Úvod do bioetiky
advertisement

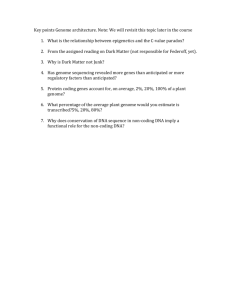
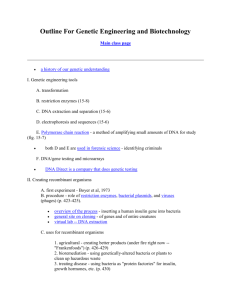
There are more things in heaven and earth, Horatio, than are dreamt of in your philosophy. Hamlet, Act 1, Scene V. Marek Vácha 2014 FOUR YEARS WITH ETHICS II. „TAKE-HOME MESSAGES“ THIRD YEAR 2014 HUMAN GENOME: A BRIEF HISTORY Perhaps you have heard the joke about the guy whose keys fell out of his coat pocket late at night on a darkened street. Realizing later that he was without his keys, he began searching. His companions were surprised to find him searching vainly injust one place – under the streetlight. Asked why he was limiting his search, he explained, „Anyone knows you can´t find your keys where there´s no light.“ Sadly, the candidate gene strategy generally suffered the same fate – and we didn´t find keys. Why couldn´t this be done more systematically? Why couldn´t we light up the whole street? BRIEF HISTORY june 1986, Cold Spring Harbor, symposium on „The Molecular Biology of Homo sapiens“ the idea has been discussed for the first time in front of a large audience, more than 300 of the world´s top human geneticists and molecular biologists Walter Gilbert´s estimate that the project could cost $ 3 billion ($ 1 per base) caused uproar: many of his listeners assumed that funding for biological research would essentially be diverted to this one goal, leaving nothing for the traditional, bottom-up approach to science funding that favoured individual innovation Sulston, J., Ferry, G., (2003) The Common Thread. A Story of Science, Politics, Ethics and the Human Genome. Gorgi Books, London. p. 74 Three Stage Approach Whole-genom shotgun approach Celera Genomics The Ethics of Genome Sequence Publications 2003: this community database (EMBL- bank/GenBank/DDBJ) contains over 40 billion bp of sequence from over 100 000 different organism All three databases implemented a policy that was both courageous and foresighted: to make all of their data freely available to all (whether they be companies, academics or „John Smith“) The Ethics of Genome Sequence Publications By the late 1980s most reputable scientific journals were demanding deposition of sequence data in this database as a precondition for the publication of a scientific paper. This immediately gave rise to a conflict: commercial companies (and some academics) saw their DNA sequence data as a intelectual property that might be turned into money. They were often reluctant to make their data freely available, since this might both compromise patent protection and reduce value of their „property“. Bermuda Agreement 1996 = all data from the Human Genome Project will be deposited in the public sequence databanks each sequencing center will release its own data every day Open access and early release mean that anyone in the worldwide biological community can use those data and turn them into biological understanding and ultimately into new inventions that can be patented. But the sequence itself in its raw form when publicly released becomes unpatentable. Sulston, J., Ferry, G., (2003) The Common Thread. A Story of Science, Politics, Ethics and the Human Genome. Gorgi Books, London Jim Watson „As I saw it, Craig wanted to own the human genome the way Hitler wanted to own the world“ Sulston, J., Ferry, G., (2003) The Common Thread. A Story of Science, Politics, Ethics and the Human Genome. Gorgi Books, London Francis offered apologies all ound – but he then said bluntly that 1999 was going to be a make-or-break year. There was no doubt that Celera would announce that the genome was „complete“ within little more than a year, and that Congress was under real pressure from some quarerrs to shut down the publicly funded genome effort. The only hope was to move fast and in a tightly coorinated way, putting most of the resources available into a small number of big centers. Sulston, J., Ferry, G., (2003) The Common Thread. A Story of Science, Politics, Ethics and the Human Genome. Gorgi Books, London Public Consortium x Celera Genomics Francis Collins Craig Venter Human Genome Project ...has been finished „many times“ Draft (90 %) June 2000 (announced in White House) February 15, 2001 (draft sequence published) Finished (99,3 %) May 2003 (complete sequence announced) October 2004 (complete sequence published) Nature, únor 2001 V davu jsou fotografie Gregora Mendela, Jamese Watsona a Francise Cricka. Science february 2001 BIOLOGY OF THE HUMAN GENOME Human Genome – Internal Universe After many centuries of investigations we have built up an approximate understanding of at least the more accesible parts of our external Universe ...however, there is also a largely unexplored Universe within us about 1011 neurons and somewhere in the region of 1015 interconnections Human Genome DNA sequences that code for proteins or give rise to tRNA or rRNA compose a mere 1,5 % of the human genome there are 78 000 proteins in human body If we include introns and regulatory sequences associated with genes, the total amount of DNA that is gene-related - coding and non-coding - constitutes about 25 % of the human genome put another way, only about 6 % (1,5 % out of 25 %) of the lenght of the average gene is represented in the final gene product 1980: one lab 1000bp a day 2000: one lab 1000bp per second, 24 hours a day, seven days a week first human genome: 13 years and cost $ 3 billion James Watson´s genome: four months (2007) for about $ 1 million 2010: 3 humans, each $ 4 400 2011: one day, $ 1000, cca 1000 persons Craig Venter´s Genome 3 millions SNPs 14 779 changes in protein coding regions (SNPs) 20% never seen before 2020 change in protein sequence (nonsynonymous aminoacid substitutions) 12% predicted to disrupt function of proteins 11% in disease-causing genes There is no "The Human Genome" platonic´s idea of the ideal human genome probably does not agree with reality another marks should be invented for deletions and inzertions 2010: HOMO NEANDERTHALENSIS Sekvenování genomu neandertálce Sekvenování genomu neandertálce http://news.bbc.co.uk/2/hi/science/nature/8660940.stm Between 1% and 4% of the Eurasian human genome seems to come from Neanderthals. Svante Paabo (pictured here with a Neanderthal skull) led the research effort ETHICS James Watson ” We used to think that our fate was in our stars. Now we know, in large part, that our fate is in our genes.“ Zdroj:http://www.cnn.com/video/#/video/us/2007/10/19/todd.saudi.schools.cnn Zdroj:http://www.cnn.com/video/#/video/us/2007/10/19/todd.saudi.schools.cnn A Man: a Periodic Table of Genes? „All matter can be reduced to a periodic table of elements, but at a higher level, every living thing can be reduced to a periodic table of genes.“ (Strachan, T., Read, A.P., (2004) Human Molecular Genetics. 3rd ed. Garland Publishing, New Yourk, p. 208) James Watson: ”We used to think that our fate was in our stars. Now we know, in large part, that our fate is in our genes.“ Walter Gilbert: „When we have the complete sequence of the human genome, we will know what it is to be a human“ E.O.Wilson:Ethics, as we understand it, is an illusion fobbed on us by our genes to get us to cooperate. Robert Weinberg So what are you going to do if you begin to find on a chip of a child's DNA that this kid is likely to be very good in language, probably is going to have poor math skills, will be a rather anxious and obsessive person, will have difficulty associating with his or her peers, and is likely to come down with heart disease at the age of 45? How is that going to affect your relationship to that person, that child? HGP Salvador Luria: “‘Will the Nazi program to eradicate Jewish or otherwise ‘inferior’ genes by mass murder be transformed into a kinder, gentler program to ‘perfect’ human individuals by ‘correcting’ their genomes in conformity perhaps to an ideal ‘white, Judeo-Christian, economically successful’ genotype?