mCRC - Oncología Clínica / Hematología
advertisement

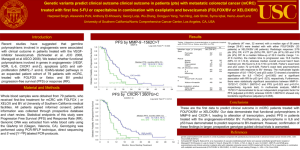
Avances en terapia sistémica en cáncer metastásico de colon y recto (mCRC) Mauricio Lema Medina MD Clínica de Oncología Astorga – Clínica SOMA – Medicáncer Medellín, Colombia Temario (107) Consideraciones iniciales: Vías de transducción de señales (EGFR), y angiogénesis en mCRC (15) Evolución histórica del tratamiento del mCRC -1: Citostáticos convencionales (12) Mecanismos de acción del Bevacizumab y los MOAs anti EGFR (10) Evolución histórica del tratamiento del mCRC -2: Terapia molecular dirigida (39) – Bevacizumab en mCRC (31) – Cetuximab en mCRC (8) Evolución histórica del tratamiento del mCRC -3: Terapia individualizada (29) – Impacto de las alteraciones en las vías de transducción de señales del EGFR en la eficacia de Cetuximab (20) – (Ausencia de) Impacto de las alteraciones en las vías de trasnducción de señales del EGFR en la eficacia de Bevacizumab (9) Conclusiones (2) Efectos adversos del Bevacizumab y de los MOAs anti EGFR (14) Page 2 Consideraciones iniciales: Vías de transducción de señales (EGFR), y angiogénesis en mCRC Page 4 Page 5 EGFR es una proteina transmembrana Dominio Extracelular Dominio Transmembrana Dominio intracelular Page 6 La activación del EGFR activa múltiples procesos Shc Grb2 PI3-K Sos-1 Ras AKT MEKK-1 Raf MEK mTOR Page 7 MKK-7 ERK La activación del EGFR activa múltiples procesos Shc Grb2 PI3-K Sos-1 Ras AKT MEKK-1 Raf MEK mTOR Page 8 MKK-7 ERK La activación del EGFR activa múltiples procesos Shc Grb2 PI3-K Sos-1 Ras AKT MEKK-1 Raf MEK mTOR MKK-7 ERK JNK Page 9 Apoptosis Resistance Proliferation Angiogenesis Metastasis Page 10 Page 11 Targeting the EGFR pathway: K-Ras mutations EGFR overexpression: • CRC (27–77%) • Pancreatic cancer (30–50%) • Lung cancer (40–80%) • NSCLC (14–91%) TGF-α Sos EGFR* K-Ras* Grb2 B-Raf* EGFR mutation: • NSCLC (10%) • Glioblastoma (20%) MEK MAPK *Mutated in human cancers NSCLC = non-small cell lung cancer Page 12 TGF = transforming growth factor K-Ras mutation: • CRC (30–50%) • Pancreatic cancer (90%) • Papillary thyroid cancer (60%) • NSCLC (30%) B-Raf mutation: • CRC (10%) • Melanoma (70%) • Papillary thyroid cancer (50%) Adapted from Roberts Der. Oncogene 2007 CRC: Adenoma-Carcinoma Sequence Normal Colon APC hMSH2 hMLH1 abnormalities (hereditary) Hyperproliferative Epithelium Methylation abnormalities APC hMSH2 hMLH1 inactivation Adenoma KRAS mutation 18q deletion 32% to 57% KRAS mutant Page 13 Carcinoma p53 deletion Further accumulation of genetic abnormalities Targeting the EGFR pathway TGF-α extracellular R intracellular R Grb2 K K Shc mutation loss Grb2 PI3K Sos Ras Akt PTEN mTOR phosphorylation Sos FKHR GSK–3 Raf Bad p27 mutation mutation MEK1/2 MAPK Cyclin D1, E Cell cycle progression Page 14 Survival Proliferation Mendelsohn et al. JCO 2003 VEGF: Un Mediador Clave de Angiogenesis Aumento de los niveles de VEGF Genes implicados en tumorogénesis (p53, p73, src, ras, vHL, bcr-abl) Factores ambientales (hipoxia, pH) Factores de crecimiento, Hormonas (EGF, bFGF, PDGF, IGF-1, IL-1, IL-6, estrogen) bFGF, basic fibroblast growth factors; EGF, epidermal growth factor; IGF, insulin-like growth factor; IL, interleukin; PDGF, platelet-derived growth factor; VEGFR, VEGF receptor. 1. Dvorak HF. J Clin Oncol. 2002;20:4368-4380; 2. Ebos JM, et al. Mol Cancer Res. 2002;1:89-95; 3. Page 15 N, et al. Nat Med. 2003;9:669-676. Ferrara VEGF: Un Mediador Clave de Angiogenesis Unión y activación del VEGFR VEGF P P PLC PKC IP3 Surviva l Page 16 PI3-K AKT P P FAK Paxillin Ras MAPK Proliferation Migratio n ANGIOGENESIS Activación de la célula endotelial VEGF es expresado durante toda la historia natural bFGF bFGF bFGF TGFb-1 TGFb-1 VEGF VEGF VEGF VEGF TGFb-1 PIGF bFGF TGFb-1 VEGF PIGF PIGF PD-ECGF PD-ECGF Pleiotrophin Evolución tumoral bFGF = basic fibroblast growth factor TGFb-1 = transforming growth factor b-1 PIGF = placenta growth factor PD-ECGF = platelet-derived endothelial cell growth factor Page 17 www.clinicaloptions.com Adapted from Folkman. Cancer. Principles and practice of oncology 2005 Evolución histórica del tratamiento mCRC – 1: Citostáticos convencionales Evolución histórica del manejo de mCRC ¿ Hacia una enfermedad crónica ? Terapia de soporte K-Ras mutado factor pronóstico adverso, y predictivo de no respuesta contra terapia dirigida con EGFR Oxaliplatino Capecitabina Irinotecán 1985 1990 1998 Fluoruracilo inicia la terapia antineoplásica Page 19 2004 Bevacizumab Cetuximab 2009 Nuevas molécultas están siendo evaluadas…. Quimioterapia en mCRC Citostáticos convencionales Inhibidores TS Fluoruracilo (IV) Inhibidores Topo-I Irinotecán Capecitabina (PO) Raltitrexed (IV) Alquilantes Oxaliplatino Comentarios 4 Modulación con folinato incrementa respuesta de Fluoruracilo. Oxaliplatino es inactivo como monoagente TS: Timidilato sintestasa; Topo-I: Topoisomerasa I Page 20 La combinación de 3 agentes citotóxicos incrementa la supervivencia mediana a 17-20 meses en mCRC Supervivencia mediana BSC 35 30 Aproximadamente 6 meses Meses 25 20 15 10 5 0 1980 Page 21 1985 BSC = mejor terapia de soporte 1990 1995 2000 Fluoropirimidines en mCRC No cambio en la supervivencia mediana con diferentes esquemas – Supervivencia mediana: ~ 12 meses Regimen Respuesta, % 5-FU en bolo 7-15 5-FU en infusión 20-30 5-FU/LV Mayo, Roswell Park 12-35 de Gramont (LV5-FU2) 28-33 AIO (cada semana, 24-hour infusion) 25-44 Capecitabina 20-25 Grothey A, et al. J Clin Oncol. 