attention is given to the patient.
52 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Table 13: Measuring governance
Process
1. How many times did the board members meet? What sort of issues did they transact at
that time? What sort of difference have they been able to make? What sort of contribution
have they been able to make to the healthcare service? Did the board members actually
take time to go through that sort of thing in advance of coming? How well did they
understand their function?
2. I think the first thing is to look at is if the governance structure has a strategy. A strategy
that has smart and strategic objectives. I think that is really where it should start. Do
they have the discipline to implement and after they implement, to have a look at
outcomes?
3. To measure governance, we need to measure the following: measure people’s
participation: Have people participated in decision-making? Do people know the rules
and regulations? Their awareness. Performance: Have targets been achieved against
indicators? Are there policy units and think tanks involved in the processes of policy and
decision-making? Is there external evaluation of work?
4. You just look back at the three key principles: the accountability, transparency and the
participation. What should be the indicator for each of these key principles and now if
you talk about result based management, we need to create indicators so that we’re able
to track the results that have been achieved in every each of the three areas.
5. When we talk accountability for example in health services, we would like to see at the
end of the day have the resources that have been allocated resulted in the decreased
morbidity and mortality due to various diseases and with particular attention to maternal
mortality and the child mortality; those are key indicators. We will see improvement in
the quality of life of the people, and increase in the life expectancy which can be
measured through information available through census.
6. Again on accountability, we look on a set of issues whether the structures and systems for
accountability are in place. Do we have monitoring and evaluation systems in place and
are operational and effective? Do we have effective systems for financial management?
Do we have effective systems for tracking progress in the implementation of these
various programs we are implementing?
7. On transparency, we need to have indicators that enable us to identify whether there are
systems for information sharing, how information is flowing from lower levels to higher
levels and how is this information being used for planning, in the decision making and
how do we provide feedback to the constituency we serve, to the people we serve? And
then, whether we have systems for participation and how have we engaged stakeholders
and all the key actors in the planning processes, and in other key processes like
monitoring and evaluation, and implementation of programs that we planned.
8. To what extent have we involved the most vulnerable groups, for example as far as health
services are concerned, to what extent have we engaged with people living with
HIV/AIDS, people with disabilities, people suffering from certain chronic illnesses
accessing various services within the health system. These are some of the key indicators
that we need to think of in measuring the impact of good governance practices within our
system.
53 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Health service attributes
1. One way to measure effective governance is through efficiency: higher productivity, and
better application of available resources.
2. First question; if good governance leads to better management of finances; okay yes, it
does. Does it (effective governance) translate into good health? I’m not sure. Somebody
has to show me conclusive evidence.
Health outcomes
1. I think governance should be measured on the impact of the health of the population.
What is it that we have changed? We need to have a baseline where we were before and
then because of that good governance, the health of the population has improved. Let’s
take one example. Maternal health. Maternal mortality is at this rate at the beginning –
before we make the governance decision, but because we have implemented that decision
very well at the end of the period that we said we will change this maternal mortality has
been reduced. Then that has made a difference.
2. When things are governed well, there is an attentive staff, the health is improved, the
community will be able to give an indication of governance of the institution.
Both process and outcomes
Whether or not there is transparency in the health system, whether or not there is
accountability in the health system, whether or not citizens have voice in the system,
whether or not services are efficient and effective, whether or not services are equitable?
Impact on health
1. We measure governance by measuring the quality of health that people have.
2. I believe that it is done through results. I think it is fundamental to be able to show
results. When we talk about health and the lives of the people, the results of governance
are measured by the increased wellbeing of the people.
Impact beyond health
Whether kid finishes his University studies....... That’s one measure, in the long term.
54 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Table 14: Gender in governance
Theme and sub theme
Women in boardrooms and women in governing positions
Gender exploitative comment by a group of
leaders
They are very blunt…the older doctors said we
didn’t realize you (women medical association) had
so many good ideas…we thought you just have tea
parties….that sort of organization.
Gender blind position
1. It is a requirement that there should be gender
representation but the issue comes in if – usually it
is actually the women who are over represented in
our committees. It is a good thing but we would
also like competencies to be there as well.
2. In my view, it is about competence. To me it
doesn’t matter which gender one belongs to as long
as they have the skills, the knowledge and the
qualifications to be involved in any aspect of health
delivery.
Gender accommodating position
Encourage very positively and openly participation
of women but it needs to be merit based because if
it’s not merit based then even those decisions will
be then sub-optimal.
Gender responsive position
1. “All the differences in those peculiarities between
men and women in regards to access to health
services have to be taken into consideration…my
suggestion is to make sure that we ensure
engagement of both women and the vulnerable
groups in the key processes as they relate to
planning for health services…in resource
allocation, we also have to look into the different
needs of the various groups within our population.
Some have specific needs that have to be taken into
consideration and we need to create an environment
to ensure that those needs are well taken care
of….the other issue is to have friendly services for
all the groups when it comes to provision of
services; and we need to ensure confidentiality in
health service delivery.”
2. We are conscious of that. We always have ladies in
our board. In our board of 12, you will find we
have four. If they don’t get elected, we have option
to co-opt. We don’t want a board of all men.
55 L M G P r o j e c t Y e a r 1
What can be done
1. Once women are included
in the processes of
governance, I believe, the
treatment must be equal.
That is, their opinion
should not be invalid
because it comes from a
woman, or from a
homosexual. The value of
an opinion depends on the
ability to present it, to
propose it, to sustain it and
maintain a point of view.
This is what makes an
opinion count.
2. Whatever sex is either
managing or governing or
leading should be given the
same audience, the same
understanding, the same
respect.