“ Ethical Questions knowledge gained from the HGP may lead to the construction of a „standard“ human genome. if this occurs, one must ask what variation society would view as permissible before an individual´s genome was labelled substandart or abnormal? ELSI "All men are created equal" = moral and political equality insurance companies: "you should pay according the risk you bring" more risk - you more have to pay but what about genetic predispositions? genome is not "a bean bag" ... genome is rather an ecosystem RACISM IS DEAD Ethical Issues: Racism is dead 1,5 milions bp – difference between mother and her daughter 2,25 milions bp - difference between grandmother and granddaughter 3 milions bp - difference between two random chosen people on Earth „Race“ is not a biological concept modern population genetics makes the concept of „race“ in the human context biologically meaningless, although socially explosive polish jews are more similar to polish nonjews than to jews in f.e. Spain Humans show little genetic variation compared with other species p p 1.4 0,4 1.2 0,3 0.8 0,2 0.6 0.4 0,1 0.2 Human Chimpanzee Gorilla Human Fish Fly Orang-utan 0 0 Pea* Genetická variabilita (%) 1 Out of Africa and multiregional hypothesis Chimp Genome and Human genome What makes us "human"? Ethical Issues: The Chimpanzee Genome Are there any differences between chimps and humans? The chimpanzee genome is 98.77% identical to the human genome. On average, a typical human protein-coding gene differs from its chimpanzee ortholog by only two amino acid substitutions; nearly one third of human genes have exactly the same protein translation as their chimpanzee orthologs. A major difference between the two genomes is human chromosome 2, which is the product of a fusion between chimpanzee chromosomes 12 and 13. Among the 3 billion base pairs in the DNA of both humans and chimpanzees, researchers found differences in 40 million sites. When measured by changes in their genetic codes, humans and chimpanzees are about 10 times more different than are individual humans from each other. We cannot see in this why we are so different from chimpanzees. Part of the secret is hidden in there /in the genome/, but we don´t understand it yet. Svante Paabo Le Fanu, J., (2009) Why us? How Science Rediscovered the Mystery of Ourselves. Pantheon Books, New York. Skeleton of the Gorilla and Homo Roger Fenton (1819-69), 'Skeleton of Man and of the Male Gorilla (Troglodytes Gorilla)' About 1855 Fenton was the official photographer at the British Museum, which then held collections that are today in the Natural History Museum. Photographed four years before the publication of Darwin’s On the Origin of Species, the ape skeleton has been reconstructed in a more upright form than natural to emphasise the similarities between humans and apes. The gorilla’s left arm shows evidence of a lion bite. Auguste Rodin Woman Centaur (Mind and Body) CREATIONISM IS DEAD How genetically unique are we? 96% with chimpanzee 80% with mouse 50 % with Drosophila 40% with C. elegans 30% with S. cerevisiae Creationism is dead 51% sequences we share with yeasts 57% sequences we share Brassica oleracea 98,6% sequences we share wit Pan troglodytes Creationism is dead Collins, F., (2006) The Language of God. Free Press, New York, p. 128) Convention for the Protection of Human Rights and Dignity of the Human Being with regard to the Application of Biology and Medicine: Convention on Human Rights and Biomedicine OVIEDO, 1997 Chapter IV – Human genome Article 11 – Non-discrimination Any form of discrimination against a person on grounds of his or her genetic heritage is prohibited. The Genetic Information Nondiscrimination Act passed the American Senate in 2003 Act will prevent insurers and employers from discriminating based on genetic information. This means that an insurance company cannot deny you insurance or charge you more because you have a particular genotype, and that an employer cannot fire you or pay you less because you have a particular genotype. FUTURE For centuries, we considered ourselves to be healthy until symptoms of illness arose. Once diagnosed, correctly or not, we received standardized treatments. In accordance with this view, the human body was generally ignored untill something went wrong. Collins, F., (2010) The Language of Life. Profile Books LTD. London, GB. p. 34 We do not have a health care system; we have a sick care system! Collins, F., (2010) The Language of Life. Profile Books LTD. London, GB. p. 58 DNA analysis 23andMe Navigenics deCODE https://www.23andme.com/ http://www.navigenics.com/ http://www.decode.com/ 2010: DNA analysis 23andMe https://www.23andme.com/ $ 399 spitting into special test tube Navigenics http://www.navigenics.com/ $ 2499 spitting into special test tube deCODE http://www.decode.com/ $ 985 scraping cells from a cheek by a swab 2013: DNA analysis 23andMe https://www.23andme.com/ $ 99 spitting into special test tube Navigenics http://www.navigenics.com/ $ spitting into special test tube deCODE http://www.decode.com/ $ scraping cells from a cheek by a swab Your DNA sequence, properly encrypted, will soon become a permanent part of your electronical medical record Collins, F., (2010) The Language of Life. Profile Books LTD. London, GB. ENCODE The Encyclopedia of DNA Elements Project to identify all the functional elements of the genome and to determine how those work together to turn on or off in particular tissues. An additional surprise emerged: for most of the genetic variants that played a role in risk of disease, the problem wasn´t that the glitch led to a garbled protein; rather, the glitch affected whether the responsible gene was turned „off“ or „on“ at the right time and in the right amount. Collins, F., (2010) The Language of Life. Profile Books LTD. London, GB. p. 138 Your DNA sequence, properly encrypted, will soon become a permanent part of your electronical medical record Collins, F., (2010) The Language of Life. Profile Books LTD. London, GB. For centuries, we considered ourselves to be healthy until symptoms of illness arose. Once diagnosed, correctly or not, we received standardized treatments. In accordance with this view, the human body was generally ignored untill something went wrong. Collins, F., (2010) The Language of Life. Profile Books LTD. London, GB. p. 34 USA On May 14, 2008, President Bush signed the legislation /against genetic discrimination in health insurance and in the workplace/. 