2005;23:9441-9442. Page 22 www.clinicaloptions.com IFL vs FOLFOX vs IROX (N9741) diseño IFL (n=264) R n=795 FOLFOX (n=267) IROX (n=264) Primary endpoint: PFS Goldberg et al, JCO 2004 Page 23 Bolo (IFL) vs infusión (FOLFOX) FOLFOX4: ciclo de 14-días 5-FU 600mg/m2 iv 22 h LV 200mg/m2 iv 2 h d2 d1 5-FU 400mg/m2 iv bolus LV 200mg/m2 iv 2 h 5-FU 400mg/m2 iv bolus OX 85mg/m2 iv 2 h 5-FU 600mg/m2 iv 22 h d3 IFL LV 20mg/m2 iv 2 h 1 Page 24 8 5-FU 500mg/m2 iv bolus Iri 125mg/m2 iv 1.5 h 15 22 5-FU = 5-fluorouracilo; LV = leucovorin (Folinato de calcio); OX = oxaliplatino; Iri = Irinotecán Page 25 N9741: Sanoff HK. J Clin Oncol 26:5721-5727. N9741 Resultados n IFL 264 FOLFOX 267 IROX 264 RR (%) 31 45 35 PFS (m) 6.9 8.7 6.5 OS (m) 15 19.5 17.4 p Goldberg et al, JCO 2004 Page 26 0.0001 Efficacy: Sequence FOLFIRI/FOLFOX Arm A Arm B Results FOLFIRI FOLFOX FOLFOX FOLFIRI Patients, n 109 81 111 69 Confirmed RR, % 56 15 54 4 TTP, mos 8.5 4.2 8.0 2.5 Survival, mos 21.5 20.6 No statistically significant differences in first- or second-line therapy RR or TTP and OS Page 27 Tournigand C, et al. J Clin Oncol. 2004;22:229-237. XELOX y FOLFOX4 XELOX: 21-day cycle OX 130mg/m2 iv 2 h d1 Rest d2 OralCapecitabina (Xeloda) 1000mg/m2 bid d15 d21 FOLFOX4 + Avastin/placebo: 14-day cycle d1 Page 28 5-FU 600mg/m2 iv 22 h LV 200mg/m2 iv 2 h 5-FU 400mg/m2 iv bolus LV 200mg/m2 iv 2 h 5-FU 400mg/m2 iv bolus OX 85mg/m2 iv 2 h 5-FU 600mg/m2 iv 22 h d2 5-FU = 5-fluorouracil; LV = leucovorin; OX = oxaliplatin; PL = placebo d3 CapeOx Noninferior to FOLFOX Median follow-up: 17.7 mos HR for PFS: 1.04 (97.5% CI: 0.93-1.16) – Upper limit of 97.5% CI: < 1.23 (noninferiority margin) PFS Events, n Median (ITT), mos Page 29 CapeOx/ CapeOx + Placebo/ CapeOx + Bevacizumab (n = 1017) FOLFOX-4/ FOLFOX-4 + Placebo/ FOLFOX-4 + Bevacizumab (n = 1017) 813 826 8 8.5 Cassidy J, et al. J Clin Oncol. 2008;26:2006-2012. Plateau de la eficacia de la quimioterapia convencional en mCRC La supervivencia mediana con los citostáticos convencionales alcanza unos 17-20 meses Combinación Agentes activos Supervivencia mediana (meses) 5-FU/LV 1 droga 11-12 Irinotecan/5-FU 2 drogas 14-15 Oxaliplatino/5-FU ± irinotecan 3 drogas 17-20 Meta-analysis Group in Cancer. J Clin Oncol. 1998;16:301-308. Saltz LB, et al. N Engl J Med 2000;343:905-914. de Gramont A, et al. J Clin Oncol. 2000;18:29382947. Goldberg RM, et al. J Clin Oncol. 2002;20:4591-4596. Tournigand C, et al. J Clin Oncol. 2004;22:229-237. Page 30 www.clinicaloptions.com Quimioterapia en mCRC La combinación de citostáticos incrementa la supervivencia Comentarios Inhibidores TS Inhibidores TS Fluoruracilo (IV) Fluoruracilo (IV) Capecitabina (PO) Capecitabina (PO) Inhibidores Topo-I Alquilantes Irinotecán TS: Timidilato sintestasa; Topo-I: Topoisomerasa I Page 31 Oxaliplatino 4 La supervivencia mediana con la exposición a los 3 agentes es de aproximadamente 20 meses. Grothey A, et al J Clin Oncol. 2005;23:94419442. Mecanismos de acción del Bevacizumab y los MOAs anti EGFR VEGF (Bevacizumab) Bevacizumab Mab Recombinante humanizedo anti VEGF Neutraliza todas las isoformas de VEGF A T1/2 17-21 días Page 34TM Avastin (bevacizumab) [package insert]. San Francisco, Calif: Genentech, Inc; 2004. Bevacizumab (Avastin®): Mecanismo de Acción Bevacizumab VEGF P P Page 35 P P Bevacizumab (Avastin®): Mecanismo de Acción Bevacizumab VEGF P P P P BLOQUEO de la activación del VEGFR Page 36 EGFR (Cetuximab, Panitumumab) Cetuximab IgG1 (anticuerpo quimérico) Anti EGFR (y sus heterodímeros) Aprobado en 2004 en mCRC Page 38 Courtesy of: Paulo Hoff MAb Anti-EGFR Extracelular Intracelular Shc Grb2 PI3-K AKT Sos-1 Ras MEKK-1 Page 39 Raf MOAs Anti-EGFR Extracelular Intracelular Shc Grb2 PI3-K Sos-1 mK-Ras AKT MEKK-1 Raf MEK Page 40 www.clinicaloptions.com mTOR MKK-7 Targeting the EGFR pathway TGF-α extracellular R intracellular R Grb2 K K Shc mutation loss Grb2 PI3K Sos Ras Akt PTEN mTOR phosphorylation Sos FKHR GSK–3 Raf Bad p27 mutation mutation MEK1/2 MAPK Cyclin D1, E Cell cycle progression Page 41 Survival Proliferation Mendelsohn et al. JCO 2003 Evolución histórica del tratamiento mCRC – 2: Terapia molecular dirigida Bevacizumab en mCRC – Primera línea Phase III Trial With Bevacizumab Therapy in First-Line MCRC Untreated MCRC R A N D O M I Z E Bolus IFL + placebo (n = 412) Bolus IFL + BV (n = 403) 5-FU/LV + BV (n = 110): Closed due to lack of efficacy Hurwitz. NEJM, 2004 Page 44 Courtesy of: Paulo Hoff Phase III Trial of Bevacizumab in First-Line mCRC IFL + Placebo (n=411) IFL + Bevacizumab (n=402) P Value 0.0036 ORR (%) 35 45 CR 2.2 3.7 PR 32.5 41.2 Hurwitz H et al. N Engl J Med 2004;350:2235–42 Page 45 Courtesy of: Paulo Hoff Probability of being progression-free Phase III Trial : PFS Median PFS (months) IFL + placebo: 6.2 (95% CI: 5.6–7.7) IFL + bevacizumab: 10.6 (95% CI: 9.0–1.0) HR=0.54 (95% CI: 0.45–0.66) p<0.001 1.0 0.8 0.6 IFL + bevacizumab 0.4 IFL + placebo 0.2 6.2 0 0 10.6 10 20 30 PFS (months) Hurwitz H et al. N Engl J Med 2004;350:2335–42 Page 46 Courtesy of: Paulo Hoff Phase III Trial: Survival Median survival (months) IFL + placebo: 15.6 (95% CI: 14.3–17.0) vs IFL + bevacizumab: 20.3 (95% CI: 18.5–24.2) HR=0.66 (95% CI: 0.54–0.81) p<0.001 Probability of survival 1.0 0.8 0.6 IFL + bevacizumab IFL + placebo 0.4 0.2 15.6 0 0 10 20.3 20 Survival (months) 30 40 Hurwitz H et al. N Engl J Med 2004;350:2335–42 Page 47 Courtesy of: Paulo Hoff Trial of Bevacizumab plus FOLFIRI/mIFL (BICC-C): design R n=430 Initial design Amended design FOLFIRI (n=144) FOLFIRI+Bev. (n=60) mIFL (n=141) XELIRI (n=145) R n=117 Feb 2003 – April 2004 Primary endpoint: PFS mIFL+Bev. (n=57) May 2004 – Dec 2004 Protocol amended due to approval of bevacizumab * Celecoxib data not shown Fuchs et al, JCO 2008 Page 48 Courtesy of: Paulo Hoff Proportion of Subjects Who Survived Overall Survival Regimen Median