PayneWelcoming African-American Women into Your Breastfeeding
advertisement

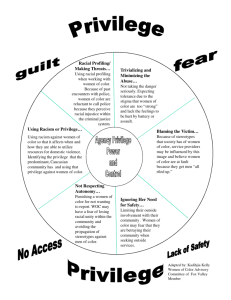
Lack of cultural congruent education Care provider bias in practice Inadequate social support Normalization of artificial feeding Insufficient clinical support Dominant culture framing Suboptimal maternity care practices and facilities Breastfeeding and infant mortality Increased infant morbidity Parental disempowerment and diminished roles Increased maternal morbidity Communities that don’t thrive To be racially prejudiced means to have an unfavorable or discriminatory attitude or belief towards someone else or another group of people primarily on the basis of skin color or ethnicity. http://ctb.ku.edu/en/table-of-contents/culture/culturalcompetence/reduce-prejudice-racism/main When racial prejudice is supported by institutions and laws, racism is present. Racism is prejudice codified by power and embedded in the key structures of society. http://ctb.ku.edu/en/table-of-contents/culture/cultural-competence/reduce-prejudice-racism/main They impede or prevent the object of racism from achieving his or her full potential as a human being. They impede or prevent the object of racism from making his or her fullest contribution to society. They impede or prevent the person or group engaging in racist actions from benefiting from the potential contributions of their victim, and, as a result, weaken the community as a whole. White privilege (or white skin privilege) is a set of societal privileges, existing in predominantly white societies, which benefit white people beyond what is commonly experienced by non-white people in the same social, political, or economic circumstances. Could racially embedded biases be impacting breastfeeding rates among women of color in your practice? (Black women won’t breastfeed…so I’ll use my limited time elsewhere.) Could there be structural barriers that unfairly target women of color in your organization? (Your breastfeeding support group is held during the day when those working outside the home cannot take advantage of them.) Dominant culture values and images are the only ones on display. (A recent seminar was held for clients on ‘attachment-style parenting.’) Culture is defined as the shared traditions, beliefs, customs, history, folklore, and institutions of a group of people. Culture is shared by people of the same ethnicity, language, nationality, or religion. It's a system of rules that are the base of what we are and affect how we express ourselves as part of a group and as individuals. http://ctb.ku.edu/en/table-of-contents/culture/cultural-competence/culturally-competentorganizations/main Just because we share a common linguistic language does not mean that communication is occurring. It helps to understand the meta-language of the culture. This can be more difficult to interpret. Cultural knowledge" means that you know about some cultural characteristics, history, values, beliefs, and behaviors of another ethnic or cultural group. •"Cultural awareness" is the next stage of understanding other groups -- being open to the idea of changing cultural attitudes. •"Cultural sensitivity" is knowing that differences exist between cultures, but not assigning values to the differences (better or worse, right or wrong). Clashes on this point can easily occur, especially if a custom or belief in question goes against the idea of multiculturalism. Internal conflict (intrapersonal, interpersonal, and organizational) is likely to occur at times over this issue. Conflict won't always be easy to manage, but it can be made easier if everyone is mindful of the organizational goals. •"Cultural competence" brings together the previous stages -- and adds operational effectiveness. A culturally competent organization has the capacity to bring into its system many different behaviors, attitudes, and policies and work effectively in crosscultural settings to produce better outcomes Does your environment reflect the women you serve or does it reflect you? Does your staff reflect the population you serve (at all levels of the organization?) What are your own internal biases? How are your biases reflected in your practice? How does my practice really look to the women it serves? How can I find out how they really feel when they come into my space? What can I do to change things if they don’t meet my client needs? How can I increase my own awareness to my blindspots? How do I begin to build bridges to all the women I serve? How does my practice create breastfeeding barriers for women of color? Communications that subtly exclude negate or nullify the thoughts, feelings or experiential reality of a person of color. Example: Saying everyone is welcome when everything about your practice and the way it is designed provides comfort and familiarity to normative culture women. Derald Wing Sue. Racial Microaggressions in Everyd Say Life: Race, Gender and Sexual