PowerPoint Lecture Notes Presentation
Chapter 14
Disorders of Childhood
Abnormal Psychology, Eleventh Edition
by
Ann M. Kring, Gerald C. Davison, John M. Neale,
& Sheri L. Johnson
Classification and Diagnosis of
Childhood Disorders
Developmental psychopathology
» Studies disorders within context of normal child
development
Externalizing disorders
» Characterized by outward behaviors
» Noncompliance, aggressiveness, overactivity,
impulsiveness
» Includes attention-deficit/hyperactivity disorder,
conduct disorder, and oppositional defiant disorder.
» More common in boys
Internalizing disorders
» Characterized by inward behaviors
– Depression, anxiety, social withdrawal
» Includes childhood anxiety and mood disorders
» More common in girls
Copyright 2009 John Wiley & Sons, NY
2
Copyright 2009 John Wiley & Sons, NY
3
Attention Deficit/Hyperactivity
Disorder
Excessive levels of activity
» Fidgeting, squirming, running around when
inappropriate, incessant talking
Distractibility and difficulty concentrating
» Makes careless mistakes, can’t follow instructions,
forgetful
Must be severe and persistent
» Present for at least 6 months and cause
impairments in functioning
Congress created National ADHD Awareness
Day
» First observed September 7, 2004
Copyright 2009 John Wiley & Sons, NY
4
Attention Deficit/Hyperactivity
Disorder
Three subcategories in DSM-IV-TR
1. Predominantly inattentive type
2. Predominantly hyperactive-impulsive type
3. Combined type
Differential diagnosis
»
»
ADHD or Conduct Disorder?
ADHD
–
»
More off-task behavior, cognitive & achievement deficits
Conduct Disorder
–
More aggressive, act out in most settings, antisocial
parents, family hostility
Copyright 2009 John Wiley & Sons, NY
5
Attention Deficit/Hyperactivity
Disorder
ADHD often comorbid with
anxiety and depression
Prevalence estimates 2 to
7% worldwide
More common in boys
than girls
»
May be because boys’
behavior more likely to be
aggressive
Symptoms persist beyond
childhood
»
»
Numerous longitudinal
studies show 65 to 80% still
exhibit symptoms
60% of adults continue to
meet criteria for ADHD in
remission
Copyright 2009 John Wiley & Sons, NY
6
Girls with Attention
Deficit/Hyperactivity Disorder
Hinshaw et al. (2006) large, ethnically diverse study of girls
» Combined type had:
– More disruptive behaviors than inattentive type
– More comorbid diagnoses of conduct disorder or oppositional
defiant disorder than girls without ADHD
– Viewed more negatively by peers than inattentive type or girls w/out
ADHD
» Inattentive type
– Viewed more negatively by peers than girls w/out ADHD
» Girls w/ADHD more likely to:
– Be anxious and depressed
– Exhibit neurological deficits (e.g., poor planning, problem-solving)
– Have symptoms of eating disorder and substance abuse by
adolescence
Copyright 2009 John Wiley & Sons, NY
7
Etiology of ADHD
Genetic factors
» Adoption and twin studies
– Heritability estimates as high as 70 to 80%
» Two dopamine genes implicated
– DRD4
Dopamine receptor gene
– DAT1
Dopamine transporter gene
» Mixed support for this gene
» Either gene associated with increased risk only when
prenatal maternal nicotine or alcohol use are present
Neurobiological factors
» Dopaminergic areas smaller in children with ADHD
– Frontal lobes, caudate nucleus, globus pallidus
» Poor performance on tests of frontal lobe function
Copyright 2009 John Wiley & Sons, NY
8
Etiology of ADHD
Perinatal and prenatal factors
» Low birth weight
– Can be mitigated by later maternal warmth
» Maternal tobacco and alcohol use
Environmental toxins
» Limited evidence that food additives can have a small
impact on hyperactive behavior
» No evidence that refined sugar causes ADHD
» Nicotine from maternal smoking
– Exposure to tobacco in utero associated with ADHD
symptoms
– May damage dopaminergic system resulting in behavioral
disinhibition
Copyright 2009 John Wiley & Sons, NY
9
Etiology of ADHD
Parent-child relationship
» Parents give more commands and have
more negative interactions
» Family factors
– Interact with genetic and neurobiological factors
– Contribute to or maintain ADHD behaviors but
do not cause them
Copyright 2009 John Wiley & Sons, NY
10
Treatment of ADHD
Stimulant medications (Ritalin, Adderall, Concerta,
Strattera)
»
»
»
»
»
Reduce disruptive behavior
Improve interactions with parents, teachers, peers
Improve goal-directed behavior and concentration
Reduce aggression
Side effects
– Loss of appetite, weight
– Sleep problems
Medication plus behavioral treatment (MTA study)
»
»
»
»
Slightly better than meds alone
Improved social skills whereas meds alone did not
No difference in groups at 3 year follow-up
Stimulant medication more effective for some children than
others
Copyright 2009 John Wiley & Sons, NY
11
Treatment of ADHD
Psychological treatment
» Parental training
» Change in classroom management
» Behavior monitoring and reinforcement of
appropriate behavior
Supportive classroom structure
»
»
»
»
Brief assignments
Immediate feedback
Task-focused style
Breaks for exercise
Copyright 2009 John Wiley & Sons, NY
12
Conduct Disorder (CD)
Pattern of engaging in behaviors that violate
social norms, the rights of others, and are
often illegal.