3. Consider the affirmative
action of gender.
4. You need to have a gender
policy in any organization,
everything should be
gender sensitive. All the
data we’re collecting
should be gender
disaggregated and we
should monitor that
regularly. The
implementation needs to be
monitored regularly. It
doesn’t happen really
regularly and I should
really make it happen and
we should monitor that we
have included gender in
every area in which we are
working.
September 2011 – June 2012
Gender transformative position
We have no discrimination against women in the
health sector. Women are totally involved in
governance in the MoH. Out of the 16 Departments
in the Ministry, 10 are headed by women.
Need for gender awareness, gender
responsiveness, and gender transformation
1. Some of the boardrooms are full with men. They
don’t even know about some of the issues that need
to improve in the systems and in governance.
2. Most of the times we find that people who are
occupying the chief positions are males. I think
that could be the reason females are not able to
make decisions.
3. The health sector used to be male dominated so
now that the women are coming in and there are
many, there is the challenge of the males accepting
to be governed by the women on their wards for
example in my setting.
4. Most of the time governance positions are held by
men and at the decision making level very few
women are there but also most of the decisions we
make are not gender disaggregated. Women are not
involved in the decision making, men make the
decisions for women and there is a lot of problem in
this but we’re making a little bit of progress
particularly in our continent. It’s moving slowly
but we’ll get there.
Women in health workforce
Gender relations are transforming
1. Conventionally, this place for leadership is usually
constricted for women. So very often we are
looking for more women to be trained and deployed
as medical doctors, as nurses, and midwives, and so
on and so forth. So I am happy that in Africa
women are generally in higher numbers in this
field.
2. We used to have more male physicians than female
so it is adjusting now and we used to have more
female nurses than male and this is also adjusting. It
has to do with the tradition and the history. In the
area of nursing, we have been working to encourage
male nurses because we have a big problem of
shortage of nurses. If you go to the university now
you see more women studying medicine, pharmacy
etc., you see more women than men.
56 L M G P r o j e c t Y e a r 1
1. More women doctors, more
women health
administrators, more
women policy makers and
of course with 33 per cent
reservation in the elected
councils is a good policy.
2. Consider the affirmative
action of gender
3. Create an agenda to
overcome the issues of
discrimination, segregation,
ostracism, experienced not
only by women, but also by
transsexuals.
4. Have a gender policy for
the organization.
September 2011 – June 2012
Women as users of health care
Need for gender awareness, gender
responsiveness, and gender transformation
1. I think women are at a disadvantage in terms of
access to services because they are confined to their
houses and their health always comes secondary,
the health of the man comes as the primary thing in
the family and the woman’s childbearing and child
caring, even general health come as secondary.
2. Women are somewhat neglected in terms of the
access to health services, even in terms of their own
health seeking behavior. That’s again a societal
thing which actually puts a lower premium on
women’s health in the family and also the whole
social milieu doesn’t provide them adequate access
to health services and they do not have sufficient
income at their disposal to also purchase services.
3. Women have such unacceptably high levels of
underweight and anemia and particularly adolescent
girls are being neglected.
4. In a situation like that where governance basically
is a male thing, then women’s issues are likely to
get forgotten and yet, when it comes to healthcare
service utilization, you find that women do have,
because of the obstetric function, the need to utilize
healthcare services a lot more than men do and also
because of their caregiver role, they are the ones
who are likely to be bringing children to for
services, not the men. And when the men are
unwell, they bring the men, too. It is important to
recognize that women are key users of services and
yet women tend to be grossly underrepresented
within governance bodies…...
57 L M G P r o j e c t Y e a r 1
1. It is an issue of giving a
voice to all those affected.
2. Any health policy or
development plan has to
take into consideration the
differences existing within
the society. You know the
society is not
homogeneous. We differ in
culture, geographically,
economically, culturally, so
on and so forth and to be
able to be effective, one has
to take into consideration
these differences.
3. Women are subsequently
discriminated against in
terms of our access in the
healthcare and we need to
alleviate that and we need
to prioritize gender very
effectively when we’re
planning health services.
4. Create an agenda to
overcome these issues, and
have a gender policy for
the organization.
September 2011 – June 2012
Table 15: Inter-relationship and interaction of leadership, management and governance
Themes and sub themes
1. Leadership,
management and
governance are
interdependent,
intricately
linked, and
reinforce each
other.
2. All three roles
interact in a
balanced way to
serve a purpose
or to achieve a
result.
1. There is a clear
overlap between
the roles of
leading,
managing, and
governing.
2. Nevertheless,
each of the roles
is relevant.
Representative quotes
1. It’s a bit like if you think of the African stools ― three-legged
stools; you can’t quite say that this one leg is more important
than the other, because without any of those three legs; it
doesn’t effectively serve the purpose that the stool is meant to
serve. Else think of the three stones that make a three stone
cooking fire.
2. It is like a three-legged stool; you can’t cut one leg and then
say you’re still going to sit and balance.
3. I can’t delink governance from leadership, nor can I delink
management from governance because they are so closely
intertwined that we need to consider to all of them together
and not like in compartments.
4. Leadership, management and governance are three legs of the
same chair; let’s say they are key elements or fundamental
factors in that to the extent that there is good leadership, there
is also good governance. I cannot think of governance
without good leadership.
5. To the extent a good leadership or effective governance exists,
they nourish each other and they grow together. On the
contrary if there is one without the other two, there is entropy.
6. I consider that as a reinforcing relationship. Each one will
enforce each other.