2013 lincRNA http://www.youtube.com/watch?v=8e9-APttutU Eric Lander cca 100% of the genome transcribed into RNA (non- coding) ...but most in extremly low level, poorly conserved is it biologically functional or biological noise? only cca 15 functional long ncRNAs known XIST, AIR, HOTAIR, H19, TUGI, JPX, KCNQ, PINC, NEAT1, lincP21 there are thousands lincRNA in mammals lincRNAs scaffold regulatory proteins to control cell state can exploit and alter chromosome architecture lincRNA http://www.youtube.com/watch?v=8e9-APttutU are not so conserved like protein-coding genes but are more conserved than background lincRNAs http://www.youtube.com/watch?v=8e9-APttutU make flexible scaffold regulating cell states can exploit and alter chromosome architecture Biology 2.0 Post-Genomic Biology FUTURE the way genes are switched on and off is at least as important, both biologically and medically, as the composition of those genes. The idea that the recipe book would be easy to understand is kind of hubris. View from 2001 Protein-coding genes: 35 000 – 120 000 Regulatory Sequences: less than proteincoding information (promoter + a few enhancers) Non-coding RNAs just a few classical types (rRNA, tRNA, snoRNA + XIST, telomerase, 7SL, H19) Transposons Parasites, junk View from 2013 Protein-coding genes: 21 000 Regulatory Sequences: much MORE than protein-coding information (5:1 ratio) Non-coding RNAs around 7 000 Transposons symbionts (accelerate evolution) evolutionary conserved sequences 6% protein-coding genes 1,2 % most conserved sequences are in the gene- poor regions! most evolutionary inovation concerns non- coding sequences highly conserved elements control early development The Road Ahead Complete catalogs across the wide range of cell types and conditions of all transcripts all long-range genomic modifications all epigenetic modifications all interactions among proteins, DNA and RNA “Whenever man takes a new step towards subduing nature through the art of organisation and technology, he should previously have taken two steps within himself in order to deepen his ethical thinking” (Friedrich von Hardenberg, 18th. century) GEN-ETHICS 2013 Marek Vácha John Sulstone against genetic discrimination "A hundred years ago, there was no equitable treatment for women; they didn't even have the vote. There was no equitable treatment for people of different races. We've established both of those, and now we need to do it across the board for all genetics.„ http://www.guardian.co.uk/science/2004/may/15/genetics.academicexperts GENES H.G.Brunner only males 50 % of males X chromosome Abdelmalek Bayout Abdelmalek Bayout, an Algerian citizen who has lived in Italy since 1993, admitted in 2007 to stabbing and killing Walter Felipe Novoa Perez on 10 March. Perez, a Colombian living in Italy, had, according to Bayout's testimony, insulted him over the kohl eye make-up the Algerian was wearing. Bayout, a Muslim, claims he wore the make-up for religious reasons. During the trial, Bayout's lawyer, Tania Cattarossi, asked the court to take into account that her client may have been mentally ill at the time of the murder. After considering three psychiatric reports, the judge, Paolo Alessio Vernì, partially agreed that Bayout's psychiatric illness was a mitigating factor and sentenced him to 9 years and 2 months in prison — around three years less than Bayout would have received had he been deemed to be of sound mind. Genes „For“ Criminal Behaviour Crime = an act or the comission of activity that is forbidden Criminal behaviour can be a one-time phenomenon can be a profession shoplifting x pickpocketing leaving lethal nerve gas on a subway station shooting a doctor working in an abortion clinic „white collar crime“ = there is not such thing as „a crime“ GENES ...AND RESPONSIBILITY GENES INFLUENCE BEHAVIOUS Artificial selection ENVIRONMENT Environment behaviorism: give me a dozen healthy infants, well-formed, and my own specified world to bring them up in and I´ll guarantee to take anyone at random and train him to become any type of specialist I might select – doctor, lawyer, artist, merchant-chief and, yes, even beggar-man and thief, regardless of his talents, penchants, tendencies, abilities,vocations, and race of his ancestors. Behaviorism A man is nothing but a piece of plasticine... FREEDOM Animisms There is no difference between 1. person and thing 2. living and non-living 3. spiritual and material World of children and world of science Being is being alive Science Animism René Descartes Panmechanismus Francis Crick: The Scientific Search for the Soul Francis Crick : the soul was not discovered... 1470 1994 Replicators and Vehicles Now (the replicators) they swarm in huge colonies, safe inside gigantic lumbering robots, sealed off from the outside world, communicating with it by tortuous indirect routes, manipulating it by remote control. They are in you and me; they created us, body and mind; and their preservation is the ultimate rational for our existence. They have come a long way, those replicators. Now they go by the name of genes, and we are their survival machines. (Richard Dawkins: The Selfish Gene) The genetic engineering is nothing that „revolution of robots“! GENETIC DISORDERS Unique characteristics of genetic disorders Genetic disordres strike families, not only individuals. Knowledge about genetic disease in one family member may have important implications for the health prospects of other family members; the „patient“ may be an entire family rather that just single person in order to counsel one member of a family it may be necessary to have detailed information about several other family members Unique characteristics of genetic disorders Inherited disorders may affect more than one generation. Thus, genetic disease may have serious consequences for people in generations yet unborn there is a strong need for long term storage (over many generations) of information about genetic disease and for the data protection genetic diseases also differ from non-genetic diseases in the sense that it is to an increasing degree becoming possible to predict disease risk in people who today are healthy and even people who are not yet born Genetic counseling nondirectiveness; informed consent; confidentiality DIRECT-TO-CONSUMER DTC Direct To Consumer individuals obtain direct analysis of their genome for prediction of future medical risks, without the involvement of a health provider. Direct To Consumer it is a natural next step, in the same way that pregnancy tests had left the confines of the physician´s office and found their way onto the pharmacy shelves (see the lecture Human Genome Project) 23andMe Navigenics deCODE https://www.23andme.com/ http://www.navigenics.com/ http://www.decode.com/ Direct marketing of genetic tests to the public (DTC) A development with important ethical implications is the marketing of genetic tests directly to the public. Such tests are designed to detect differences in DNA, genes or chromosomes that are not provided as part of a medical consultation. Direct marketing might be seen as a positive step, as individuals take increasing responsibility for their own health and, armed with information about their susceptibility to particular disease conditions, makes lifestyle changes to promote their health Direct marketing of genetic tests to the public ...but there are at least two potential harms: the impact on individuals of misinterpreted or erroneous predictive health information that overstates the role of genetics in causing common diseases, and which might result in delays in proper medical advice being sought, or in expensive and unproven dietary or lifestyle changes the possibility of people performing inappropriate genetic tests on children or other adults without proper consent Direct marketing of genetic tests to the public for complex disorders such as high blood pressure, genetic factors may only account for a few percent of the risk, whereas changing habits in relation to diet, exercise, smoking and antihypertensive drug treatment could reduce the risk of a heart attack by up to 80 %. Questions and problems with DTC the risk factors detectable by DTC tests are modest in their quantitative contribution to disease for most conditions an individual´s risk will bechanged only slightly by the result of the test the testing does not incorporate an assessment of family history DTC tests do not detect the less common but highly significant genetic mutations that carry a high risk for disease BRCA1/2, Huntington´s disease, fragile X syndrome Questions