»
»
»
»
»
»
Aggression
Cruelty towards other people or animals
Lying
Stealing
Vandalism
Often accompanied by lack of remorse and
callousness
» Frequent and severe offenses
Copyright 2009 John Wiley & Sons, NY
13
Oppositional Defiant Disorder (ODD)
ODD behaviors do not meet criteria for CD but
child displays pattern of defiant behavior
»
»
»
»
»
»
Argumentative
Loses temper
Lack of compliance
Deliberately aggravates others
Hostile, vindictive, spiteful, or touchy
Blames others for their problems
Comorbid with ADHD, learning and
communication disorders
» Disruptive behavior of ODD more deliberate than ADHD
Most often diagnosed in boys but may be as
prevalent in girls
Copyright 2009 John Wiley & Sons, NY
14
Conduct Disorder (CD)
CD behavior impacts others
Many times first identified by criminal justice system
Substance abuse common
» Unclear whether it precedes or is concomitant
with disorder
Comorbid with anxiety and depression
» Comorbidity rates vary from 15 to 45%
» CD precedes anxiety and depression
Prevalence
» Boys
– 4 to 16%
» Girls
– 1.2 to 9%
Copyright 2009 John Wiley & Sons, NY
15
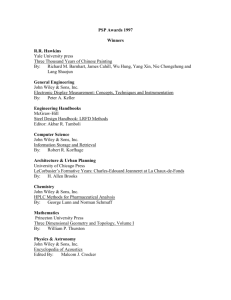
Figure 14.1 Arrest Rates Across Ages for
Homicide, Forcible Rape, Robber, Aggravated
Assault, and Auto Theft
Copyright 2009 John Wiley & Sons, NY
16
Conduct Disorder (CD)
Moffitt (1993, 2006, 2007) two distinct CD types
1.
Life-course-persistent
–
2.
10 – 15x more common in boys than girls
Adolescence-limited
Follow-up longitudinal studies of life-coursepersistent show more severe problems into early
adulthood including:
»
»
»
»
Psychopathology
Lower levels of education
Partner and child abuse
Violent behavior
Copyright 2009 John Wiley & Sons, NY
17
Figure 14.2 Etiology of Conduct
Disorder
Insert Figure 14.2
Copyright 2009 John Wiley & Sons, NY
18
Etiology of Conduct Disorder (CD)
Genetic factors
»
»
»
Meta-analysis of twin and adoption studies
suggest 40 – 50% of antisocial behavior is
heritable
»
Heritability likely plays a part
Twin study data show mixed results
Adoption studies focused on criminal behavior, not
conduct disorder
Genetics a stronger influence when behaviors begin
in childhood rather than adolescence
Genetics and environment interact (Caspi et al.,
2002)
»
Abuse as a child PLUS low MAOA activity most likely
to develop CD
Copyright 2009 John Wiley & Sons, NY
19
Etiology of Conduct Disorder (CD)
Neurobiological factors
»
»
»
»
Poor verbal skills
Difficulty with executive functioning
Low IQ
Lower levels of resting skin conductance and HR
Psychological factors
»
»
»
»
»
Deficient moral development, especially lack of remorse
Modeling and reinforcement of aggressive behavior
Harsh and inconsistent parenting
Lack of parental monitoring
Cognitive bias (Kenneth Dodge)
–
Neutral acts by others perceived as hostile
Copyright 2009 John Wiley & Sons, NY
20
Figure 14.3 Dodge’s Cognitive
Theory of Aggression
Insert
figure 14.3
Copyright 2009 John Wiley & Sons, NY
21
Etiology of Conduct Disorder (CD)
Peer influence
»
»
Sociocultural factors
»
»
Acceptance or rejection by peers
Affiliation with deviant peers
Poverty
Urban environment
Higher rates of delinquent acts among
African American males linked to living in
poorer neighborhoods rather than race.