7. We (the Board) don’t take part in day to day decisions but we
question everything they (management) do and then they
(management) report to us. There is the governance to make
sure that they (management) don’t go off on a tangent.
8. Governance is the process that holds all three of them
together.
1. They are related because most of the times, these positions are
held by the same people or by the same person so it’s
important that this person is a leader.
2. Both managers and governors do need to be leaders in their
own individual right, they need to be able to inspire people to
follow them and follow what it is that they want to see done,
what it is that they want to see happen, the sort of things that
they would want to be able to paint a picture of way that a
given healthcare service is going to, a vision that others will
be inspired by and can happily work towards.
3. I think that they are on an equal footing. Interdependence
exists among the three of them. Based on my experience, if
there is governance but no leadership, it doesn’t work. Or the
other way round. Each of the three has its own relevance and
its own responsibility within an organization.
58 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
1. Leaders are
critical to the
governing
process.
2. Effective
leadership is a
prerequisite for
effective
governance and
effective
management.
1. Leadership makes a big difference in governance.
2. There cannot be governance without leadership. Leadership is
an integral part of good governance and good decisionmaking. In any unit or group, even in a family there has to be
leadership. Leadership is the most important.
3. I would say probably leadership is at the top.
4. I think leadership comes first because someone has to carve a
vision and know where they want to go. Then put in place
their policies, guidelines, governance to be able to get there.
5. I think leadership comes first because once you have the right
leadership then you can have great governance systems in
place and once you have the right governance and if you have
the resources then you can have management that works well
for the health sector.
6. The most important thing about governance is leadership.
7. Leadership is most accurately the ability to make a change
when required and where required. It requires the ability to
take people along, to motivate them and use the best of their
talents collectively to bring about that desired change and
therefore good leadership is indispensable for transforming the
health system and a good leadership is integral to good
governance.
59 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
SUBGROUP ANALYSIS
This technical appendix describes the findings of subgroup analyses across gender, sectors
(public, private, civil society), levels (local, state, national and global), country where respondent
works (non-OECD vs. OECD), geographical region (Asia vs. Africa vs. Latin America and
Caribbean), those who govern vs. those who manage but not govern, and those who govern vs.
those who lead but not govern. There are more similarities than differences on most of the
aspects of governing in the survey responses.
Gender
There is no statistically significant difference the way female and male respondents define
governance and effective governance in the context of health. They were asked what governing
means to them in practical terms and to indicate the degree to which they consider to steer, to
regulate, to allocate, to include, to collaborate, and to oversee are a part of the governing process.
The responses of female and male respondents were statistically similar with regard to ‘to steer’
(exact test p-value = 0.8262), to regulate (p-value = 0.9122), to allocate (p-value = 0.2826), to
include (p-value = 0.0697), to collaborate (p-value = 0.3128), and to oversee (p-value = 0.0827),
at 95% confidence level. At 90% confidence level, female respondents were more likely to
perceive to include and to oversee as significant part of governing.
Female and male respondents on average defined effective governance in the context of overall
health as governance that leads to improvement in both a health service, and health of individuals
and populations. There were no statistically significant differences across gender at 95%
confidence level (chisq p value= 0.0723). At 90% confidence level, on average women were
more likely to define effective governance in terms of these improvements.
There were no statistically significant differences in the way men and women defined hindrances
(all p-values >0.05) in effective governance for health except women were more likely to
identify poor governance in sectors other than health (p-value = 0.0146), political context (pvalue = 0.035) and historical and cultural context (p-value = 0.0231) as significant impediments
in governing for health. Speaking of facilitators, there were no statistically significant differences
in the way men and women defined facilitators (all p-values >0.05) in effective governance for
health except women were more likely to perceive good governance in sectors other than health
as one of the facilitators (p-value = 0.054). This finding is consistent with the earlier one
recorded on women more likely to perceive poor governance in sectors other than health as one
of the impediments to effective governing for health.
When asked to indicate the extent to which they considered effective governance in health sector
leads health service outcomes, the female and male respondents gave statistically similar
responses except at 90% confidence level female respondents were more likely to consider
effective governance leading to shorter waiting times (p-value = 0.0607) and equitable health
service (p-value = 0.0978).
60 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
The male respondents were more likely than female to believe in power of governance in health
sector to positively influence health outcomes (p-value < 0.001), financial risk protection (pvalue = 0.0052) and client satisfaction (p-value < 0.001). On the other hand, the female
respondents were more likely than male to believe in power of effective governance in sectors
other than health sector leading to the better health of individuals and populations (p-value =
0.04860). The perceptions of female and male respondents were statistically similar in respect of
interrelationships between leadership, management, and governance.
Sectors
The perceptions on what constitutes governance and what are the elements and practices of
governing are statistically similar across public, private and civil society except the respondents
in public sector and civil society were more likely to perceive ‘to allocate’ as significant part of
governing than the respondents in private sector (p-value = 0.0488).
The respondents in public sector were more likely to cite inadequate information as a constraint
to decision making than those working in civil society or private sector (p-value = 0.0766).
Consistent with this, they were more likely to cite a definite policy on measurement, data
gathering, analysis, and use of information for decision making as an enabler of effective
governance (p-value = 0.0846). Similarly, the respondents in public sector were more likely to
perceive availability of adequate financial resources for governing as an enabler of effective
governance than those working in civil society or private sector (p-value = 0.0405).
Levels
Based on where they work, the respondents working at local level were more likely to perceive
‘to include’ as a significant part of governing than those working at state level who in turn were
more likely to so perceive than those working at national level (p-value = 0.0921). Those
working at national level were more likely to perceive this element of governing as highly
significant, than those working at regional and global levels.