and problems with DTC a substantial fraction of the heritability for most common disease has not been discovered yet. the possibility of laboratory mistakes the company´s interpretation of the DNA test results is not entirely trivial most of the current data about risk prediction from DNA testing are based upon studies done on individuals of northern European background Questions and problems with DTC consumers who are provided risk information should be skeptical of claims about interventions is it really necessary to pay hundreds of dollars for a DNA test to be told that you should eat a balanced diet, engage in regular exercise, and maintain a normal weight? infomations may cause anxiety, and may require to beconsulted with experts AUTOSOMAL DOMINANT INHERINTANCE Huntington´s disease autosomal dominant inheritance Huntington´s Disease ethical issues Informational self – determination •right to know •right to not know Convention on Human Rights and Biomedicine (Oviedo Convention) 1997 Article 12 – Predictive genetic tests Tests which are predictive of genetic diseases or which serve either to identify the subject as a carrier of a gene responsible for a disease or to detect a genetic predisposition or susceptibility to a disease may be performed only for health purposes or for scientific research linked to health purposes, and subject to appropriate genetic counselling. AUTOSOMAL RECESSIVE INHERINTANCE Sickle cell disease Allison found that different African tribes had very different frequencies of the HbS allele. In some tribes, as many as 40 % of the population was heterozygous faor the HbA allele, while in others almost no one carried HbS It was found, that the HbS allele has evolved at least five separate times! (Gilbert, S.F., Epel, D., (2009) Ecological Developmental Biology. Sinauer Associates, Inc. Sunderland, MA. p. 314-315) Sickle cell disease The disease results from an altered hemoglobin, in which the aminoacid valin substitutes for glutamic acid at position 6 in the βglobin chain. Innocence Project STRs short tandem repeats = tandemly repeated units of 2 - 5 base sequences in specific regions of tahe genome. The number of repeats present in these regions is highly variable from person to person (polymorphic) and for one individual, the two alleles of an STR may even differ from each other Innocence Project nonprofit organization dedicataed ato overaturning wrongful convications, uses STR analysis of archived samples from crime scenes ato revisit old cases. As of 2010, more than 250 innocent people had been released from prison as a result of forensic and legal work by this group Innocence Project In 1984, Earl Washington was convicted and sentenced to death for the 1982 rape and murder of Rebecca Williams. His sentence was commuted to life in prison in 1993 due to new doubts about he evidence. In 2000, STR analysis by forensic scientists associated with The Innocence Project showed conclusively that he was innocent Engineering the engineer as well as the engine, we race our train we know not where. Leon Kass 2013 Marek Vácha GENE THERAPY Gene therapy Pills Cell therapies The gene itself becomes the drug Gene therapy somatic cells concerns one single individual germ cells concerns plenty of individuals CURRENT GOVERNMENT POSITIONS Oviedo 1997: CONVENTION ON HUMAN RIGHTS AND BIOMEDICINE Article 13 – Interventions on the human genome An intervention seeking to modify the human genome may only be undertaken for preventive, diagnostic or therapeutic purposes and only if its aim is not to introduce any modification in the genome of any descendants. Some Comments. Ethics there is no fundamental difference between the transplantation of genes into somatic cells and the transplantations of organs Gene therapy Most human disease results from interaction of a born genetic factors with environmental influences. Therapy only modifies the symptoms of disease, thereby giving the body an opportunity to heal itself gene therapy: effective treatment should correct the underlying genetic defect itself and not just a symptoms Gene Therapy is it true that… the natural is good and the unnatural is bad? ...not particularly important for obtaining the credits, but interesting enough GENETIC ENGINEERING Engineering: man nature (metal) Biological engineering: man man History Gene therapy The first approved gene-therapy protocol began on September 14, 1990, in NIH, Maryland CASES Angelina Jolie underwent a preventive double mastectomy http://www.nytimes.com/2013/05/14/opinion/my-medicalchoice.html?hp MY MOTHER fought cancer for almost a decade and died at 56. She held out long enough to meet the first of her grandchildren and to hold them in her arms. But my other children will never have the chance to know her and experience how loving and gracious she was. ¶We often speak of “Mommy’s mommy,” and I find myself trying to explain the illness that took her away from us. They have asked if the same could happen to me. I have always told them not to worry, but the truth is I carry a “faulty” gene, BRCA1, which sharply increases my risk of developing breast cancer and ovarian cancer. ¶My doctors estimated that I had an 87 percent risk of breast cancer and a 50 percent risk of ovarian cancer, although the risk is different in the case of each woman. ¶Only a fraction of breast cancers result from an inherited gene mutation. Those with a defect in BRCA1 have a 65 percent risk of getting it, on average. ¶Once I knew that this was my reality, I decided to be proactive and to minimize the risk as much I could. I made a decision to have a preventive double mastectomy. I started with the breasts, as my risk of breast cancer is higher than my risk of ovarian cancer, and the surgery is more complex. ¶On April 27, I finished the three months of medical procedures that the mastectomies involved. During that time I have been able to keep this private and to carry on with my work. ¶But I am writing about it now because I hope that other women can benefit from my experience. Cancer is still a word that strikes fear into people’s hearts, producing a deep sense of powerlessness. But today it is possible to find out through a blood test whether you are highly susceptible to breast and ovarian cancer, and then take action. ¶My own process began on Feb. 2 with a procedure known as a “nipple delay,” which rules out disease in the breast ducts behind the nipple and draws extra blood flow to the area. This causes some pain and a lot of bruising, but it increases the chance of saving the nipple. ¶Two weeks later I had the major surgery, where the breast tissue is removed and temporary fillers are put in place. The operation can take eight hours. You wake up with drain tubes and expanders in your breasts. It does feel like a scene out of a science-fiction film. But days after surgery you can be back to a normal life. ¶Nine weeks later, the final surgery is completed with the reconstruction of the breasts with an implant. There have been many advances in this procedure in the last few years, and the results can be beautiful. http://www.nytimes.com/2013/05/14/opinion/my-medicalchoice.html?hp ¶I wanted to write this to tell other women that the decision to have a mastectomy was not easy. But it is one I am very happy that I made. My chances of developing breast cancer have dropped from 87 percent to under 5 percent. I can tell my children that they don’t need to fear they will lose me to breast cancer. ¶It is reassuring that they see nothing that makes them uncomfortable. They can see my small scars and that’s it. Everything else is just Mommy, the same as she always was. And they know