OS (months) 1 Year P Value 1 FOLFIRI+ BEV 28 87% -- 0.9 mIFL + BEV 19.2 61% 0.01 0.8 0.7 0.6 0.5 0.4 0.3 0.2 FOLFIRI + Bevacizumab 0.1 mIFL + Bevacizumab 0 0 Fuchs et al. JCO 2008 Page 49 10 20 30 40 Survival Time (months) Courtesy of: Paulo Hoff Phase III Trial of Bevacizumab With Oxaliplatin-Based Therapy in CRC + Bevacizumab (7.5 mg/kg, q3w) XELOX + Placebo Previously untreated MCRC Primary end point: TTP + Bevacizumab (5 mg/kg, q2w) FOLFOX4 + Placebo Saltz L, et al. JCO 2008 Page 50 Courtesy of: Paulo Hoff Progression-free Survival 1.0 HR = 0.83 [97.5% CI 0.72–0.95] (ITT) p = 0.0023 PFS estimate 0.8 0.6 0.4 0.2 8.0 9.4 0 0 25 5 15 20 FOLFOX+placebo/XELOX+placebo N=701; 547 events FOLFOX+bevacizumab/XELOX+bevacizumab N=699; 513 events Saltz L, et al. JCO 2008 Page 51 10 Months Courtesy of: Paulo Hoff Efficacy XELOX/FOLFOX N=701 XELOX/FOLFOX + bev 49% 47% 0.99 PFS (mos) 8.0 9.4 0.0023 OS (mos) 19.9 21.3 0.076 Response rate (%) Saltz L, et al. JCO 2008 Page 52 P-value N=699 Courtesy of: Paulo Hoff Patients should remain ‘on treatment’* to achieve optimal clinical benefit with bevacizumab 6 months 1.0 FOLFOX4/XELOX + bevacizumab Estimated probability FOLFOX4/XELOX + placebo 0.8 0.6 On treatment: HR=0.63 (PFS 10.4 vs 7.9 months, p<0.0001) 0.4 General: HR=0.83 (PFS 9.4 vs 8.0 months, p=0.0023) 0.2 0 0 5 10 PFS (months) 15 20 *Prespecified secondary analysis Page 53 Saltz, et al. ASCO 2007 (poster) Phase III Trial of Bevacizumab + Panitumumab-CT With Bev-CT in CRC (PACCE) Bev + Pan Ox-CT Bev Previously untreated MCRC Bev + Pan Iri-CT Bev Hecht JR, et al. JCO 2008 Page 54 Primary end point: PFS Phase III Trial of Bevacizumab + Panitumumab-CT With Bev-CT in CRC (PACCE) Bev + Pan Ox-CT Bev Previously untreated MCRC Bev + Pan Iri-CT Bev Hecht JR, et al. JCO 2008 Page 55 Primary end point: PFS Phase III Trial of Bevacizumab + Panitumumab-CT With Bev-CT in CRC (PACCE) Hecht JR, et al. JCO 2008 Page 56 Phase III Trial of Bevacizumab + Panitumumab-CT With Bev-CT in CRC (PACCE) Hecht JR, et al. JCO 2008 Page 57 Phase IV BRiTE Therapy in First-Line MCRC Untreated MCRC Page 58 E N R O L L Bev + CT Grothey, et al. JCO 2008 Phase IV BRiTE Therapy in First-Line MCRC PFS FOLFOX + Bev: 10 m (n=1092) Untreated MCRC E N R O L L Bev + CT PFS FOLFIRI + Bev: 10.4 m (n=280) Page 59 Grothey, et al. JCO 2008 BRiTE:* continuation of bevacizumab post-first progression significantly increases OS (time from initiation of first-line treatment to death) Post-progression therapy Estimated probability 1.0 Bevacizumab post-PD (n=642) No bevacizumab post-PD (n=531) No treatment (n=253) 0.8 0.6 0.4 Post-progression bevacizumab HR=0.48 (95% CI: 0.41–0.57) p<0.001 0.2 12.6 0 Page 60 0 5 10 *Non-randomised, observational trial 19.9 15 20 OS (months) 31.8 25 30 35 Grothey, et al. ASCO 2007 (poster) Grothey, et al. JCO 2008 BRiTE:* continuation of bevacizumab post-first progression significantly increases survival beyond progression, irrespective of subgroup factors Subgroup Age at disease progression <65 years ≥65 years Race White Black Other Baseline ECOG PS 0 1 ≥2 Site of primary tumour Colon Rectum First-line chemotherapy regimen FOLFOX FOLFIRI Other Exposed to EGFR inhibitors No Yes Exposed to all three active chemotherapy agents No Yes Time to first progression <6 months ≥ 6 months Best first-line response Complete response/partial response SD/PD All patients Page 61 HR 95% CI 0.47 0.51 0.37–0.60 0.40–0.65 0.51 0.32 0.48 0.42–0.62 0.18–0.57 0.21–1.08 0.53 0.45 0.37 0.40–0.71 0.35–0.59 0.18–0.65 0.49 0.49 0.40–0.59 0.32–0.75 0.47 0.38 0.62 0.37–0.59 0.24–0.59 0.46–0.85 0.52 0.42 0.41–0.66 0.32–0.54 0.51 0.42 0.39–0.68 0.33–0.52 0.48 0.52 0.37–0.62 0.41–0.65 0.44 0.50 0.49 0.33–0.59 0.41–0.63 0.41–0.58 Favours bevacizumab 0 *Non-randomised, observational trial 0.5 Favours CTx 1 Grothey, et al. JCO 2008 Phase II–IV clinical trials PFS benefits of bevacizumab with irinotecanbased therapy confirmed in daily practice FOLFIRI alone1 (n=109) Bevacizumab + FOLFIRI (BICC-C)2 (n=209) Bevacizumab + FOLFIRI (PACCE)3 (n=115) Bevacizumab + FOLFIRI (AVIRI)4 (n=209) Daily practice* Bevacizumab + FOLFIRI (MD Anderson)5 11.2 11.7 11.1 12.5 (n=120) Bevacizumab + FOLFIRI (BRiTE)7 (n=280) Bevacizumab + FOLFIRI (BEAT)8 (n=503) 0 Page 62 10 months (n=43) Bevacizumab + XELIRI (AIO 0604)6 *Large prospective, observational trials 8.5 2 12.1 10.9 11.6 4 6 8 10 Median PFS (months) 12 14 1. Tournigand, et al. JCO 2004; 2. Fuchs, et al. JCO 2007; 3. Hecht, et al. JCO 2009 4. Ackland, et al. ASCO GI 2008; 5. Kopetz, et al. ASCO 2007; 6. Reinacher-Schick, et al. ASCO 2008; 7. Grothey, et al. JCO 2008; 8. Van Cutsem, et al. ESMO 2008 PFS benefits of bevacizumab with oxaliplatinbased therapy confirmed in daily practice Daily practice‡ Phase II/III clinical trials XELOX/FOLFOX4 alone (NO16966)1 (n=699) Bevacizumab + XELOX/FOLFOX4 (NO16966)1 Bevacizumab + XELOX/FOLFOX4 ‘on treatment’* (NO16966)1 (n=699) (n=410) Bevacizumab + XELOX (AIO 0604)3 (n=127) Bevacizumab + FOLFOX (BRiTE)4 10.4 11.1 10.4 (n=1,092) 10.0 Bevacizumab + FOLFOX (BEAT)5 (n=552) 11.3 Bevacizumab + XELOX (BRiTE)4 (n=94) 11.2 Bevacizumab + XELOX (BEAT)5 (n=346) 0 *Secondary endpoint ‡Large prospective, observational trials Page 63 9.4 (n=699) Bevacizumab + oxaliplatin (PACCE)2 10 months 8.0 10.8 2 4 6 8 Median PFS (months) 10 12 1. Saltz, et al. JCO 2008; 2. Hecht, et al. JCO 2009 3. Reinacher-Schick, et al. ASCO 2008 (poster); 4. Grothey, et al. JCO 2008 5. Van Cutsem, et al. ESMO 2008 (poster) MACRO: Maintenance Bev vs Continued Bev + XELOX in Patients With mCRC Patients with previously untreated mCRC (N = 480) Induction Therapy XELOX + Bevacizumab 6 cycles XELOX + Bevacizumab (n = 239) Bevacizumab (n = 241) Maintenance cycles administered q3w: Oxaliplatin 130 mg/m2 IV on Day 1 Capecitabine 1000 mg/m2 BID PO on Days 1-14 Bevacizumab 7.5 mg/kg IV on Day 1 Page 64 Tabernero J, et al. ASCO 2010. Abstract 3501. Disease progression, severe toxicity, or consent withdrawal MACRO: Duration of PFS Comparable Between Bev vs XELOX + Bev No significant difference between treatment arms in any efficacy outcome Noninferiority of bevacizumab vs XELOX + bevacizumab cannot be confirmed – The median PFS HR 95% CI (0.89-1.37) beyond the planned noninferiority limit of 1.32 Outcome Bevacizumab (n = 241) XELOX/ Bevacizumab (n = 239) HR (95% CI) OR (95% CI) Median PFS,* mos 9.7 10.4 1.11 (0.89-1.37) -- Median OS,* mos 21.7 23.4 1.04 (0.81-1.32) -- 49 46 -- 0.89 (0.62-1.27) Confirmed objective response, % *Median follow-up: 20.4-21.1 mos. Page 65 Tabernero J, et al. ASCO 2010. Abstract 3501. MACRO: Conclusions After bevacizumab + XELOX induction therapy for patients with mCRC, maintenance bevacizumab comparable to continued bevacizumab + XELOX – No significant difference in any efficacy outcome between arms Single-agent bevacizumab may be a feasible option for patients receiving bevacizumab + XELOX as induction therapy Page 66 Tabernero J, et al. ASCO 2010. Abstract 3501. Bevacizumab: only biological proven to extend both PFS and OS in first- and second-line Estimated probability 0.8 IFL + bevacizumab IFL + placebo 0.6 0.4 0.2 6.2 0 10.6 0 0.6 0.2 15.6 0.2 4.7 10 10 20 PFS (months) FOLFOX4 + bevacizumab FOLFOX4 HR=0.75 (p=0.0011) 0.8 0.6 0.4 0.2 20.3 20 30 OS (months) 7.3 0 10.8 0 0 Page 67 0.4 1.0 0.4 0 FOLFOX + bevacizumab FOLFOX 0.6 30 IFL + bevacizumab IFL + placebo HR=0.66 (p<0.001) 0.8 Second-line2 0.8 0 10 20 PFS (months) 1.0 Estimated probability 1.0 First-line1 Estimated probability Estimated probability 1.0 40 0 12.9 12 24 OS (months) 36 1. Hurwitz, et al. NEJM 2004; 2. Giantonio, et al. JCO 2007 Bevacizumab + FU in 1st Line mCRC mCRC with at least one of: 65≤ age, or PS 1-2, 3.5≤Albumin, or Previous abdominopelvic RT FU/LV (Weekly) (n=105) R Main end point: OS Secondary end points PFS RR QoL Page 68 Kabbinavar FF. J Clin Oncol 23:3697-3705 FU/LV + Bevacizumab (5 mg/kg/q2w) (n=104) Page 69 Kabbinavar FF. J Clin Oncol 23:3697-3705 Page 70 Kabbinavar FF. J Clin Oncol 23:3697-3705 Bevacizumab improves survival without impacting on health-related QoL First comparisons of QoL with the addition of bevacizumab to chemotherapy – study 2107 • IFL + placebo (n=411) • IFL + bevacizumab (n=402) – study 2192 • 5-FU/LV + placebo (n=105) • 5-FU/LV + bevacizumab (n=104) Assessed CCS score, TOI-C, FACT-C Addition of bevacizumab does not add to the treatment burden of chemotherapy Page 71 CCS = colorectal cancer subscale Kabbinavar, et al. Oncologist 2008 Role of Bevacizumab in curable mCRC Phase II trial: XELOX + bevacizumab – 54 patients with potentially resectable liver metastases – 6 cycles of neoadjuvant therapy (1 week on, 1 week off) – Clinical response: 74% – pCR: 11% Gruenberger B, et al. ASCO 2007. Abstract 4060. Page 72 Bevacizumab in ‘borderline’ resectable mCRC: OS in resected patients 100% 1.0 94.4% Estimated probability 0.8 0.6 0.4 0.2 0 0 40 Page 73 63.6% Response n (%) Complete pathological response 5 (9) Partial response 36 (64) Stable disease 12 (21) 20 OS (months) Gruenberger, et al. ASCO 2008 (poster) Chemotherapy-induced sinusoidal injury reduced with addition of bevacizumab in mCRC p=0.002 100 p=0.001 Incidence of sinusoidal injury (%) 80 p=0.212 60 40 20 p=0.086 0 36/79 (46%) 1–8 cycles 22/38 (58%) ≥9 cycles FOLFOX Page 74 4/78 (6%) 1–8 cycles 4/24 (17%) ≥9 cycles FOLFOX + bevacizumab Zorzi, et al. ASCO GI 2009 Impact of bevacizumab on OS in mCRC: a population-based study Patients with mCRC (n=1,417): 2003–2004 (pre-bevacizumab) versus 2006 (post-bevacizumab) Proportion of patients receiving Irinotecan or oxaliplatin and 5-FU: no change (p=0.68) Anti-EGFR therapy: no change (p=0.63) Bevacizumab therapy: increased 5.9% vs 30.6% (p<0.001) Addition of bevacizumab to systemic chemotherapy significantly improved OS: 23.6 vs 18.6 months (p<0.001) Page 75 Renouf, et al. ASCO GI 2009 Impact of bevacizumab in mCRC: significantly improved OS Estimated probability 1.0 0.8 Bevacizumab era (2006) 30.6% received bevacizumab 0.6 0.4 Pre-bevacizumab (2003–2004) p<0.001 5.9% received bevacizumab Bevacizumab + standard chemotherapy significantly improved OS: 23.6 vs 18.6 months (p<0.001) 0.2 0 0 Page 76 6 12 18 OS (months) Bevacizumab era (2006), n=448 Pre-bevacizumab (2003–2004), n=969 24 30 Renouf, et al. ASCO GI 2009 Cetuximab en mCRC Cetuximab versus BSC Metastatic colorectal cancer with prior 5-FU, irinotecan and oxaliplatin (572 pts) R A N D O M I Z E Cetuximab + BSC (287) BSC (285) Jonker et al. NEJM 2007; 357: 2040 Page 78 Courtesy of: Paulo Hoff Cetuximab versus BSC BSC Cetuximab P value (285) (287) RR 0% 8% P<0.001 PFS 1.8 months 1.9 months HR = 0.68 P<0.001 OS Page 79 4.6 months Jonker et al NEJM 2007; 357: 2040 6.1 months P=0.005 Courtesy of: Paulo Hoff EPIC: Cetuximab + Irinotecan after Fluoropyrimidine + Oxaliplatin failure Cetuximab 400 mg/m2 initial dose mCRC with progression after 1st line fluoropyirimidine and Oxaliplatin (n=1298) cycle 1, wk 1, 250 mg/m2 weekly Irinotecan 350 mg/m2 (n=648) R Primary endpoint: Overall survival Page 80 Sobrero AF. J Clin Oncol. 26: 2311-2319, 2008 Irinotecan (n=650) Cetuximab + Irinotecan vs Irinotecan in 2nd line - EPIC Page 81 Cet + Iri Iri (n=648) (n=650) RR 16.4% 4.2% P<0.05 PFS 4 months 2.6 months P<0.005 OS 10.7 m 10 m P=0.71 Sobrero AF. J Clin Oncol. 