The perceptions and opinions on what impedes and what enables effective governance differed
in a statistically significant manner based on the level at which the respondents worked i.e. local,
state, national, regional or global level. Clearly, the facilitators and deterrents of effective
governance are perceived with varying intensity at different levels. On average, ineffective
management, inadequate accountability, inadequate checks and balances, inadequate
participation, inadequate financial resources for governing, inadequate use of technology were
more likely to be perceived as highly significant deterrents. Similarly, reduced waiting time,
increased client satisfaction, increased service effectiveness, and increased equity were perceived
as highly significant health system outcomes at local level than other levels.
61 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Table: Wilcoxon Scores (Rank Sums) for variables classified by level of work and p-values of
Kruskal-Wallis Test
Variable
Local
State National
Practices of governance
‘To include’ as a practice of governance
210.09 190.02
185.78
Deterrents of effective governance
Incompetent leaders
188.99 195.77
194.82
Ineffective management
198.44 195.5
187.44
Corruption
192.9 200.11
179.42
Inadequate accountability
203.39 174.79
189.06
Inadequate checks and balances
210.23 174.9
169.57
Inadequate participation
203.1
174.5
175.5
Inadequate use of technology in governing
204.36 177.16
174.56
Inadequate financial resources for governing
203.14 188.46
175.63
Political context
198.18 185.09
178.59
Health system outcomes of effective governance
Reduced waiting times
200.5 179.23
176.35
Satisfaction of clients
195.09 188.15
178.1
Service becomes effective
191.1 173.73
183.98
Service becomes efficient
196.34 182.68
174.05
Service becomes equitable
196.68 181.12
182.23
Access and coverage increase
192.59 196.28
182.37
Governance in sectors other than health
Governance in sectors other than health leading to better health 201.34 177.74
174.86
Inter-relationship of leadership, governance, and management
Leadership influences management.
192.33 197.07
168.93
Management influences governance.
189.73 185.96
172.12
Management influences leadership.
197.03 171.65
169.79
Effective leadership is a prerequisite for effective governance.
192.34 195.77
161.73
Effective leadership is a prerequisite for effective management. 186.24 196.82
169.89
Effective governance is pre-requisite for effective management. 187.29 170.34
183.56
Effective governance is a prerequisite for effective leadership.
188.22 181.74
177.82
Regional
Global
p-value
178.62
182.81
0.0921
144.98
135.23
189.83
172.88
166.15
172.39
193.08
185.08
225.65
186.47
168.42
153.33
150.69
152.28
172.25
155.69
151.97
142.47
0.0219
0.0042
0.0717
0.0417
0.002
0.0854
0.0692
0.0964
0.0355
169.42
180.9
177.71
199.79
161.5
149.58
102.24
103.97
130.06
134.09
133.32
105.18
0.0005
0.0002
0.0292
0.0122
0.0214
<.0001
165.1
124.06
0.0034
152.09
127.26
143.52
150.98
148.09
122.86
113.41
134.38
166.53
159.88
158.72
157.94
159.84
196.59
0.0033
0.0412
0.0383
0.0066
0.0894
0.0357
0.0158
At local, state and national levels, respondents were more likely to perceive leadership,
management and governance influencing each other than the respondents at regional and global
levels. Similarly, the respondents at local, state and national levels were more likely to perceive
effective leadership as a prerequisite for effective governance than the respondents at regional
and global levels.
Country where respondent works
The responses were more similar than different based on whether the respondents worked for
OECD countries or Non-OECD countries. There were a few differences of shade in the opinion.
Firstly, the respondents form the non-OECD countries were more likely to report ‘to regulate’
and ‘to oversee’ as practices of governance. Secondly, they were more likely to perceive
corruption as a deterrent of effective governance. Thirdly, they were more likely to see greater
sustainability and higher efficiency as health system outcomes and better health as a health
outcome of effective governance. Finally, they were more likely to perceive leadership
influencing management.
62 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Table: Wilcoxon Scores (Rank Sums) for variables classified by place of work (non-OECD
countries versus OECD countries) and p-values of Exact Test
Variable
‘To regulate’ as a practice of governance
‘To oversee’ as a practice of governance
Corruption as a deterrent
Service becomes sustainable a health system outcome
Service becomes efficient as a health system outcome
Better health as an outcome of effective governance
Leadership influences management.
Non-OECD countries
175.7
170.64
166.55
165.06
164.62
165.67
161.51
OECD countries
124.57
144.4
137.74
135.69
138.86
126.2
141.09
p-value
0.0002
0.0672
0.0055
0.0147
0.0302
0.0035
0.0891
Geographical regions: Asia, Africa, Latin America and Caribbean
The responses were more similar than different depending on whether the respondents lived in
Africa, and Latin America and Caribbean, or Asia. However, the shades of opinion differ in a
few aspects. The respondents in Latin America and Caribbean on average are more likely to
perceive ‘to include’ and ‘to collaborate’ as significant part of governing process than the
respondents in Africa and Asia; whereas the respondents in Africa on average are more likely to
perceive ‘to steer’ as significant part of governing process than the respondents in Latin America
and Caribbean, and Asia.
The respondents in Africa are more likely to believe inadequate transparency and political
context as deterrents to effective governance than the respondents in Latin America and
Caribbean, and Asia. On the other hand, the respondents in Latin America and Caribbean on
average are more likely to perceive ineffective management, corruption, inadequate checks and
balances, inadequate participation, inadequate media freedoms, inadequate use of technology in
governance, inadequate finances for governance, poor governance in sectors other than health,
and historical and cultural context as deterrents to effective governance than the respondents in
Africa and Asia.