that I love them and will do anything to be with them as long as I can. On a personal note, I do not feel any less of a woman. I feel empowered that I made a strong choice that in no way diminishes my femininity. ¶I am fortunate to have a partner, Brad Pitt, who is so loving and supportive. So to anyone who has a wife or girlfriend going through this, know that you are a very important part of the transition. Brad was at the Pink Lotus Breast Center, where I was treated, for every minute of the surgeries. We managed to find moments to laugh together. We knew this was the right thing to do for our family and that it would bring us closer. And it has. ¶For any woman reading this, I hope it helps you to know you have options. I want to encourage every woman, especially if you have a family history of breast or ovarian cancer, to seek out the information and medical experts who can help you through this aspect of your life, and to make your own informed choices. ¶I acknowledge that there are many wonderful holistic doctors working on alternatives to surgery. My own regimen will be posted in due course on the Web site of the Pink Lotus Breast Center. I hope that this will be helpful to other women. ¶Breast cancer alone kills some 458,000 people each year, according to the World Health Organization, mainly in low- and middle-income countries. It has got to be a priority to ensure that more women can access gene testing and lifesaving preventive treatment, whatever their means and background, wherever they live. The cost of testing for BRCA1 and BRCA2, at more than $3,000 in the United States, remains an obstacle for many women. ¶I choose not to keep my story private because there are many women who do not know that they might be living under the shadow of cancer. It is my hope that they, too, will be able to get gene tested, and that if they have a high risk they, too, will know that they have strong options. ¶Life comes with many challenges. The ones that should not scare us are the ones we can take on and take control of. ¶Angelina Jolie is an actress and director. „The Bubble Boy“ David Phillip Vetter (September 21, 1971 – February 22, 1984) he suffered SCID at the age of 12, he died after hematopoietic stem cell transplantation „The Bubble Boy“ What was wrong? pros cons effort to save the life career of the researchers doing everything is publications possible popularity for the researches giving too much hope to the parents Celý životopis JG sepsaný jeho otcem Paulem Gelsingerem je na http://www.jesse-gelsinger.com/ Jesse Gelsinger Treatment for JG: low- protein diet and cca 32 pills per day the day he turned eighteen he left to Pennsylvania and gave the informed consent with the gene therapy Jesse Gelsinger he was pronounced dead on September 17, 1999 His death was the first reported death ever directly attributable to a gene therapy experiment There were questions about the quality of informed consent at University of Pennsylvania and accusations that the university had failed to report toxic side effects earlier that could have shut down the study. ETHICS Gene Therapy Arguments for Gene Therapy Arguments FOR Isolating a disease-inducing aberrant gene looks fairly continuous with isolating a disease-inducing intracellular virus Suppllying diabetics with normal genes for producing insulin has the same medical goal as supplying them with insulin for injection Gene Therapy of Germ Cells Arguments FOR it solves the problem once and for all. Why leave the patient´s descendants at risk of a disease if you could equally well eliminate the risk? Gene Therapy Arguments against Germ cells gene therapy objections present men have the power over the future men, who are the defenseless objects of antecedent choices by the planners of today there is no right to existence for hypothetical individuals not yet conceived but though not the right of merely imagined offspring, the right to offspring of the hindered progenitor is involved. Germ cells gene therapy objections it could lead to people being viewed as products capable of being manufactured, with the result that people could be „made to measure“. our actions might come to be viewed as genetically determined rather than a matter of free will Germ-line Therapy Objections it is not safe when altered genes are inserted into the genome, they may disrupt presently functional genes this has certainly been encountered in laboratory mice. In one case, the disruption of single gene resulted in mice who were born without eyes, semicircular ear canals, or a sense of smell some effects may take several generations to manifeste themselves - and any mistakes made will be permanent (Gilbert, S.C., Tyler, A.L., Zackin, E.J., (2005) Bioethics and the New Embryology. Sinauer Associates, Inc. W.H. Freeman & comp. Sunderland, MA U.S.A. p. 202) Enhancement Nontherapeutical gene modifications Genetic Enhancement Beacause memory is good, can we say how much more memory would be better? If sexual desire is good, how much more will be better? Life is good, but how much extension of the lifespan would be good for us? Only simplistic thinkers believe they can easily answer such question Kass, R.L., (2002) Life, Liberty and the Defense of Dignity. Encounter Books, New York, London. p. 132 Nontherapeutic genetic modification ethical issues Issue of eugenic - are we allowed to make hereditary „improvements“? Slippery slope - might we slide into a new age of eugenic thinking by starting with small genetic improvements? Nontherapeutic genetic modification ethical issues since more and more scientists believe that all traits of personality have at least a partial biological basis, how will we distinguish the biological "defect" that yields "disease" from the biological condition that yields shyness or melancholy or irascibility? Runners Nontherapeutic genetic modification ethical issues researches have produced smart mice by inserting extra copies of a memory-related gene into mouse embryo. The altered mice learn more quickly and remeber things longer than normal mice. The extra copies were programmed to remain active even in old age, and the improvement was passed on to offspring. .. we are now looking for "a Viagra for the brain" Gen-ethics and Synt-ethics 2014 Marek Vácha Green generation Taiwan: DNA from jellyfish was added to about 265 pig embryos which were implanted in eight different sows. Four of the female pigs became pregnant and three male piglets were born The pigs are transgenic, created by adding genetic material from jellyfish into a normal pig embryo. Green generation They are the only ones that are green from the inside out. Even their heart and internal organs are green It remains to be seen, whether from the ethical point of view… ….everything is ok? ANDi ANDi a transgenic rhesus monkey has been born that carries the gene for green fluorescent protein (GFP) in each cell of his body the gene for GFP was inserted into a viral vector that was injected into the space between the oocyte and the zona pellucida in a rhesus monkey egg. The vector inserted the GFP gene into the egg DNA, and the resulting offspring, a monkey called ANDi (=inserted DNA) has GFP genes in all of his cells (Gilbert, S.C., Tyler, A.L., Zackin, E.J., (2005) Bioethics and the New Embryology. Sinauer Associates, Inc. W.H. Freeman & comp. Sunderland, MA U.S.A. p. 196) Frankenfish Frankenfish The GM Atlantic salmon grows twice as fast as its wild cousin. Its genes have been artificially augmented with DNA taken from two other fish – the Pacific Chinook salmon and an eel-like species called an ocean pout (Zoarces americanus) – in order to boost the