26: 2311-2319, 2008 P value CRYSTAL: Cetuximab in First Line mCRC Cetuximab 400 mg/m2 initial dose cycle 1, wk 1, 250 mg/m2 weekly Irinotecan 180 mg/m2 5-FU mg/m2 bolus +2400 mg/m2 CI LV every 2 weeks EGFR-expressing mCRC R Irinotecan 180 mg/m2 5-FU mg/m2 bolus + 2400 mg/m2 40-h CI LV every 2 weeks Stratification: • Regions • ECOG PS Randomized patients: 1217 Page 82 Van Cutsem E, et al. NEJM 2009 Courtesy of: Paulo Hoff CRYSTAL Trial: Primary Endpoint PFS 1.0 Cetuximab + FOLFIRI, n=599 0.9 FOLFIRI, n=599 0.8 HR = 0.851; 95% CI = [0.726-0.998] PFS estimate 0.7 Stratified log-rank p-value = 0.0479 0.6 8.9 mo 0.5 1-year PFS rate 23% vs 34% 8.0 mo 0.4 0.3 0.2 0.1 0.0 0 2 4 6 8 10 12 14 16 18 20 Progression-free survival time (months) Page 83 Van Cutsem E, et al. NEJM 2009 Courtesy of: Paulo Hoff Correlation of Skin Toxicity and Efficacy with Cetuximab in the CRYSTAL Study (1st Line) CRYSTAL combination arm: Cetuximab + FOLFIRI (n=599) 1.00 Skin reaction grade 3*, n=112 (18.7%) Skin reaction grade 2, n=243 (41%) Skin reaction grade 0 or 1, n=244 (41%) PFS estimate 0.75 *There were no grade 4 skin reactions 11.3 mo 9.4 mo 5.4 mo 0.50 0.25 0.00 0.0 *PFS Page 84= 2.5 progression-free survival Van Cutsem et al. Proc ASCO 2007 5.0 7.5 10.0 Time (months) 12.5 15.0 17.5 20.0 Courtesy of: J Tabernero Evolución histórica del tratamiento mCRC – 3: Terapia individualizada Impacto de las alteraciones en las vías de trasnducción de señales del EGFR en la eficacia de Cetuximab OPUS: FOLFOX4 + Erbitux Cetuximab 400 mg/m2 initial dose cycle 1, wk 1, 250 mg/m2 weekly Oxaliplatin 85 mg/m2 5-FU/FA every 2 weeks EGFR-detectable mCRC R Skin rash 0/1 FOLFOX4 Oxaliplatin 85 mg/m2 5-FU/FA every 2 weeks Primary endpoint: Overall response rate Stratification: • ECOG PS 0/1, 2 Randomized patients: 337 Page 87 Bokemeyer, et al. ASCO 2008 Courtesy of: Paulo Hoff Relating KRAS Status to Efficacy PFS & Response – KRAS Wild-type KRAS wild-type: HR=0.57; p=0.016 mPFS Cetuximab + FOLFOX: 7.7 months mPFS FOLFOX: 7.2 months 70 Cetuximab + FOLFOX FOLFOX 60 0.9 0.8 Response rate (%) Progression-free survival 1.0 p=0.011 Odds ratio=2.544 (95% CI: 1.238–5.227) 0.7 0.6 0.5 0.4 0.3 61 50 40 30 37 20 0.2 10 0.1 0.0 0 Page 88 2 4 6 Months Bokemeyer C, et al. J Clin Oncol 2008 8 10 12 0 FOLFOX Cetuximab + FOLFOX Courtesy of: Paulo Hoff MOAs Anti-EGFR Extracelular Intracelular Shc Grb2 PI3-K Sos-1 mK-Ras AKT MEKK-1 Raf MEK Page 89 www.clinicaloptions.com mTOR MKK-7 CRYSTAL: Summary of Efficacy Data in KRAS wt Pre-2009 ESMO Post-2009 ESMO KRAS wt KRAS wt FOLFIRI 43 p-value mPFS (Months) FOLFIRI 540 (45%) KRAS Analysis (%) ORR (%) Cetuximab +FOLFIRI 1063 (89%) 59 39.7 0.0025 8.7 Cetuximab +FOLFIRI 57.3 < 0.0001 9.9 8.4 9.9 HR 0.68 0.70 p-value 0.017 0.0012 OS (Months) P-value Page 90 21.0 24.9 0.22 20.0 23.5 0.0094 Courtesy of: Paulo Hoff NCIC CTG C0.17: Overall Survival in K-ras Wild-Type Patients 1 Proportion Alive 0.8 Study arm MS (months) 95% CI Cetuximab + BSC 9.5 7.7 – 10.3 BSC alone 4.8 4.2 – 5.5 0.6 HR 0.55 95% CI (0.41,0.74) Log rank p-value: <0.0001 0.4 0.2 Cetuximab BSC 0 0 Cetuximab 117 113 BSC Page 91 2 108 92 4 95 69 6 8 10 12 14 Time from Randomization (Months) 81 36 Karapetis C et al, New Engl J Med 2008 52 24 34 17 20 12 9 5 16 18 6 3 2 3 Courtesy of: Paulo Hoff Phase III MRC COIN Untreated MCRC Page 92 R A N D O M I Z E XELOX/OxMdG (n = 815) XELOX/OxMdG + Cetuximab (n = 815) XELOX/OxMdG + Cetuximab (n = 815) Intermitent ESMO, 2009 COIN: K-ras WT OS Survival probability Arm A (XELOX/FOLFOX) Arm B (XELOX/FOLFOX + cetuximab) 1.00 0.75 Arm A Arm B Diff. Median OS, months 17.9 17.0 –0.92 2-year survival, % 36.1 34.4 -1.66 0.50 HR point estimate = 1.038 95% CI 0.90–1.20 p=0.68 0.25 0 0 No. at risk Arm A 367 362 Arm B 6 12 18 24 30 Time (months) 36 42 316 306 250 238 154 149 19 17 1 3 83 80 44 42 Page 93 ITT analysis Maughan, et al. ECCO-ESMO 2009 (abstract No. 6LBA) COIN: K-ras WT PFS Arm A (XELOX/FOLFOX) Arm B (XELOX/FOLFOX + cetuximab) Survival probability 1.00 0.75 Median PFS, months 0.50 Arm A Arm B Diff. 8.6 8.6 +0.07 HR point estimate = 0.959 95% CI 0.84–1.09 p=0.60 0.25 0 No. at risk Arm A Arm B 0 6 12 18 24 30 36 367 361 245 249 92 103 41 42 18 22 11 9 6 6 42 1 0 Page 94 ITT analysis Maughan, et al. ECCO-ESMO 2009 (abstract No. 6LBA) COIN: No Significant Difference in OS, PFS Between Treatment Arms, Pt Subsets Survival Outcome, Mos Cetuximab + Chemotherapy Chemotherapy HR (95% CI) P Value Median OS 17.0 17.9 1.038 (0.90-1.20) .68 Median PFS 8.6 8.6 0.959 (0.84-1.09) .60 Median OS 19.9 20.1 1.019 (0.86-1.20) .86 Median PFS 9.2 8.8 0.922 (0.80-1.07) .36 Median OS 12.7 14.4 1.004 (0.87-1.15) .96 Median PFS 6.3 6.6 1.079 (0.95-1.23) .33 Wild-type KRAS All wild-type patients Patients with mutated KRAS, NRAS, or BRAF Page 95 Maughan TS, et al. ASCO 2010. Abstract 3502. ITT Survival: WT K-Ras (n=729) XELOX/OxMdG OS 17,9 XELOX/OxMdG + HR Cetuximab (p value) 17,0 1,038 (months) 2y OS (%) 36,1 34,4 PFS 8,6 8,6 (months) Page 96 (0,68) 0,95 (0,60) ESMO, 2009 COIN: K-RAS and Response All patients K-ras WT K-ras MT Cetuximab Cetuximab Cetuximab FOLFOX/ FOLFOX/ FOLFOX/ + FOLFOX/ + FOLFOX/ + FOLFOX/ XELOX XELOX XELOX XELOX XELOX XELOX (n=815) (n=367) (n=268) (n=815) (n=362) (n=297) Best overall response (%) 51 Odds ratio 1.08 (p=0.428) Page 97 53 57 64 OR=1.35 (p=0.049) 46 43 OR=0.88 (p=0.449) Maughan, et al. ECCO-ESMO 2009 (abstract No. 6LBA) NORDIC VII: Cetuximab in First Line mCRC Nordic FLOX (FU 500 mg/m2 + LV 60 mg/m2, d1,2 Q2W) mCRC R Nordic FLOX + Cetuximab Nordic FLOX stop & go + Cetuximab Endpoint: • PFS Randomized patients: 571 Page 98 Tveit KM, ESMO 2010 NORDIC VII: Cetuximab in First Line mCRC Nordic FLOX (FU 500 mg/m2 + LV 60 mg/m2, d1,2 Q2W) mCRC