Talking of enablers of effective governance, the respondents in Africa are more likely to believe
governing with ethical and moral integrity, governing with openness and transparency, and
governing with checks and balances as enablers of effective governance than the respondents in
Latin America and Caribbean, and Asia. They are also more likely to believe improved safety of
care, reduced waiting times, greater sustainability and increased efficiency of service as health
system outcomes of effective governance. Whereas the respondents in Latin America and
Caribbean on average are more likely to perceive increased equity of service and improved
access and coverage as health system outcomes of effective governance. The respondents in
Africa and Asia are more likely to perceive better health, financial risk protection and client
satisfaction as health outcomes of effective governance.
The respondents in Latin America and Caribbean on average are more likely to perceive
management influencing governance, and management as a prerequisite of governance than the
respondents in Africa and Asia. The respondents in Africa are likelier to believe governance
influencing leadership.
63 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Table: Wilcoxon Scores (Rank Sums) for variables classified by geographical region (Asia,
Africa, and Latin America and Caribbean) and p-values of Kruskal-Wallis Test
Variable
‘To steer’ as a practice of governance
‘To include’ as a practice of governance
‘To collaborate’ as a practice of governance
Ineffective management as a deterrent
Corruption as a deterrent
Inadequate transparency as a deterrent
Inadequate checks and balances as a deterrent
Inadequate participation as a deterrent
Inadequate media freedoms as a deterrent
Inadequate use of technology as a deterrent
Inadequate finances for governance as a deterrent
Poor governance in sectors other than health
Political context
Historical and cultural context
Governing with ethical and moral integrity
Governing with openness and transparency
Governing with checks and balances as an enabler
Improved safety of care as a health system outcome
Reduced waiting times as a health system outcome
Client satisfaction as a health system outcome
Service becomes sustainable a health system outcome
Service becomes efficient as a health system outcome
Service becomes equitable as a health system outcome
Improved access and coverage as a health system outcome
Better health as an outcome of effective governance
Financial risk protection as an outcome of effective governance
Governance influences leadership.
Management influences governance.
Effective management is a prerequisite for effective governance.
Africa
191.07
179.99
176.63
172.67
174.82
178.71
175.27
174.37
171.08
170.66
169.44
171.23
183.08
165.27
178.59
180.67
180.82
178.43
175.61
212.62
179.74
177.03
169.42
167.67
215.97
200.12
178.27
158.4
155.33
LAC
171.6
195.16
199.64
185.02
181.32
175.58
179.34
180.98
192.21
189.76
189.45
191.85
180.88
191.69
175.02
163.71
160.2
167.98
173.52
111.78
165.01
170.78
184.77
180.47
108.59
122.01
155.09
179.82
181.31
Asia
152.28
140.71
145.77
151.73
141.09
142.99
133.26
134.68
117.63
131.21
147.38
126.59
118.19
149.13
145.62
155.04
150.4
148.31
133.94
182.62
157.33
149.5
140.18
148.86
185.93
189.32
154.74
151.53
164.99
p-value
0.0051
0.0006
0.002
0.0292
0.0017
0.031
0.0143
0.0154
<.0001
0.0023
0.0245
0.0005
0.0002
0.0128
0.0138
0.0566
0.0458
0.0915
0.0154
<.0001
0.0929
0.0973
0.0055
0.0344
<.0001
<.0001
0.0505
0.0661
0.0422
Respondents who govern vs. respondents who manage but not govern
Those who said they govern but not manage are more likely to report inadequate transparency as
a deterrent than those who said they manage and not govern. The former are likelier to report
inadequate checks and balances as a deterrent. Consistent with this, they are more likely to report
governing with checks and balances as an enabler of effective governance. The former are also
more likely to report reduced waiting times and client satisfaction as health system outcomes,
management influencing leadership, and effective management as a prerequisite for effective
leadership.
Table: Wilcoxon Scores (Rank Sums) for variables classified by the respondents who govern vs.
respondents who manage but not govern and p-values of Exact Test
Variable
Inadequate transparency as a deterrent
Inadequate checks and balances as a deterrent
Governing with checks and balances as an enabler
Reduced waiting times as a health system outcome
Client satisfaction as a health system outcome
Management influences leadership.
Effective management is a prerequisite for effective leadership.
64 L M G P r o j e c t Y e a r 1
Governors
125.96
127.95
131.37
125.91
124.59
124.53
124.36
Managers
112.4
111
106.37
111.65
111.58
108.25
108.48
p-value
0.0616
0.0375
0.0016
0.0702
0.0994
0.0508
0.0588
September 2011 – June 2012
Respondents who govern vs. respondents who lead but not govern
Those who said they govern but not lead are more likely to report inadequate transparency as a
deterrent than those who said they lead and not govern. The former are likelier to report
inadequate checks and balances as a deterrent. Again consistent with this, they are more likely to
report governing with ethical and moral integrity, competent leaders governing, and sound
management as enablers of effective governance. The former are also more likely to report
reduced client satisfaction as a health system outcome, management influencing leadership, and
effective management and effective as prerequisites for effective leadership.
Table: Wilcoxon Scores (Rank Sums) for variables classified by the respondents who govern vs.
respondents who lead but not govern and p-values of Exact Test
Variable
Inadequate transparency as a deterrent
Inadequate checks and balances as a deterrent
Governing with ethical and moral integrity
Governing with checks and balances as an enabler
Competent leaders governing as an enabler
Sound management as an enabler
Client satisfaction as a health system outcome
Management influences leadership.
