Patient-Centered Care
advertisement

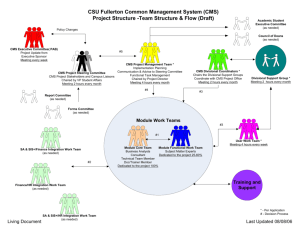
Quality & Hospital Acquired Conditions Rebecca Armbruster, DO, MS, FACOI Medical Director Resource Management Patricia Heys, BS Director of Infection Prevention & Control Sally Hinkle, DNP, MPA, RN Director of Performance Improvement & Clinical Value Institute of Medicine Six Aims for Improving Health Care Quality • Safe Care – Avoiding injuries to patients • Effective Care – Providing care based on scientific knowledge • Patient-Centered Care – Providing respectful & responsive care that ensures that patient values guide clinical decisions • Timely Care – Reducing waits for both patients & providers of care • Efficient Care – Avoiding waste • Equitable Care – Providing consistent quality of care HOSPITAL ACQUIRED CONDITIONS The Centers for Medicare and Medicaid Services (CMS) has identified 11 types of medical occurrences that: • Are Preventable • Are high cost or high volume • Result in additional costs to CMS These are referred to as never events NEVER EVENTS • • • • • • • • Foreign Object Retain After Surgery Air Embolism Blood Incompatibility Stage III and IV Pressures Ulcers Falls and Trauma Catheter Associated Urinary Tract Infections Vascular Catheter Associated Blood Stream Infections Surgical Site Infections Following Coronary Artery Bypass Graft and Following Certain Orthopedic and Bariatric Procedures • Certain Manifestations of Poor Control of Blood Sugar Levels • Deep Vein Thrombosis or Pulmonary Embolism Following Total Knee and Total Hip Replacement ACT 52 Patients must be notified in writing of all hospital acquired conditions in the Commonwealth of Pennsylvania TWO AREAS TO FOCUS ON Identify, document and code those conditions present on admission Prevent conditions from occurring Case Study What conditions were present at the time of admission? Were there any infections that resulted from the care delivered during the inpatient admission? • 50 year old female with past history of obesity, schizophrenia, and sleep apnea (remote tracheostomy) • Presents with Back pain and Chest Pain • Positives on exam: • pulse ox 91% room air, heart rate 120, respiratory rate 20 • Oriented x 2, mild respiratory distress, • rales at bilateral bases • Obese, mild diffuse abdominal tenderness • Abnormal labs/tests: • White blood count 23.9, Hemoglobin: 9, Sodium 130, bicarb: 10, Creatine 1.37, Glucose 540 (anion gap of 25) • Amylase and Lipase both elevated • Urine: + ketones, blood, protein • Cat Scan thorax: multiple pulmonary nodules, consistent with metastatic disease “50 year old with Chest pain, shortness of breath and cough, found to have Diabetic ketoacidosis and Anion Gap Metabolic acidosis” Day 1: Admit for 1. Diabetic Ketoacidosis(no history of Diabetes), may be secondary to pancreatitis, rule out infection, pan culture, start insulin drip, fluids, antibiotics. 2. Pulmonary nodules- concern for unknown primary, check cat scan of chest/abdomen/pelvis, 3. Pancreatitisnothing to eat, 4. Chest pain- rule out acute coronary syndrome. Day 4: Condition declines, with worsening respiratory distress-possibly due to Pancreatitis, continued leukocytosis and fevers- possibly due to Diabetic Ketoacidosis. And she was found on the floor. Day 7: increasing oxygen requirements, now requiring full ventilator support- possibly due to Pulmonary Embolus. Check dopplers and cat scan. And found to have Vaginal bleeding. Day 15: Hypotension- due to sepsis (on multiple drips), Hypoxic respiratory failure –due to pulmonary embolus (on heparin), Multiorgan system failuredue to sepsis Discharge summary: The patient had a long and complicated course which included being treated for Diabetic ketoacidosis and PNEUMONIA! So what if … • White Blood Cell Count Is 9.6 • Urinalysis Is Negative • Input / Output Requires Foley Catheter On Admission Core Measures • Set of best practice standards proven to decrease morbidity, mortality & readmission rates • Process indicators tied to clinical outcomes & improved quality • Mandated by Centers for Medicare & Medicaid Services (CMS) & The Joint Commission (TJC) • Links healthcare provider performance practices to facility reimbursement Core Measures Measuring the Care You Deliver FY'11 Target FY 2011 FY'12 Target FY 2012 CMS/TJC AMI-1 Aspirin at arrival 100% 99.1% 100% 99.7% 100% 100.0% 98.9% 100.0% 98.8% 99.2% CMS/TJC AMI-2 Aspirin at discharge 100% 98.7% 100% 100.0% 100% 100.0% 100.0% 100.0% 100.0% 100.0% CMS/TJC AMI-3 ACE-I or ARB for LVSD 100% 95.1% 100% 98.8% 100% 100.0% 100.0% 100.0% 100.0% 100.0% CMS/TJC AMI-5 Beta blocker at d/c 100% 99.3% 100% 99.7% 100% 100.0% 100.0% 100.0% 100.0% 100.0% NA 100% NA NA NA NA NA Required by Core Measures FY'13 Target Source FY'13 Target FY'12 Q4 FY'13 Q1 FY'13 Q2 FY'13 Q3 FY'13 Q4 FY 2013 To Date Inpatient Acute Myocardial Infarction (AMI) HQA - Top 10% CMS/VBP/TJC AMI-7a Fibrinolysis w/i 30 min of arrival 100% NA 100% CMS/VBP/TJC AMI-8a PCI w/i 90 min of arrival 99% 86.7% 100% 90.2% 100% 100.0% 100.0% 100.0% 100.0% 100.0% NA 98.4% NA 100.0% 100% 100.0% 100.0% 98.6% 100.0% 99.5% 99.8% 95.5% 99.8% 98.4% 99.9% 100.0% 98.9% 98.8% 98.9% 98.8% 99% 96.1% 100% 97.8% 100% 97.4% 97.0% 94.7% 98.3% 96.5% 100% 100.0% 100.0% 100.0% 100.0% 100.0% 100% 100.0% 99.0% 100.0% 100.0% 99.7% 97.6% 97.3% 94.9% 98.4% 96.8% CMS/TJC AMI-10 Statin Prescribed at discharge ACM for AMI (CMS methodology) QIO - Top 10% Heart Failure (HF) CMS/VBP/TJC HF-1 D/C instructions HQA - Top 10% CMS/TJC HF-2 Evaluation of LVSF 100% 99.8% 100% 100.0% CMS/TJC HF-3 ACE-I or ARB for LVSD 100% 97.3% 100% 99.6% 99.5% 94.8% 99.8% 97.7% QIO - Top 10% 99.9% ACM for HF (CMS methodology) Pneumonia (PN) CMS/VBP/TJC PN-3b Bld cultures prior to antibiotic 100% 97.0% 100% 98.7% 97.6% 100.0% 100.0% 100.0% 100.0% PN-6 Antibiotic Selection ICU and non-ICU 98% 97.4% 99% 99.4% HQA - Top 10% 100% CMS/VBP/TJC 100% 100.0% 96.7% 100.0% 96.6% 97.7% 98.6% 93.1% 99.1% 97.6% QIO - Top 10% 99.5% 98.5% 98.5% 100.0% 98.2% 98.8% ACM for PN (CMS methodology) 14 CMS Hospital Value-Based Purchasing Program (VBP) • Required in the Affordable Care Act • Quality incentive program built on the Hospital Inpatient Quality Reporting • Rewards value, patient outcomes & innovations • Hospitals have potential to earn more than 1.50% based on total performance VBP Domains, Measures & Dimensions Get Involved in Quality & Safety Accountable Care Units: Huddles, Multidisciplinary Rounds, Mini RCA’s, Throughput, Patient Satisfaction, Core Measures, Infection Control Resident Integration Into Quality House Staff Quality Council & Program Level PI/QI Medical Staff Committees: Patient Safety, Performance Improvement, Peer Review Centers for Medicare & Medicaid Services Health care quality is: Getting the right care to the right patient – every time REMEMBER • Always keep the patient at the center of everything that you do • Provide care based on nationally excepted best practices • Document conditions that are present on admission • And last but not least ... 19 WASH YOUR HANDS! 20