R Nordic FLOX + Cetuximab Nordic FLOX stop & go + Cetuximab Outcome FLOX F+Cet Stop&Go-Cet PFS 7.9 8.3 7.3 RR 41% 49% 47% OS 20.4 19.7 20.3 Endpoint: • PFS Randomized patients: 571 Page 99 Tveit KM, ESMO 2010 TRIALS IN mCRC 1st Line treatment K-Ras status WT TRIAL CRYSTAL OPUS COIN NORDIC Page 100 PH PFS FOLFIRI FOLFIRI+ CETUXIMAB P FOLFIRI FOLFIRI + CETUXIMAB P 8.4 9.9 0.0017 20 23.5 0.0094 FOLFOX FOLFOX + CETUXIMAB P FOLFOX FOLFOX + CETUXIMAB P 7.2 8.3 0.006 18.5 22.8 0.3854 XELOX/ FOLFOX XELOX/FOLFOX +CETUXIMAB P XELOX/ FOLFOX XELOX/FOLFOX + CETUXIMAB P 8.6 8.6 0.6 17.9 17 0.68 FLOX FLOX + CETUXIMAB P FLOX FLOX + CETUXIMAB P 7.9 8.3 0.3 20.4 19.7 0.30 3 2 3 OS 3 NCCTG0147: Adjuvant FOLFOX +/- Cetuximab mFOLFOX6 q2w x12 CRC stage III R mFOLFOX6 q2w x12 + Cetuximab Endpoint: • DFS@3y Randomized patients: 2581 Page 101 FOLFOX FOLFOX-Cet Total Wt KRAS 909 955 1864 Mt KRAS 374 343 717 Total 1283 1298 2581 Goldberg RM, ASCO 2010 NCCTG0147: Adjuvant FOLFOX +/- Cetuximab mFOLFOX6 q2w x12 R CRC stage III Endpoint: • DFS@3y Randomized patients: 2581 mFOLFOX6 q2w x12 + Cetuximab Outcome FOLFOX – wt-KRAS FOLFOX+Cet – wt-KRAS FOLFOX – mut-KRAS FOLFOX+Cet mut-KRAS DFS@3y 76% 72% 67% 64% OS 88% 84% 88% 80% Page 102 Goldberg RM, ASCO 2010 Targeting the EGFR pathway TGF-α extracellular R intracellular R Grb2 K K Shc mutation loss Grb2 PI3K Sos Ras Akt PTEN mTOR phosphorylation Sos FKHR GSK–3 Raf Bad p27 mutation mutation MEK1/2 MAPK Cyclin D1, E Cell cycle progression Page 103 Survival Proliferation Mendelsohn et al. JCO 2003 Incidence of genetic alterations in CRC Molecular finding K-RAS mutation Loss of PTEN Epiregulin BRAF mutation PI3K EGFR non-amplified Page 104 % of Incidence 30 – 50% 19% ? 3 – 10% 13% 11 – 25% Loupakis F et al. J Clin Oncol. 2009 Jun 1;27(16):2622-9 Laurent-Puig P, et al. J Clin Oncol 2009 doi: 10.1200/ JCO.2009.22.4295 Perrone F, et al. Ann Oncol. 2009 Jan;20(1):84-90 Goldstein NS, et al. Cancer 2001;92:1331-1346 CRYSTAL: BRAF mutations and PFS for cetuximab PFS according to BRAF status in retrospective CRYSTAL substudy Page 105 Köhne et al. ASCO 09. Abstract 4068 BRAF mutations and response to cetuximab in K-RAS wild type Page 106 Laurent-Puig P, et al. J Clin Oncol 2009 doi: 10.1200/ JCO.2009.22.4295 – Patients with wild-type KRAS have better prognosis vs mutated KRAS – Patients with mutated BRAF have the poorest prognosis Maughan TS, et al. ASCO 2010. Abstract 3502. Page 107 12 Chemotherapy Chemotherapy + Cetuximab 6 0 18 Median OS (Mos) Strong OS prognostic effect of KRAS, NRAS, and BRAF mutation status evident regardless of cetuximab use Median PFS (Mos) COIN: Prognostic Effect of Mutational Status 12 6 0 n= 57 268 367 340 815 289 45 297 362 366 815 292 Mutation Status BRAF mutation Any mutation All patients KRAS wild type KRAS mutation All wild type Many patients will not respond to treatment with EGFR inhibitors due to KRAS and BRAF mutations mCRC patients treated with panitumumab or cetuximab (n=114) KRAS mutational status (evaluable patients n=113) Responders Non-responders Mutant KRAS 34/113 (30%) Wild-type KRAS 79/113 (70%) 2/34 (6)* 22/79 (28)* 32/34 (94)* 57/79 (72)* BRAF mutational status on wild-type KRAS tumours (n=79) Responders Non-responders Mutant BRAF 11/79 (14%) Wild-type BRAF 68/79 (86%) 0/11 (0)‡ 22/68 (32)‡ 11/11 (100)‡ 46/68 (68)‡ *p<0.05 (p=0.011); ‡p<0.05 (p=0.029) Page 108 Di Nicolantionio, et al. JCO 2008 Loss of PTEN and response to cetuximab in K-RAS wild type Page 109 Laurent-Puig P, et al. J Clin Oncol 2009 doi: 10.1200/ JCO.2009.22.4295 Loss of PTEN and response to cetuximab Responders (CR+PR+SD) (%) Non-responders (%) PTEN+ (n=33) PTEN– (n=22) 12 (36) 1 (5) 21 (64) 21 (95) Estimated probability 1.0 PTEN+ median PFS = 4.7 months PTEN– median PFS = 3.3 months 0.8 Log-rank test: p=0.005 HR=0.49; 95% CI: 0.20–0.75 0.6 0.4 0.2 0 0 2.5 5.0 7.5 10.0 12.5 15.0 PFS (months) Fisher’s Exact Test: p=0.008 Concordance primary tumour sample/metastasis: 27/45 (60%) Page 110 Loupakis, et al. JCO 2009 KRAS status and EGFR monoclonal antibodies in chemorefractory patients Non-responder: BRAF mutation 10% Responds to standard dose 22% KRAS wild-type Non-responder: loss of PTEN or PI3K mutation percentage unknown Non-responder: reason unknown percentage unknown Page 111 Responds to increased dose ~5% Non-responder: KRAS mutant 40% KRAS mutant Wong, Cunningham. JCO 2008 (Ausencia de) Impacto de las alteraciones en las vías de trasnducción de señales del EGFR en la eficacia de Bevacizumab AVF2107: OS by K-ras Status Group: Mutant (N=78) Group: Wild-Type (N=152) HR=0.69; P=0.26 HR=0.58; P=0.04 1.0 13.6 19.9 0.6 0.4 0.4 0.2 0.0 0.0 5 10 15 20 25 30 IFL + Placebo IFL + Avastin 0.6 0.2 0 Median OS (mo) 0.8 Proportion Surviving IFL + Placebo IFL + Avastin 0.8 Proportion Surviving 1.0 Median OS (mo) 0 Duration of Survival (months) Page 113 Ince et al. J Natl Cancer Inst. 2005;97:981. Hurwitz et al. GI World Congress. Abstract O-035 and poster. 5 10 15 20 25 Duration of Survival (months) 30 17.6 27.7 AVF2107: PFS by K-ras Status Group: Mutant (N=78) Group: Wild-Type (N=152) HR=0.41; P=0.0008 HR=0.44; P<0.0001 1.0 Median PFS (mo) 0.8 IFL + Placebo IFL + Avastin 5.5 9.3 0.6 0.4 0.2 Proportion progression-free Proportion progression-free 1.0 Median PFS (mo) 0.8 IFL + Placebo IFL + Avastin 7.4 13.5 0.6 0.4 0.2 0.0 0.0 0 5 10 15 20 25 Duration of Survival (months) 114 IncePage et al. J Natl Cancer Inst. 2005;97:981. Hurwitz et al. GI World Congress. Abstract O-035 and poster. 