Effective governance is a prerequisite for effective leadership.
Effective management is a prerequisite for effective leadership.
65 L M G P r o j e c t Y e a r 1
Governors
129.62
132.51
130.95
136.01
127.99
127.49
131.51
130.51
128.03
128.22
Leaders
116.07
113.25
118.4
107.82
116.29
115.92
112.14
108.61
110.3
110.3
p-value
0.0645
0.0199
0.0566
0.0005
0.065
0.0912
0.0173
0.0099
0.0383
0.0359
September 2011 – June 2012
SURVEY INSTRUMENTS
Quantitative survey
Thank you for your passionate work in public health and a special thank you to those of you who participated in the MSH 2011
survey on Governance for Health. We highly value the work you are doing to strengthen health systems in your jurisdiction.
Management Sciences for Health (MSH) commissioned the Leadership, Management and Governance (LMG) Project on 26
September 2011. At MSH, we have a long history of 25 years of solid work in strengthening leadership and management for
health. Now we are adding a new dimension of ‘governance’ to our existing model of leadership and management, to make the
results of our work sustainable across time and scalable across geographical regions. The results of the MSH 2011 survey on
governance for health have been a useful starting point. We solicit your inputs into the evolving conceptual model of governing
for better health. Your inputs will make the model robust and we will then use it to inform our interventions to save lives and
improve the health of the world’s poorest and most vulnerable people.
We value your insights and experiences and now ask you to help shape the model of ‘governing for health’. We are asking
thought and practice leaders and managers in health sector and also those who govern for health worldwide to participate in a
short, web-based survey about various elements of governing for health.
The questions are focused on various dimensions of governing for health:
■ Practices of governing for health
■ Impediments in effective governance for health
■ Facilitators of effective governance for health
■ Outcomes of effective governance for health
■ Interaction of Leadership, Management and Governance in health
Participation in this survey is completely voluntary. If you decide not to participate there will not be any negative consequences.
Please be aware that if you decide to participate, you may stop participating at any time and you may decide not to answer any
specific question. If you would like to participate, your insights and comments will be confidential and reported in the aggregate.
Your name or any other identifiable information will neither be collected nor be reported or published. There is a minimal risk in
taking this interview. Discussion on governance in general, governance in health sector, and gender in governance is a sensitive
discussion in many local contexts. Issues related to corruption and poor governance may come up in your response which may
not be viewed appropriately by your employer if these become known to the employer. In addition, you will spend 15 minutes in
taking the survey which you could use otherwise.
You may not receive any direct benefit by responding to this survey. If you have any questions about this survey, feel free to
contact Mahesh Shukla, Senior Technical Adviser, Leadership, Management, and Governance Project, Management Sciences for
Health, 4301 N. Fairfax Drive, Suite 400, Arlington, VA 22203 United States (Telephone +1.703.310.3479 direct,
+1.202.386.1164 mobile, fax +1.703.524.7898, email mshukla@msh.org, skype mahesh.shukla8). The survey will take you about
15 minutes. To begin the survey, please continue to the next page.
Thank you again for your work to enhance health gains in nations and communities across the world.
Best Regards,
James A. Rice, Ph.D.
Project Director
Leadership, Management, and Governance Project
Inspired Leadership. Sound Management. Transparent Governance.
Management Sciences for Health
4301 N. Fairfax Drive, Suite 400
Arlington, VA 22203
United States
www.msh.org
jrice@msh.org
Cell: 1 612 703 4687
Skype: jamesrice123
Fax: +1.703.524.7898
66 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
1. Which of the following is focus of your work?
No
Yes
Clinical and curative medicine
HIV/AIDS
Malaria
Tuberculosis
Maternal health
Child health
Nutrition
Family planning and
Reproductive health
Neglected tropical diseases
Chronic diseases
Health service delivery
Human resources for health
Health information system
Medical products, vaccines
and technologies
Health systems financing
Leadership and governance
Other (please specify) _____________________
2. What is your gender?
Female
Male
3. In which sector do you predominantly work?
Public
Private
Civil society
Other
4. At which of the following levels do you work? (check all that apply)
Local
State (or a province)
National
Regional (a group of nations)
Global
Other
67 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Other (please specify) _________________________________________
5. In which country do you live?
Drop-down menu of the countries
6. For which country/countries do you predominantly work?
OECD countries (Australia, Austria, Belgium, Canada, Chile, Czech Republic,
Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Iceland, Ireland,
Israel, Italy, Japan, Korea, Luxembourg, Mexico, Netherlands, New Zealand,
Norway, Poland, Portugal, Slovak Republic, Slovenia, Spain, Sweden, Switzerland,
Turkey, United Kingdom, and United States)
Non-OECD Countries
7. Please check all that apply
No
Yes
Do you govern?
Do you observe others
govern?
Do you manage?
Do you lead?