(Peeples & Loeber,1994)
Copyright 2009 John Wiley & Sons, NY
22
Treatment of Conduct Disorder
Family interventions
» Family check-ups (FCU) associated with
less disruptive behavior
» Parental management train (PMT; Gerald
Patterson)
– Teach parents to reward prosocial behavior
Cognitive therapy
» Anger-control training
Copyright 2009 John Wiley & Sons, NY
23
Figure 14.4 Multisystemic Treatment
of CD
Insert Figure 14.4
Copyright 2009 John Wiley & Sons, NY
24
Depression in Children and
Adolescents
Symptoms common to
children, adolescents,
and adults
» Depressed mood
» Inability to experience
pleasure
» Fatigue
» Problems concentrating
» Suicidal ideation
Symptoms specific to
children & adolescents
» Higher rates of suicide
attempts and guilt
» Lower rates of
– Early morning
awakening
– Early morning
depression
– Loss of appetite
– Weight loss
Copyright 2009 John Wiley & Sons, NY
25
Depression and Anxiety in
Children and Adolescents
Commonly co-occur with ADHD and CD
Also co-occur with each other
Early research suggested that depression and
anxiety could be distinguished from one another
in the same way they are in adults:
» Depression – high negative affect, low positive
affect
» Anxiety – high negative affect but not low levels of
positive affect
» More recent research calls this finding into
question
Copyright 2009 John Wiley & Sons, NY
26
Depression in Children and
Adolescents
Depression recurrent
Prevalence
» 1% of preschoolers
» 2 – 3% of school age children
» Adolescent rates equivalent to adult levels
» Girls
– 7 – 13% - Twice that of boys
– No difference in symptoms experienced
Copyright 2009 John Wiley & Sons, NY
27
Etiology of Depression in Children
and Adolescents
Genetic factors
Early adversity and negative life events
Family and relationship factors
» A parent who is depressed
» Parental rejection only modestly associated with depression
» Children with depression and their parents interact in
negative ways
– Less warmth
– More hostility
Cognitive distortions and negative attributional style
Stable attributional style (Cole et al., 2008)
» Develops by early adolescence
» By middle school, attributional style serves as a cognitive
diathesis for depression.
Copyright 2009 John Wiley & Sons, NY
28
Treatment of Depression in Children
and Adolescents
Medications
SSRIs more effective than tricyclics
» Meta-analysis showed medications most effective for anxiety
other than OCD
– Less effective for depression and OCD
Concerns about medications
» Side effects including diarrhea, nausea, sleep problems, and
agitation
» Possibility of increased risk of suicide attempts
CBT
» More effective for Caucasian adolescents, those with
pretreatment good coping skills, and recurrent depression
Interpersonal psychotherapy (IPT)
» Focuses on peer pressures, transition to adulthood, and
issues related to independence
Psychotherapy generally only modestly effective with
children and adolescents
» CBT no better than non-CBT therapies
Copyright 2009 John Wiley & Sons, NY
29
Anxiety in Children and Adolescents
Fears and worries common in childhood
Anxiety disorder
» More severe and persistent worry
» Must interfere with functioning
Most childhood fears disappear but adults
with anxiety disorders report feeling
anxious as children
» “I’ve always been this way”
Prevalence
» 12 to 20% of children and adolescents would
be diagnosed with anxiety disorder
Copyright 2009 John Wiley & Sons, NY
30
School Phobia (School Refusal)
Two types
1. Separation anxiety
» Worry about parental or personal safety when
at school
2. Fear of school
» Specific aspect of school environment (e.g.,
academic failure) or social phobia
» Begins later in childhood