growth hormone that allows it continually to put on weight throughout the year. http://www.independent.co.uk/news/science/a-giant-leap-into-the-unknown-gm-salmon-that-grows-andgrows-2085856.html The Enviropig A genetically engineered pig recently approved for limited production in Canada makes urine and feces that contain up to 65 percent less phosphorous, officials have announced. Fluorescent mice GloFish In 2007, South Korean scientists altered a cat’s DNA to make it glow in the dark and then took that DNA and cloned other cats from it — creating a set of fluffy, fluorescent felines. Here’s how they did it: The researchers took skin cells from Turkish Angora female cats and used a virus to insert genetic instructions for making red fluorescent protein. Then they put the gene-altered nuclei into the eggs for cloning, and the cloned embryos were implanted back into the donor cats — making the cats the surrogate mothers for their own clones. Scientists at the University of Washington are engineering poplar trees that can clean up contamination sites by absorbing groundwater pollutants through their roots. The plants then break the pollutants down into harmless byproducts that are incorporated into their roots, stems and leaves or released into the air. In laboratory tests, the transgenic plants are able to remove as much as 91 percent of trichloroethylene — the most common groundwater contaminant at U.S. Superfund sites — out of a liquid solution. Regular poplar plants removed just 3 percent of the contaminant. SYNT-ETHICS On May 21, 2010, Science reported that the Venter group had successfully synthesized the genome of the bacterium Mycoplasma mycoides from a computer record, and transplanted the synthesized genome into the existing cell of a´Mycoplasma capricolum bacterium that had had its DNA removed. The "synthetic" bacterium was viable, i.e.capable of replicating billions of times. Artificial life Mycoplasma mycoides 1,08 Mb „synthetic cell“ – only its genome is truly synthetic Synthia Craig Venter: "the first species.... to have its parents be a computer" James Joyce: "To live to err, to fall, to triumph, to recreate life out of life" Robert Oppenheimer: "See things not as they are, but as they might be". Richard Feynman: "What I cannot build, I cannotunderstand" Artificial life critics the potential benefits of synthetic organisms have been overstated. By releasing these „synthetic organisms“ into areas of pollution, we may actually releasing a new kind of pollution. We don't know how these organisms will behave in the environment. Artificial life in the near future we may switch from „reading“ the genomes to „writing“ them the time of „digitizing biology“ is about to come the software builds its own hardware Biomedical Research Bioterrorism Bioerrorism "superweed" etc. Bioerrorism strains of microorganisms to be used in recombinant DNA experiments are genetically crippled to ensure that they cannots survive outside the laboratory. Biomedical research Precautionary Principle When in doubt, pause (mostly Europe) Proactionary Principle When in doubt, go ahead (Thomas Murray, http://www.youtube.com/watch?v=1y4jt7oDrZI) Biomedical research Precautionary Principle When in doubt, pause (mostly Europe) Proactionary Principle When in doubt, go ahead (Thomas Murray, http://www.youtube.com/watch?v=1y4jt7oDrZI) The Presidential Comission for the Study of Bioethical Isues: New Directions: The Ethics of Synthetic Biology and Emerging Technologies (16/12/2010) "prudent vigilance" "the field of synthetic biology does not require new regulations" New Directions: The Ethics of Synthetic Biology and Emerging Technologies 8 FEB 2012 public beneficence responsible stewardship intellectual freedom democratic deliberation justice and fairness 2014 Marek Vácha EUTHANASIA Euthanasia „Dutch definition of euthanasia“ =the intentional termination of the life of a patient at his request by someone other than the patient Euthanasia active active deen on active request nonvoluntary euthanasia pacient is not capable of articulating her wishes involuntary euthanasia which ignores the individual´s autonomous rights and could potentially bring about the death of unwilling victim, is not easily distinguished from murder. (Edge, R.S., Groves, J.R. (2006) Ethics of Health Care. A Guide for Clinical Practice 3rd. ed.Thomson Delma learning, NY. p. 235) passive „doing nothing“ passive voluntary doing nothing with the intention of the death of the patient (sometimes it is hard to distinguishes it from active euthanasia) Assistence in Suicide Assistance in suicide means knowingly and intentionally providing a person with the knowledge or means or both required to commit suicide, including counseling about lethal doses of drugs, prescribing such lethal doses or supplying the drugs Letting die = enabling nature to take its course but there is a difference between: withdrawing machines and medications from the patient withholding or withdrawing artificial nutrition and hydration Reasons for opening the discussion Formerly active life Now active life diaseases and dying death disease and dying death Because of medicine we have today a little bit longer the active life, but proportionally much longer the time of diseases, staying in the hospitals and dying Medische macht en medische ethiek Hippocratic oath the physician must preserve human life, save it and prolong it, where and whenever possible today, with all the medical possibilities: the physician must preserve human life, save it and prolong it, wherever it is sensible and meaningful to do so. should the physician consider it no longer sensible to proceed, then he should be permitted to end patient´s life. This can be done in two ways: through ceasing all life-sustaining measures through actively terminating the life of the patient Sohn, W., Zenz, M., (eds) (2001) Euthanasia in Europe. Schattauer. Stuttgart, New York. p.138 Postma Case Leeuwarden 1973 Dr. Postma was sentenced to only one week in prison this remarkably mild sentence was based on the fact, that the physician´s mother was incurably ill she experienced her suffering as unbearable she was already in dying phase the ending of life was done on her own expressed wish Rotterdam criteria: 1982 the patient makes a voluntary request the request must be well considered the wish for death is durable the patient is in unacceptable suffering the physician has consulted a colleague who agrees the proposed course of action …without specific request… there is a difference between questions what would the patient want in this circumstances? what do you want for the patient? …without specific request… in 1990, besides the 2 300 cases of voluntary euthanasia and 400 cases of physician-assisted suicide per year, there were over 1 000 cases of active nonvoluntary euthanasia performed without the patient´s knowledge or consent, including roughly 140 cases (14 percent) in which the patients were mentally totally competent. (Kass, R.L., (2002) Life, Liberty and the Defense of Dignity. Encounter Books. New York, London. p. 201) Maas van der, P.J. et al., Euthanasia and Other Medical Decisions Concerning the End of Life (New York: Elseveir Science Inc., 1992) euthanasia ARGUMENTS FOR AND AGAINST Arguments For Euthanasia fear of living too long, without fatal illness to carry one off; hence, a right to assisted suicide fear of the degradations of senility and dependence; hence, a right to death with dignity fear of loss of control; hence, a right to choose the time and manner of one´s death Arguments For Euthanasia It provides a way to relieve extreme pain It provides a way of relief when