0 5 10 15 20 25 Duration of Survival (months) Core Slide AVF2107g: Response according to K-Ras status 70 IFL + Avastin Response rate (%) 60 60 IFL + placebo 50 40 43 37 41 30 20 10 0 K-Ras wild-type K-Ras mutant p=0.006 p=0.8 Hurwitz HI, et al. Oncologist 2009;14:22-8 Page 115 Bevacizumab improves patient outcome independent of KRAS or BRAF status Biomarker All subjects KRAS mutation status Mutant Wild-type BRAF mutation status Mutant Wild-type N 267 Placebo + IFL Median n (months) 120 17.45 Bev + IFL Median n (months) 147 26.35 HR 0.57 (95% CI) (0.39–0.85) 78 152 34 67 13.60 17.64 44 85 19.91 27.70 0.69 0.58 (0.37–1.31) (0.34–0.99) 10 217 3 97 7.95 17.45 7 120 15.93 26.35 0.11 0.53 (0.01–1.06) (0.34–0.82) KRAS and BRAF mutation status Mutant Wild-type 88 125 37 57 13.60 21.72 51 68 19.91 27.70 0.67 0.57 (0.37–1.20) (0.34–0.82) p53 mutation status Mutant Wild-type 139 66 63 31 21.72 16.36 76 35 27.70 NR 0.54 0.67 (0.30–0.95) (0.32–1.42) p53 overexpression Positive Negative 191 75 92 28 17.45 16.26 99 47 26.35 25.07 0.70 0.32 (0.45–1.10) (0.15–0.70) HR 0.2 0.5 1 2 5 Survival benefit also independent of p53, VEGF (plasma and tissue) and TSP-2 Page 116 Bev = bevacizumab Jubb, et al. JCO 2006; Ince, et al. JNCI 2005 Holden, et al. ASCO 2005 (Abstract 3555); Hurwitz, et al. Oncologist 2009 Avastin in K-RAS mutant patients IFL IFL + Avastin Folfiri Folfiri + Cetuximab Folfox Folfox + Cetuximab Xelox + Avastin Folfiri + Avastin Progression Free Survival Page 117 Avastin in K-RAS wild-type IFL IFL + Avastin Folfiri Folfiri + Cetuximab Folfox Folfox + Cetuximab Xelox + Avastin Folfiri + Avastin Progression Free Survival Page 118 Incidences of bevacizumab-associated adverse events were comparable for the two K-RAS subgroups Page 119 Hurwitz HI, et al. Oncologist 2009;14:22-8 TRIALS IN mCRC 1st Line treatment K-Ras status WT TRIAL CRYSTAL OPUS COIN PRIME AVF2107g Page 120 PH PFS FOLFIRI FOLFIRI+ CETUXIMAB P FOLFIRI FOLFIRI + CETUXIMAB P 8.4 9.9 0.0017 20 23.5 0.0094 FOLFOX FOLFOX + CETUXIMAB P FOLFOX FOLFOX + CETUXIMAB P 7.2 8.3 0.006 18.5 22.8 0.3854 XELOX/ FOLFOX XELOX/FOLFOX +CETUXIMAB P XELOX/ FOLFOX XELOX/FOLFOX + CETUXIMAB P 8.6 8.6 0.6 17.9 17 0.68 FOLFOX FOLFOX + PANITUMUMAB P FOLFOX FOLFOX + PANITUMUMAB P 8 9.6 0.023 19.7 23.9 0.072 IFL IFL + BEVACIZUMAB P IFL IFL + BEVACIZUMAB P 7.4 13.5 0.0001 17.6 27.7 0.04 3 2 3 OS 3 3 Conclusiones La adición de Bevacizumab a Quimioterapia en mCRC en primera línea mejora los desenlaces relevantes en forma CONSISTENTE – – – – – – – – – Quimioterapias basadas en oxaliplatino Quimioterapias basadas en irinotecán Quimioterapias basadas en fluoruracilo En pacientes con mutaciones del K-RAS, y sin ellas En pacientes con otras mutaciones de la cascada del EGFR Se ratifican en estudios observacionales prospectivos Se ratifican en estudios poblacionales Se debe continuar hasta progresión Hay evidencia no aleatorizada, pero impactante, del beneficio de continuarlo más allá de progresión – Exhibe buenas tasas de respuesta en pacientes marginalmente resecables – Parece mitigar el daño sinusoidal asociado a oxaliplatino Page 121 Conclusiones La toxicidad adicional asociada al Bevacizumab es manejable Los MOAs anti EGFR no son eficaces en pacientes con mutación del KRAS, y su uso en estos pacientes debe ser excluido de la práctica diaria. Los MOAs anti EGFR exhiben respuestas INCONSISTENTES en pacientes con KRAS nativo (en primera línea) Los MOAs anti EGFR son ineficaces en una fracción no determinable – y no despreciable - de pacientes con mCRC por razones biológicas (Mutaciones de BRAF, PTEN, etc) Los MOAs anti EGFR tienen un papel en pacientes en última línea de tratamiento (con KRAS nativo) El Bevacizumab y los MOAs anti EGFR no deben ser combinados Page 122 Bev o Cet en 1ª Línea- mCRC Estudio (año pub) N9741 (2008) Tipo Línea Brazo (n) F3 1ª FOLFOX / IFL RR (%) 45 / 31 PFS (m) OS (m) Comentarios 8.7 / 6.9 19.5 / FOLFOX mejor que IFL 14.5 Hurwitz (2004) F3 1ª Bev IFL / IFL 45 /35 10/6 20 / 16 Registro Bev en 1ª línea Kabbinavar (2005) RF2 1ª Bev FULV / FULV 21/18 17 / 13 Pacientes no candidatos a I u O Ackland (2008) D 1ª FOLFIRI + Bev 50 22 Giantonio (2005) RF2 2ª Fox / Bev + Fox 7.2 / 12.9 Registro Bev en 2ª línea NO16966 (2007) F3 1ª Fox / Bev + Fox 47 / 49 8 / 9.4 19.9 / Bev sólo durante Negativo. 21.3 PACCE (2009) F3 1ª Bev+Fox/PBev+Fo 48 / 46 11.4 / 24.5 / RR KRAS nativo Bev+Fox: 56% x 10 19.4 PACCE (2009) F3 1ª Bev+Fir/PBev+FIr 40 / 43 11.7/10. 20.5/20.7 1 BICC-C (2007) F3 1ª Bev+Fir/Bev+mIFL 58 / 56 11.2/8.3 >23/19.2 First BEAT OCS 1ª Bev + QT 10.2 22.7 – No US BRiTE OCS 1ª Bev + QT (>Fox) 10 25 1953 pts – US BRiTE OCS 1ª BBP / No-BBP 31.8/ 19.9 Cochrane MA 1ª Bev + QT / QT 9.7/7.1 20.5/17.7 HR 0.61 para PFS, 0.81 para OS CRYSTAL (2009) F3 1ª Cet + FIr / FIr 47 / 39 8.9/8 19.9/18.6 No discriminados por KRAS CRYSTAL (2009) AS 1ª Cet + FIr / FIr 59 / 43 9.9/8.7 24.9/21 KRAS nativo COIN (2009) F3 1ª Cet + Fox / FOx 51/53 8.6/8.6 17/17.9 KRAS nativo no predictivo Abreviaturas: RR: Tasa de respuestas (PR + CR); PFS: Supervivencia libre de progresión; OS: Supervivencia global; m: meses; F: Fase; RF: Fase aleatorizado; D: Descriptivo; OCS: Estudio de observación de cohorte, prospectivo; Fox: Fluoropirimidina + Oxaliplatino; Bev: Bevacizumab; PBev: Panitumumab – Bevacizumab; FIr: Folfiri; Cet: Cetuximab; QT: Quimioterapia; US: Estados Unidos; BBP: Bevacizumab luego de progresión – Bevacizumab beyond progression; HR: Hazard ratio; MA: Meta-análisis; AS: Análisis de subgrupo retrospectivo. Page 123 Efectos adversos de Bevacizumab y MOAs anti EGFR Toxicidad de clase de los Anti-VEGF (Bevacizumab) Hipertensión arterial Incremento de los LFT Fatiga Dolor en el sitio del tumor Coágulos Proteinuria Sangrado (Epistaxis, hemoptisis, tumoral) Hipotiroidismo? Cefalea Eventos neurológicos Page 125 Perforación intestinal Hypertension