» More severe and pervasive avoidance
Copyright 2009 John Wiley & Sons, NY
31
Social Phobia
Extreme shyness and withdrawal
May exhibit selective mutism
» Refusal to speak in unfamiliar social setting
Prevalence
» 1% of children and adolescents
Etiology
» Overestimation of threat
» Underestimation of coping ability
» Poor social skills
Copyright 2009 John Wiley & Sons, NY
32
PTSD
Exposure to trauma
»
»
»
Chronic physical or sexual abuse
Community violence
Natural disasters
Symptom categories
»
»
»
Flashbacks, nightmares, intrusive thoughts
Avoidance
Hyperarousal and vigilance
Etiology
»
»
»
Preexisting anxiety
Family stress and coping styles
Parental response to trauma
Copyright 2009 John Wiley & Sons, NY
33
OCD
Prevalence 1 to 4%
Symptoms similar to those in adults
Most common obsessions
» Contamination from dirt and germs
» Aggression
» Thoughts about sex and religion more
common in adolescence
OCD more common in boys than girls
Copyright 2009 John Wiley & Sons, NY
34
Etiology of Anxiety Disorders
Genetics
» Heritability estimates from 29 – 50%
» Genetics plays a stronger role in separation anxiety in
context of more negative life events
Parenting plays a small role in anxiety disorders
» Only 4% of variance
Emotion regulation and attachment problems also play a
role
Perception of lack of acceptance by peers a factor in social
phobia
Risk factors for PTSD include:
» Family stress and coping style
» Past experience with trauma
Copyright 2009 John Wiley & Sons, NY
35
Treatment of Anxiety Disorders in
Childhood and Adolescence
Exposure to feared object
» Reward approach behavior
CBT Kendall’s Coping Cat program
» Shows to be effective in two randomized clinical trials
» For kids between 7 and 13 years old
» Cognitive restructuring
– Develop new ways to think about feats
»
»
»
»
»
Psychoeducation
Modeling and exposure
Skills training
Relapse prevention
Family involved in treatment
Copyright 2009 John Wiley & Sons, NY
36
Learning Disability
Evidence of inadequate development in a
specific area of academic, language, speech
or motor skills
» e.g., arithmetic or reading
Not due to mental retardation, autism,
physical disorder or lack of educational
opportunity
Individual usually average or above average
intelligence
Copyright 2009 John Wiley & Sons, NY
37
Learning Disability
DSM-IV-TR categories
» Learning disorders
» Communication disorders
» Motor skills disorder
Often identified and treated in school
Reading disorders more common in
boys
Copyright 2009 John Wiley & Sons, NY
38
Table 14.3 Learning Disorders in
DSM-IV-TR
Copyright 2009 John Wiley & Sons, NY
39
Etiology of Learning Disabilities:
Dyslexia
Genetic factors
» Evidence from family and twin studies
» Genes are those associated with typical reading abilities
“generalist genes”
Problems in language processing
»
»
»
»
»
»
Speech perception
Analysis of sounds and their relationship to printed words
Difficulty recognizing rhyme and alliteration
Problems naming familiar objects rapidly
Delays learning syntactic rules
Deficient phonological awareness
– Inadequate left temporo-parietal-occipital activation
Copyright 2009 John Wiley & Sons, NY
40
Treatment of Learning Disabilities
Reading and writing disorders
» Multisensory instruction in listening, speaking, and
writing skills
» Readiness skills in younger children as preparation
for learning to read
» Phonics instruction
Communication disorders
» Fast ForWord
– Involves computer games and audiotapes that slow
speech sounds
Copyright 2009 John Wiley & Sons, NY
41
Mental Retardation
Significantly below average intellectual
functioning
» IQ less than 70
Deficits in adaptive functioning
» Self-care, communication, home living, decision
making, etc.