Defining governance and effective governance in the context of health
8. This question seeks to find out what governing means to you in
practical terms. Indicate the degree to which you consider each of the
following is a part of the governing process?
option is not
relevant
is not a part of
governing at
all
is a slightly
significant part
of governing
is a moderately
significant part
of governing
is a highly
significant part
of governing
To identify a policy problem, to
advocate policy, to set policy
agenda, to have a policy dialogue, to
decide a strategic direction, to
analyze policy options, to make
sound policies, and use continual
learning in refining and adapting
policies for the future ('to steer')
To formalize policies through laws,
regulations, rules of procedure,
protocols, standard operating
procedures, or resolutions, etc. (‘to
regulate’)
To allocate responsibility of policy
implementation and also authority
and resources to carry out that
responsibility through any of the
legally enforceable instruments
stated above (‘to allocate’)
68 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
To communicate and engage with
the governed, to provide
information, to promote dialogue, to
engender trust, to allow
representation, to establish
systematic feedback mechanisms, to
respond to the feedback received, to
explain to the governed the changes
made in response to their feedback,
to enable openness, transparency,
and accountability, and to resolve
conflicts whenever they arise (‘to
include’)
To collaborate across levels (local,
state or a province, national, regional
and global) and across sectors
(public, private, and civil society), to
design and establish a process for
such collaborations, to establish
alliances, networks and coalitions, to
adopt whole-of-government and
whole-of-society approaches, and to
persuade actors across sectors and
across levels for joint action (‘to
collaborate’)
To communicate expectations to the
policy implementers, watch and
appraise the evaluation of
implementation of policies, and use
sanctions when necessary (‘to
oversee’)
Others (please specify any other actions that you feel constitute governing) _______________________
9. Effective governance in the context of overall health is governance that
leads to
improvement in a health service
improvement in health of individuals and populations
improvement in both
none of the above
Impediments to and facilitators of effective governance for
health
10. Which of the following are impediments to effective governance in
health sector?
option is not
relevant
does not
impede at
all
impedes
slightly
is a moderate
impediment
is one of the
top
impediments
Ineffective leadership
Ineffective management
Inadequate systems to collect,
69 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
manage, analyze and use data
Policies not based on scientific
evidence
Corruption
Inadequate transparency
Inadequate accountability
Inadequate checks and balances
Inadequate participation of
community/
citizens/clients/consumers/patients
Restricted media freedom
Inadequate use of technology (for
example, Information and
Communication technology,
eGovernance, etc.) for governance
Inadequate financial resources for
governance
Poor governance in sectors other
than health
Political context
Historical, social and cultural
context
Others (please specify) __________________________________
11. Indicate whether you believe each of the following leads to an
improvement in a health service and health.
does not lead to
improvement in
a health service
or health
leads to an
improvement in
a health service
leads to an
improvement in
health of
individuals and
populations
leads to an
improvement
both in a health
service and
health of
individuals and
populations
Governing in health sector with ethical
and moral integrity
Governing in health sector with a
definite policy on measurement, data
gathering, analysis, and use of
information for policy making
Governing in health sector based on
scientific evidence
Governing in health sector in a free
media environment
Governing in health sector in open and
transparent manner
Governing in health sector with
client/community participation in
decision making process
Governing in health sector with
accountability to citizens/clients
70 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Governing in health sector with checks
and balances
Competent leaders governing in health
sector
Sound management of health sector
Governing in health sector using
technology (for example, Information
and Communication technology,
eGovernance, etc.)
Adequate financial resources available
for governing in health sector
Good Governance in sectors other than
health
Others (please specify) ____________________________
Health outcomes and health gain
12. Indicate the extent to which you consider effective governance in health
sector leads to each of the following health service outcomes.
option is not
relevant
not at all
slight
moderate
to a large
extent
Service becomes safe
Waiting times are reduced
Clients are satisfied
Service becomes sustainable
Service becomes effective (we are able
to achieve what we set out to achieve)
Service becomes efficient
Service becomes more equitable
across gender, age, race, ethnicity,
language, income, education status,
health & disability status, rural/urban,
or geographic regions
Access to and coverage of the service
increase
Other important outcomes (please specify) _________________________
13. Indicate the extent to which you consider effective governance in health
sector leads to the following gain by individuals and populations.
option is not
relevant
not at all
slight
moderate
Better health
Financial risk
protection
Client
satisfaction
71 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
a large
14. Indicate the extent to which you consider effective governance in
sectors other than health sector leads to the better health of individuals
and populations.
not at all
slight
moderate
to a large extent
15. Indicate whether you agree or disagree that each of the following
statements is true.
strongly
disagree
disagree
neutral
agree
Leadership influences governance.
Leadership influences management.
Governance influences management.
Governance influences leadership.
Management influences governance.
Management influences leadership.
Effective leadership is a prerequisite for effective
governance.
Effective leadership is a prerequisite for effective
management.
Effective governance is a prerequisite for effective
management.
Effective governance is a prerequisite for effective
leadership.
Effective management is a prerequisite for effective
governance.
Effective management is a prerequisite for effective
leadership.
72 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
strongly
agree
In-depth interview protocol
Face-to-face interview will be the preference. If face-to-face interviewing is unworkable, then a
phone interview will be organized. Consent for audiotaping of the interview will be sought in
advance while scheduling the interview. Preference will be to audiotape the interview if the
interviewee has consented. The issues of governance are subtle and nuanced. An interviewee is
apt to give much better information and more authentic views if they trust the interviewer and
feel some relationship with them. Trust is the key, and a relationship of trust should be built by
the interviewer.
General probes will be used when the interviewee's response indicates confusion or is not
sufficiently detailed. Following are the examples of some of the general probes those could be
used:
Please tell me more about _____________.
I would like to understand _____________ better. How did __________ work?
You just told me about _________. I also would like to know about __________.
Table A1: Interview protocol
Introduction
(The interviewer to spend some time introducing an interview before launching into asking
questions)
Thank you for agreeing to meet with us. I’m
_____________(name)_________________________ from the _____________[organization]
__________. I also have my colleague _____________
(name)______________________________________ present to take notes for us.
Through this interview, we are trying to capture your thoughts and ideas on governance for
health. What we learn from today’s discussion will help us create a model of governance for
health which in turn will inform our interventions in improving governance for better health
outcomes.