a person's quality of life is low Frees up medical funds to help other people It is another case of freedom of choice Arguments For Euthanasia There are two general arguments used in favour of legalised euthanasia and assisted suicide. One is the ending of unbearable physical and/or psychological suffering in the case of terminal illness, and the other is to enhance individual autonomy. Arguments for euthanasia Refused by a court in Dijon the right to die under medical supervision, she was found dead at home. According to prosecutors, she had taken a "deadly dose" of barbiturates. Chantal Sebire died March 19, 2008 Arguments Against Euthanasia: Euthanasia devalues human life Euthanasia can become a means of health care cost containment Physicians and other medical care people should not be involved in directly causing death There is a "slippery slope" effect that has occurred where euthanasia has been first been legalized for only the terminally ill and later laws are changed to allow it for other people or to be done non-voluntarily. Arguments Against Euthanasia: Immanuel Kant Kant offered the "formula of the end in itself" as: "Act in such a way that you treat humanity, whether in your own person or in the person of another, always at the same time as an end and never simply as a means." This places more emphasis on the unique value of human life as deserving of our ultimate moral respect and thus proposes a more personal view of morality. In application to particular cases, of course, it yields the same results: violating a perfect duty by making a false promise (or killing myself) would be to treat another person (or myself) merely as a means for getting money (or avoiding pain) Arguments against euthanasia Emotional and psychological pressures could become overpowering for depressed or dependent people. If the choice of euthanasia is considered as good as a decision to receive care, many people will feel guilty for not choosing death. Financial considerations, added to the concern about "being a burden," could serve as powerful forces that would lead a person to "choose" euthanasia or assisted suicide. Dysthanasia USA: about half of all patients spent their last days in what the researches termed „an undesirable state“, including a week or so in an intensive care unit having a physician who was unaware of wishes not to be resuscitated being in serious, insufficiently treated pain the enthusiasm for physician-assisted suicide is driven, in part, by the fear that we will receive overly aggressive care at the end of life and that our suffering may be prolonged Euthanasia THE WORLD MEDICAL ASSOCIATION RESOLUTION ON EUTHANASIA Adopted by the WMA General Assembly, Washington 2002 May 2001 20.3/2001 Euthanasia „Euthanasia, that is the act of deliberately ending the life of a patient, even at the patient's own request or at the request of close relatives, is unethical. This does not prevent the physician from respecting the desire of a patient to allow the natural process of death to follow its course in the terminal phase of sickness." Euthanasia WMA , 1994: „Physicians-assisted suicide, like euthanasia, is unethical and must be condemned by the medical profession. Where the assistance of the physician is intentionally and deliberately directed at enabling an individual to end his or her own life, the physician acts unethically. However the right to decline medical treatment is a basic right of the patient and the physician does not act unethically even if respecting such a wish results in the death of the patient." Euthanasia BE IT RESOLVED that: 1. The World Medical Association reaffirms its strong belief that euthanasia is in conflict with basic ethical principles of medical practice, and Euthanasia The World Medical Association strongly encourages all National Medical Associations and physicians to refrain from participating in euthanasia, even if national law allows it or decriminalizes it under certain conditions. Physicians should not abandon dying patients but should continue to provide compassionate care even when cure is no longer possible Hippocratic Oath I will not give a lethal drug to anyone if I am asked, nor will I advise such a plan; Protecting human rights and dignity by taking into account previously expressed wishes of patients 25 January 2012 5. This resolution is not intended to deal with the issues of euthanasia or assisted suicide. Euthanasia, in the sense of the intentional killing by act or omission of a dependent human being for his or her alleged benefit, must always be prohibited. This resolution thus limits itself to the question of advance directives, living wills and continuing powers of attorney. http://www.assembly.coe.int/Mainf.asp?link=/Documents/AdoptedText/ta12/ERES1859.htm 2014 Marek Vácha ADVANCE DIRECTIVES PREVIOUSLY EXPRESSED WISHES OF PATIENTS Four Principles of Medical Ethics Nonmaleficence Beneficence Autonomy Justice Autonomy Patient has the right, as a competent adult, to refuse any proposed treatment, even if doing so may mean that he/she will become sicker or even die. If a competent person is sick, our legal tradition recognizes that he must want to be made well; the state cannot force him to have an operation or take his medication. Advance Care Planning = process whereby a patient, in consultation with healthcare providers, family members, and important others, makes decisions about his or her future healthcare „Every human being of adult years and sound mind has the right to determine what shall be done with his own body.“ (Benjamin Cardozzo´s statement, 1914) USA state laws allow individuals to complete advance directives documents and to name healthcare decision makers federal law requires all patients admitted to hospital to be notified of this right most european countries have followed suit with provisions for advance care planning LIWING WILL Living Will PROBLEMS Substituted judgement and best interests Substituted judgements liwing will, advanced directives without an advance directive, a proxy may then refer to the patient´s values, both implicit and explicit, regarding worldview (including religious beliefs), lifestyle, and health care. Best interests in many cases, a proxy may not have any information a bout a paataient´s values (infant, young children, mentally disabled adults) health is preferable to ilness, and life is preferable to death Order of Priority 1. current express preferences of a competent patient (informed consent) 2. past express preferences (living will) 3. what the patient would now want if he/she were competent (substituted judgment) 4. best interest Davis, J.K., (2009) Precedent Autonomy and End-of-Life Care. in Steinbock, B., (ed) The Oxford Handbook of Bioethics. Oxford University Press, Oxford. FOURTH YEAR 2013 Marek Vácha Deník Metro, 20/11/2012 Metro Journal: „Big Discovery. The Scientists can destroy a HIV bacteria.“ AIDS BIOLOGY AND ETHICS The Case of the Infected Spouse The following fictionalized case is based on an actual incident. 1982: After moving to Honolulu, Wilma and Andrew Long visit your office and ask you to be their family physician. They have been your patients ever since. 1988: Six years later the two decide to separate. Wilma leaves for the Mainland, occasionally sending you a postcard. Though you do not see her professionally, you still think of yourself as her doctor The Case of the Infected Spouse 1990: Andrew comes in and says that he has embarked upon a more sophisticated social life. He has been hearing about some new sexually transmitted deseases and wants to be tested. Testing reveals that he is positive for the AIDS virus, and he receives appropriate counseling. 