Onset before age 18
Most professionals focus on strengths of
individual to assess ability to function
Intellectual disability now preferred term over
mental retardation
Copyright 2009 John Wiley & Sons, NY
42
Table 14.4 Sample Items from
Vineland Adaptive Behavior Scales
Copyright 2009 John Wiley & Sons, NY
43
Table 14.5 DSM-IV-TR Categories of
Mental Retardation
Copyright 2009 John Wiley & Sons, NY
44
Table 14.6 AAMR Definition of
Mental Retardation
Copyright 2009 John Wiley & Sons, NY
45
Etiology of Mental Retardation:
Neurological Factors
Down’s syndrome
» Chromosomal trisomy
» 47 instead of 46 chromosomes
Fragile X syndrome
» Mutation in the fMRI gene on the X chromosome
Recessive-gene disease
» Phenylketonuria (PKU)
Maternal infectious disease, especially during 1st
trimester
» HIV, rubella, syphilis
Brain injuries from falls or auto accidents
Lead or mercury poisoning
Copyright 2009 John Wiley & Sons, NY
46
Treatment of Mental Retardation
Residential treatment
» Small to medium sized community residences
Behavioral treatments
» Language, social, and motor skills training
» Method of successive approximation to teach
basic self-care skills in severely retarded
– e.g., holding a spoon, toileting
» Applied behavioral analysis
Cognitive treatments
» Problem-solving strategies
Computer assisted instruction
Copyright 2009 John Wiley & Sons, NY
47
Pervasive Developmental
Disorder: Autistic Disorder
Kanner’s (1943) autistic aloneness
Impairments in social interactions (at least
2 of the following):
» Deficient use of nonverbal behaviors
» Poorly developed peer relationships
» Lack of social or emotional reciprocity
Impairments in communication (at least 1
of the following)
» Delay in or total lack of spoken language
» Difficulty initiating or sustaining conversation
– Repetitious or idiosyncratic language
– Echolalia
– Pronoun reversal
» Lack of developmentally appropriate play
Copyright 2009 John Wiley & Sons, NY
48
Pervasive Developmental
Disorder: Autistic Disorder
Repetitious or stereotyped behaviors (at
least 1 of the following)
» Abnormal preoccupation with objects
» Ritualized behaviors
– Body rocking, hand flapping
» Stereotyped mannerisms
» Abnormal preoccupation with parts of an
object
Begins before age 3
Copyright 2009 John Wiley & Sons, NY
49
Autistic Disorder
A study with adults found that people
with autism pay attention to different
parts of faces than do people without
autism (Spezio et al., 2007).
» Adults with autism focused their gaze
mostly on the mouth region and almost
entirely neglected the eye region.
» This neglect likely contributes to difficulties
in perceiving emotion in other people
Copyright 2009 John Wiley & Sons, NY
50
Etiology of Autistic Disorder
Bettleheim’s psychoanalytic theory
(1967)
» Rejecting and unresponsive parents
» Child withdraws into his own world
» Theory unsupported by empirical data
Genetic factors
» Twin studies
– 60 to 91% concordance rates
» Genetic flaw
– Deletion on chromosome 16
Copyright 2009 John Wiley & Sons, NY
51
Etiology of Autistic Disorder
Neurobiological factors
» Brain size
– Although normal size at birth, brains of autistic
adults and children are larger than normal.
– Pruning of neurons may not be occurring
“Overgrown” areas include the frontal,
temporal, and cerebellar, which have
been linked with language, social, and
emotional functions
Copyright 2009 John Wiley & Sons, NY
52
Treatment of Autistic Disorder
Intensive operant conditioning (Lovaas, 1987)
Parent training and education
Pivotal response treatment (Koegel et al., 2003)
» Focus on increasing child’s motivation and
responsiveness rather than discrete behaviors
Joint attention intervention & symbolic play used
to improve attention and expressive skills
Medication most common used
» Haloperidol (Haldol)
– Antipsychotic
– Reduces aggression and stereotyped motor behavior
– Does not improve language and interpersonal
relationships
Copyright 2009 John Wiley & Sons, NY
53
Pervasive Developmental Disorders
Asperger’s disorder
» Less severe form of autism
» Language and intelligence intact
» Poor social relationships and rigid,
stereotyped behaviors
» Recently recognized more in adult
population
Copyright 2009 John Wiley & Sons, NY
54
Table 14.7 Additional Pervasive
Developmental Disorders
Copyright 2009 John Wiley & Sons, NY
55
COPYRIGHT
Copyright 2009 by John Wiley & Sons, New
York, NY. All rights reserved. No part of the
material protected by this copyright may be
reproduced or utilized in any form or by any
means, electronic or mechanical, including
photocopying, recording or by any information
storage and retrieval system, without written
permission of the copyright owner.
Copyright 2009 John Wiley & Sons, NY
56