and Bevacizumab Meta-analysis of 7 trials: 1850 patients Bevacizumab was associated with hypertension in a dose dependent manner: – Low doses (3-7.5 mg/Kg): RR 3.0 (95% CI 2.2-4.2) – High doses (10-15 mg/Kg): RR 7.5 (95% CI 4.2-13.4) Incidence: – Low doses: all grades 2.7%-32%; grade 3: 8.7% – High doses: all grades 17.6-36%; grade 3: 16% – Placebo: grade 3: 1.7% Zhu X, et al. Am J Kidney Dis 2007; 49: 186-193 Page 126 Courtesy of: J Tabernero ATEs and Bevacizumab: Pooled Analysis of Five Randomized Trials Chemotherapy alone (n=782) Bevacizumab + chemotherapy (n=963) 13 (1.7) 37 (3.8) 419 673 3.1 (1.7–5.3) 5.5* (3.9–7.6) ATEs, n (%) Person-years of observation Rate/100 person-years (95% CI) Hazard ratio (95% CI) 1.99** (1.05–3.75) *p=0.076; **p=0.03 CI = confidence interval ATE = arterial thromboembolic event Page 127 Skillings Higher risk observed in patients with history of ATEs and aged ≥65 years, hypertension and proteinuria JR, et al. Proc ASCO 2005; 23: 3019 Scappaticci FA et al. J Natl Cancer Inst 2007;99:1232-9 Courtesy of: J Tabernero ATEs Incidence with Bevacizumab by Risk Factor and Aspirin Use Aspirin at baseline Risk factor Control % (n/N) All patients 2.0 (1/49) 7.6 (6/79) 1.6 (12/733) 3.5 (31/884) 0 (0/11) 5 (1/20) 1 (5/479) 1.7 (10/582) 5.3 (1/19) 10.7 (3/28) 2.5 (1/40) 18 (11/61) Age 65 years 0 (0/32) 9.1 (5/55) 2.8 (7/247) 6.7 (19/284) Age 65 years and history of ATEs 0 (0/13) 12.5 (3/24) 3 (1/33) 21 (9/43) Age <65 years and no history of ATEs History of ATEs Bevacizumab (n/N) No aspirin at baseline % Control % (n/N) Bevacizumab (n/N) % N = total number; n = subgroup Aspirin did not increase bleeding risk of any grade Grade 3/4 bleeding with and without aspirin: 3.6 versus 5.6% Page 128 Hambleton J, et al. Proc ASCO 2005; 23: 3554 Scappaticci FA et al. J Natl Cancer Inst 2007;99:1232-9 Courtesy of: J Tabernero Proteinuria and Bevacizumab Meta-analysis of 7 trials: 1850 patients Bevacizumab was associated with proteinuria in a dose dependent manner: – Low doses (3-7.5 mg/Kg): RR 1.4 (95% CI 1.1-1.7) – High doses (10-15 mg/Kg): RR 2.2 (95% CI 1.6-2.9) Incidence: – Low doses: all grades 21-41%; grade 3: 1.0% – High doses: all grades 22-63%; grade 3: 1.8% – Placebo: grade 3: 0.1% – Renal cell carcinoma patients: grade 3: 7.7% Page 129 Zhu X, et al. Am J Kidney Dis 2007; 49: 186-193 Courtesy of: J Tabernero Gastrointestinal perforations Bevacizumab: Metaanalysis: 12,294 patients, 17 RCTs Gastrointestinal perforation rate: 0.9% (95% CI 0.7-1.2) RR 2.14, p=.011, 95% CI 1.19-3.85 Relative risks: – Dose 5 vs 2.5 mg/Kg/week: RR 2.67 (95% CI 1.14-6.26) vs 1.61 (95% CI 0.76-3.38) – Tumor type: CRC RR 3.1 (95% CI 1.26-7.63) RCC RR 5.67 (95% CI 0.66-48.42) No robust data for VEGFR inhibitors and aflibercept Page 130 Hapani et al; Lancet Oncol 2009 Toxicidad de clase de los Anti-EGFR (Cetuximab) Exantema acneiforme (89%) Cefalea (26%), Astenia (48%) Diarrea (25%), Náuseas leves (29%) Constipación leve (26%) Cambios en las uñas y tejidos vecinos (14%) Dolor abdominal leve(26%) Hipomagnesemia Page 131 Skin Toxicity: Pathophysiology EGFR inhibitors1: – EGFR-inhibition driven: – Similar in all EGFR-inhibitors. – Cutaneous effects: dose-dependent: cetuximab (EVEREST), panitumumab, erlotinib – Polymorphisms in EGFR gene, intron 1 – EGFR null skin mice: similar lesions – Unique combination: itchy acneiform eruption, xerosis, paronychia, hair changes, telangiectasia – Mechanism unknown Page 132 Segaert S, et al. Ann Oncol 2006 Courtesy of: J Tabernero Cutaneous and Nail Toxicities Associated with Cetuximab Acne-like Rash Intensity Week 1 2 3 4 Only 14% of patients experience Grade 3 Acne-like rash 5 6 7 8 9 11 Fissures Dry skin Grade 3 Acne-like rash 10 12 Nail bed Images kindly provided by Prof. Segaert THERAPY SUGGESTIONS Topical anti-acne creams (drying effect) Page 133 Emollients Hydrocolloid dressing/’glue’ Antiseptic soaks or Silver nitrate +/- tetracyclines +/- antihistamines Courtesy of: J Tabernero Correlation of Skin Toxicity and Efficacy with Cetuximab in the BOND Study (Refractory) BOND combination arm: Cetuximab + Irinotecan (n=218) Maximum grade of skin reaction Number of patients Response (%) mTTP* (months) mOS** (months) 0 32 (14.7%) 6.3 1.4 3.0 1 58 (26.6%) 8.6 1.5 6.5 2 99 (45.4%) 27.3 4.2 10.3 3 29 (13.3%) 55.2 8.2 13.7 Skin reactions appear to be predictive for efficacy *mTTP = median time to progression ; **mOS = median overall survival Page 134 Cunningham D et al. N Engl J Med 2004; 351(4): 337-345. Courtesy of: J Tabernero Correlation of Skin Toxicity and Efficacy with Cetuximab in the CRYSTAL Study (1st Line) CRYSTAL combination arm: Cetuximab + FOLFIRI (n=599) 1.00 Skin reaction grade 3*, n=112 (18.7%) Skin reaction grade 2, n=243 (41%) Skin reaction grade 0 or 1, n=244 (41%) PFS estimate 0.75 *There were no grade 4 skin reactions 11.3 mo 9.4 mo 5.4 mo 0.50 0.25 0.00 0.0 *PFS = Page 135 2.5 progression-free survival Van Cutsem et al. Proc ASCO 2007 5.0 7.5 10.0 Time (months) 12.5 15.0 17.5 20.0 Courtesy of: J Tabernero Hypomagnesaemia Hypomagnesaemia Total Grade 3-4 Panitumumab1 36% 3% Cetuximab2 53% 15% Related to duration of treatment3: – Grade 3-4: 6% <3 m, 23% 3-6 m, 47% >6 m Treatment4: – Related symptoms: asthenia, irritability – Be cautious in case of: cardiomyopathy, renal failure, treatment with platin – Grade 1-2: oral or iv replacement – Grade 3-4: discontinuation and iv replacement, stop and go? Courtesy of: J Tabernero Page 136 1Van Cutsem et al. J Clin Oncol 2007;25:1658-1664 2Jonker DJ et al. N Engl J Med 2007;357:2040–8 3Fakih MG et al. Clin Colorectal Cancer 2006;6:152–6 4Izzedine H et al. Crit Rev Oncol/Hematol 2009 (Epub)