Do you have any questions about the study?
Let us begin.
Q1:
1. Tell me about your background in terms of your work and education.
2. How does it relate to governance in general and governance for health in particular?
We are developing a model of governance to be applied in multiple countries at multiple levels.
Q2:
1. Based on your experience, what does governance mean? How would you define it? What
would you say are its key elements?
2. Think of a person or a body of persons you know who governed. It could be you or some
other persons. What did the person or the body of persons do to govern?
GENERAL PROBE
Can you give an example?
73 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Q3:
1. As you think back over the times you have been involved with the governance or
observed it, what are some things that go wrong? What kind of hurdles have you
experienced or observed in trying to promote effective governance?
2. How were the hurdles overcome?
Q4:
1. Now I am interested in experiences you have had where governance was very effective.
Can you tell me about that?
2. How would you describe effective governance in the health sector?
3. Give an example from real life. Tell me about a well governed health ministry, health
department, or public, non-profit or for profit health institution.
4. What was its impact on health service?
5. What was its impact on health?
Q5:
1. Does effective governance matter in health services? Does it make a difference in a
health service?
2. How?
3. Does effective governance make a difference in health of people?
4. How?
5. How do you suggest we measure governance?
Now we come to the final two topics of our today’s conversation
Q6:
1. What are the gender issues involved in governing for health?
2. How do you deal with these issues? How do you propose those who govern deal with
them?
Q7:
1. How are leadership, governance and management inter-related?
2. Is one important over the other?
3. Does one come before another?
4. What kind of governance will enhance leadership and management?
Conclusion
(A conclusion includes another statement of thanks and reaffirmation of the value of the
responses.)
Those were all of the questions that we wanted to ask. As you know, we are trying to learn more
and develop a model of governance to inform our work. Is there anything I should have asked
you or other information you would like to share that might help us understand these issues
better?
(Answer any questions the respondent may have.)
Thank you for your time.
INFORMATION REQUESTED FROM THE INTERVIEWER (to be filled out after each
74 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
interview)
What was the best quote that came out of the interview?
What was the best story that came out of the interview?
Gender of the respondent: Female/Male
Date of Interview:
75 L M G P r o j e c t Y e a r 1
September 2011 – June 2012
Interview Steps
Step 1: Notify each participant ahead of time that you want to schedule an interview, explaining its main purpose and
importance.
About a week or two before the interview, participants will be notified about the time window and the main purpose of the
interview. A personalized notification e-mail will be sent. This e-mail will be brief and include the following information:
The approximate date when the interview is proposed to be scheduled (e.g., "the third week in January")
The main purpose of the interview
Why it is important for the person to participate (e.g., "your feedback will help us create a model of governance
for health")
The approximate time it will take to complete the interview (e.g., "about 45 minutes of your time")
A statement of thanks
The organization or project sponsoring the interview
It will be made clear that participation in this interview is completely voluntary. If a person/subject decides not to participate
there will not be any negative consequences. It will also be made clear that the subject may stop participating at any time and
may choose not to answer any specific question. There is a minimal risk in taking this interview. Discussion on governance in
general, governance in health sector, and gender in governance is a sensitive discussion in many local contexts. Issues related to
corruption and poor governance may come up in the response of an interviewee which may not be viewed appropriately by the
employer of the interviewee. In addition, the interviewee will spend 45 minutes in taking the interview which he or she could use
otherwise. If the subject decides to participate, his/her permission will be sought for audio taping the interview. An informed
consent form will be given for the interview subject’s perusal and understanding and for his/her conscious decision to sign it.
Step 2: Contact each participant personally to schedule the interview at a convenient time and confirm the interview. Check for
permission about audio taping the interview. Check whether informed consent is administered and received according to the
provisions in the informed consent form. Make sure that the participant understands both benefits and risks of the study and give
at least 24 hours to the participant to make a decision to sign the informed consent form.
The participant will be given at least a week’s notice for scheduling the interview. We will let the participant determine the most
convenient time and place for the interview and whether to allow audio taping. If the interviewee consents for audiotaping, we
shall make all arrangements required for audio taping.
Step 3: Before the interview starts, establish rapport with the participant by engaging in an informal conversation and
demonstrating an interest in the participant's working environment.
Step 4: Introduce the interview, reviewing its purpose and importance, the policies you have established with regard to
confidentiality, and the means by which you intend to record the interview data.
Step 5: With the permission of the participant, audiotape the interview and take brief notes on paper.
Step 6: Follow the interview protocol using a level of judgment; maintain control of the substance and pacing of the interview.
The interviewer will communicate neutrality. Although it might seem tempting at first to compliment the participant for answers,
this runs the risk of implying that we favor his or her views — which, in turn, might lead the participant to make more "socially
desirable" responses that don't necessarily reflect the complexity of his or her thinking. Before the interview begins we may need
to make it clear that we are biased in favor of the power of effective governance for health and the interviewee should not let that
influence what the interviewee says since the purpose of interview is to solicit the range of ideas and thoughts from people such
as the interviewee and not the interviewer.
Step 7: At the conclusion of the interview, thank the participant and collect any supporting materials.
Step 8: Later the same day, verify the quality of the interview data, expand on brief protocol notes, and document any unusual or
other interesting aspects of the interview experience.
Step 9: To consider and compare what participants said in their interviews, interview audiotapes will be transcribed. A typed
interview transcript will serve as a written record of every word spoken and thus will be the most usable and objective form of
the interview data.
*****
76 L M G P r o j e c t Y e a r 1
September 2011 – June 2012