1991: Visiting your office for a checkup, Andrew tells you Wilma is returning to Hawaii for reconciliation with him. She arrives that afternoon and will be staying at the Moana Hotel. Despite your best efforts to persuade him, Andrew leaves without giving you assurance that he will tell Wilma about his infection or protect her against becoming The Case of the Infected Spouse Do you take steps to see that Wilma is warned? Kipnis, K., A Defense of Unqualified Medical Confidentiality. The American Journal of Bioethics 6, no. 2 (2006): 7 - 18 Solution Counseling the patient to notify his partners voluntarily. If the patient is unwilling to notify their partners the nest step is to notify the Department of Health to start theproocess of contact tracing. 3. The health department interviews the patient and attempts to construct a list of partners in order to notify them 1. 2. 1. this is a voluntary process and there is neither a penalty nor criminal threat of prosecution if the patient chooses not to comply. The health department then sends notice to the partner that there is a health-related issue to discuss and the partner is notified in person of their potential exposure to HIV. 4. 1. The name of the source patient is never revealed to the partner and the confidentality of the original partner is maintained. Solution If the patient is unwilling to dislclose the maens of his contacts you cannot compel him to do so. There is no incarceration or criminal penalty for not disclosing these names. If a patient will not notify his partners and you have certain knowledge of the partner at risk, you have legal immunity to carry out the notification yourself. There is a legal protection if you do notify the partner, but it is not mandatory for you to do so. No one has ever been successfully prosecuted for violating a patient´s confidentiality if it is to warn another person who is at risk. Case You have a patient in your clinic who is accompanied by her boyfriend She is clearly having unprotected sex because she is pregnant. When you ask if her boyfriend knows her HIV status she says, „Of course not – he might leave me if I told him.“ You strongly encourage her to tell him her HIV status On a subsequent visit, when you ask her if she has notified her partner she says „Not yet.“ You know the boyfriend because he accompanies her to the office visits. What should you do? Solution You have legal immunity if you notify the partner. At this point either you can ask the health department to notify the partner or you may do it yourself if the partner were to seroconvert for HIV and you did not make sure he was notified you would be legally liable because you did not follow your duty to warn. this is similar to having a psychiatric patient who told you he was going to harm someone. Although you have a duty to maintain the confidentiality of the patient, you also have a duty to inform the person at risk. HIV AND AIDS IN NUMBERS The number of people living with HIV rose from around 8 million in 1990 to 34 million by the end of 2010. The overall growth of the epidemic has stabilised in recent years. The annual number of new HIV infections has steadily declined and due to the significant increase in people receiving antiretroviral therapy, the number of AIDS-related deaths has also declined. Since the beginning of the epidemic, nearly 30 million people have died from AIDS-related causes http://www.avert.org/worldstats.htm The number of AIDS-related deaths declined by nearly one-third in subSaharan Africa between 2005 and 2011. The Caribbean experienced declines in AIDS- related deaths of 48% between 2005 and 2011 and Oceania 41%. However two regions experienced significant increases in AIDS-related deaths; Eastern Europe and Central Asia (21%) and the Middle East and North Africa (17%). Cost of AIDS when one considers personal medical costs, direct costs of research, and indirect costs such as education, screening, and potential productivity losses, the disease carries a yearly price tag of over $ 8 billion 2012 the population affected by the disease has extended to all groups from „high-risk groups“ to „high-risk behaviours“ BIOLOGY OF HIV AIDS 1981: On June 5, the Centers for Disese Control (CDC) Mortality and Morbidity Report listed an unusual outbreak of opportunistic infections such as Pneumocystis carinii pneumonia among gay men "gay cancer" T-lymocyte infected by HIV (blue) History GRID - gay-related immune disorder july 1981 108 cases reported, 43 individuas had died 1982: Acquired Immunodeficiency Syndrome becomes the term used by the CDC to describe thr unusual outbreak of opportunistic infection 1984: Virus HIV is identified by a team of French scientists Harald zur Hausen Born 1936 German Cancer Research Center, Heidelberg, Germany Françoise BarréSinoussi Born 1947 Institut Pasteur, Paris, France Luc Montagnier Born 1932 World Foundation for AIDS Research and Prevention, Paris, France 2013 AIDS ETHICS Ethical Problems Do health care practitioners have a duty to treat? What is an acceptable risk for health care professionals? Should the patient be warned if the health care practitioner is HIV positive? Should the practitioner be warned of the patient is HIV positive? Should infected practitioners be allowed to continue practice? What is the meaning of confidentiality when it comes to AIDS, and who should be told? It is ethically unacceptable to refuse to treat HIV or take care of HIV-positive patients simply because they are HIVpositive. 2006: change http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5514a1.htm CDC changed its recommendation about HIV screening for patients in health care settings the recommendations moved away from specific, explicit informed consent, usually in written form, to general, implicit consent as part of the acceptance of medical care. previous policies required specific disclosure of information and a decision to accept or refuse testing. specific, explicit consent would still be expected in nonclinical settings 2006: change http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5514a1.htm For pregnant women HIV screening should be included in the routine panel of prenatal screening tests for all pregnant women. HIV screening is recommended after the patient is notified that testing will be performed unless the patient declines (opt-out screening). Separate written consent for HIV testing should not be required; general consent for medical care should be considered sufficient to encompass consent for HIV testing. Repeat screening in the third trimester is recommended in certain jurisdictions with elevated rates of HIV infection among pregnant women. Reagan Administration: „conservative“ approach no sex before marriage faithfullness in marriage no drugs Clinton Administration: „pragmatic“ approach HIV is not transmissed by sexual intercourse, byt by unprotected sexual intercourse condom throwaway needles Bushova administrativa 2004 2008 ABC program abstinence be faithful condoms CZECH REP. AIDS centra 1. AIDS Centrum FN Bulovka, Infekční klinika, Budínova 2, Praha 8, tel.: 266 082 629 2. AIDS Centrum České Budějovice, Nemocnice, B.Němcové 54, České Budějovice, tel.: 387 874 656 3. AIDS Centrum Plzeň, Infekční klinika FN, Dr. Beneše 13, Plzeň, tel.:377 402 546 (2264) 4. AIDS Centrum Ústí n.L., Masarykova nemocnice, Ústí n.L., tel.: 472 770 270 5. AIDS Centrum Hradec Králové, Infekční klinika FN, Hradec Králové, tel.: 495 832 531 6. AIDS Centrum Brno, FN Bohunice, Jihlavská 20, Brno, tel.:547 192 276. 7. AIDS Centrum Ostrava, FNsP Ostrava, 17 listopadu 1790, Ostrava-Poruba, tel.: 596 984 253-4