Orientation (John Wiley & Sons, 2010) Verbal, nonverbal, and environmental communications that subtly convey rudeness and insensitivity that demean a person's racial heritage or identity. Example: Having no representations of the women actually served anywhere in your practice. Derald Wing Sue. Racial Microaggressions in Everyday Life: Race, Gender and Sexual Orientation (John Wiley & Sons, 2010) Conscious and intentional discriminatory actions: Example: Hiring a dominant culture person to fill a role that would have been better filled with a representative of the women you serve. Derald Wing Sue. Racial Microaggressions in Everyday Life: Race, Gender and Sexual Orientation (John Wiley & Sons, 2010), Marginalization- relegated to the fringes Invisibility- not noticed enough to be included Trivialization- issues are dismissed Infantilization- to treat like a child Medicalization- to treat as a medical condition Dehumanization or objectification-to treat as an object Using the data of communities or populations that demonstrate great disparities, to gain funding or other assets then using those funds or assets to benefit anyone other than the community whose data was used. Running programs to end disparities that remain ineffective in changing outcomes Talking the talk of ending disparities but not walking the walk White privilege (or white skin privilege) refers to the set of societal privileges that white people are argued to benefit from beyond those commonly experienced by people of color in the same social, political, or economic spaces (nation, community, workplace, income, etc.). ... What is the role of ‘antiracism training’? Does your environment reflect the women you serve or does it reflect you? Does your staff reflect the population you serve (at all levels of the organization?) What are your own internal biases? How are your biases reflected in your practice? Diversity within and between cultures Distinguish culture from class Specific women have specific needs It’s not nature; it’s failure to nurture What is an ally? Purpose to follow and not to lead See your replacement in the population you serve Removing your cloak of privilege Engage your clients in meaningful dialog (Did you ever ask what they wanted?) Understand community strengths and capitalize on them What resources do you utilize that come from within the community? Promote cultural practices that are helpful, be neutral toward practices that are harmless, and educate about practices that are truly harmful You may have to sit with a lot of discomfort on the way to growth Not everyone will understand or approve Disparities in breastfeeding won’t end until we consciously address them How can you promote the work that is already being done in communities of color? How can you use your privilege to advance a colleague of color? How do engage other dominant culture people in the conversation around privilege and inequities? Recognizing the power and influence of culture Understanding how each of our backgrounds affects our responses to others Not assuming that all members of cultural groups share the same beliefs and practices Acknowledging how past experiences affect present interactions Building on the strengths and resources of each culture in an organization Allocating resources for leadership and staff development in the area of cultural awareness, sensitivity, and understanding Actively eliminating prejudice in policies and practices Cricco-Lizza R., (2006)., Black Non Hispanic mother’s perception about the promotion of infant feeding methods by nurses and physicians. JOGNN: Journal of Obstetric, Gynecologic & Neonatal Nursing, MarApr; 35 (2): 173-80. Freeman, K., Bonuck, K.A., Trombley, M., (2008). Journal of Human Lactation, Breastfeeding and infant illness in low income minority women; a prosepective cohort study of the dose-response relationship. Feb; 24 (1): 14-26. Forste, R., Weiss, J., (2001). The decision to breastfeedi in the United States. Does race matter? Lippincott E; Pediatrics, Aug; 108 (2 part 1): 291-6 Lee, H., Rubio, M.R., Elo, I.T., McCollum, K.F., Chung, E.K., Culhane, J.F., Factors associated with intention to breastfeed among low-income, inner-city women. Maternal & Child Health Journal, 2005 Sep; 9 (3): 253-61 McCarter-Spaulding, D., (2007). Black women’s experience of Breastfeeding; A focus group’s perspective. Journal of Multicultural Nursing & Health, Winter-Spring; 13 (1): 18-27. Micken, A.D., Modeste, N., Montgomery, S., Taylo,r M., (2009). Peer support and breastfeeding intention among Black WIC participants. Journal of Human Lactation May; 25 (2): 157-62 Ramey, R., (2005). Examing breastfeeding practices among low-income Black Women. Kentucky Nurse, JanMar; 53 (1): 13 Sherry L. Payne MSN RN CNE IBCLC Executive Director, Uzazi Village http://urbanvillagemidwife.blogspot.com sherry@uzazivillage.com www.uzazivillage.com Find me on Facebook and Twitter! Kansas City, MO 913-638-0716