Practical Steps for Getting Started
Wendy Lewis
Programme Manager
© 2012 AQuA
This session:
• Discuss the key elements of your local implementation plan
• Practical activities to get you started
• Based on the Implementation Guide
• Access to advice, guidance and support
© 2012 AQuA
2
Implementation Plan
1. Stakeholder analysis
2. Stakeholder engagement
3. Engaging with Commissioners
4. Team working
5. Understanding your current service
6. Understanding the risks
7. Understanding the investment required
8. Maintaining momentum
9. Testing and making changes to your pathway
10.Sustaining the change
Implementation Plan
1. Stakeholder analysis
2. Stakeholder engagement
3. Engaging with Commissioners
4. Team working
5. Understanding your current service
6. Understanding the risks
7. Understanding the investment required
8. Maintaining momentum
9. Testing and making changes to your pathway
10. Sustaining the change
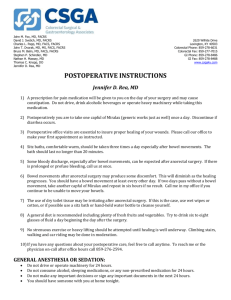
Stakeholder Analysis
High
Influence
Satisfy
Manage
•Opinion formers
Key Stakeholders need to be fully
engaged through full
communication & consultation
•Keep satisfied
•Review regularly
Inform / Monitor
Little / No
Influence
Not crucial to the process but useful
to keep informed
Little / No
Interest
Involve
•Voices that need to be heard
•Need to be proactive
High interest
Stakeholder Analysis – Activity
On the blank map provided start your stakeholder analysis by identifying your
stakeholders with high influence and high interest that you need to
actively manage
High
Influence
Satisfy
Manage
•Opinion formers
Key Stakeholders need to be fully engaged
through full communication &
consultation
•Keep satisfied
•Review regularly
Little / No
Influence
Inform / Monitor
Involve
Not crucial to the
process but useful to
keep informed
•Voices that need to be heard
Little/No
Interest
•Need to be proactive
High
interest
Identifying the team
Implementation requires a number of factors:
• Changing clinical interventions
• Changing care systems and processes
• Creating a team to work across the patient pathway
• Both require technical and behavioural change management
• Lets start with thinking about who to engage and how to
structure the project team
Essential Roles
Sponsors:
•authority to sanction change (organisational alignment / benefit)
Change Agents
•facilitate change, require knowledge, skills and credibility
Champions
•respected opinion leaders who positively promote work
•lead by example
Optimal Project Leadership
CEO
or Executive Sponsor
Project Lead /
Manager
Project Leadership
Clinical Leads
Information
Support
Ham 2001 (Report for NHS MA)
©NHS Institute for Innovation and Improvement 2006
Identifying the Team - Activity
• Consider who will take the roles of:
– Sponsor?
– Change Agent?
– Champion?
• Who will take the essential project roles:
– Project Lead / Manager?
– Clinical Lead?
• Who will provide information management support?
Understanding your current service
Referral from
Primary Care
• Optimising pre operative
haemoglobin levels
• Managing pre existing co morbidities
e.g. diabetes
PreOperative
•Admission on day
•Optimised Fluid Hydration
•CHO Loading
•Reduced starvation
•No / reduced oral bowel
preparation ( bowel
surgery)
•Planned mobilisation
•Rapid hydration &
nourishment
•Appropriate IV therapy
•No wound drains
•No NG (bowel surgery)
•Catheters removed early
•Regular oral analgesia
•Paracetamol and NSAIDS
•Avoidance of systemic
opiate-based analgesia
where possible or
administered topically
Admission
•Optimised health / medical
condition
•Informed decision making
•Pre operative health & risk
assessment
•PT information and
expectation managed
•DX planning (EDD)
•Pre-operative therapy
instruction as appropriate
•Minimally invasive surgery
•Use of transverse incisions
(abdominal)
•No NG tube (bowel surgery)
•Use of regional / LA with
sedation
•Epidural management (inc
thoracic)
•Optimised fluid management
Individualised goal directed
fluid therapy
IntraOperative
PostOperative
•DX when criteria met
•Therapy support (stoma,
physio)
•24hr telephone follow up
Follow
Up
Understanding your current service- Activity
Referral from
Primary
Care
On
the
• Optimising pre operative
haemoglobin levels
• Managing pre existing co morbidities
e.g. diabetes
map provided:
Pre-
•Admission on day
•Optimised Fluid Hydration
•CHO Loading
•Reduced starvation
•No / reduced oral bowel
preparation ( bowel
surgery)
•Planned mobilisation
•Rapid hydration &
nourishment
•Appropriate IV therapy
•No wound drains
•No NG (bowel surgery)
•Catheters removed early
•Regular oral analgesia
•Paracetamol and NSAIDS
•Avoidance of systemic
opiate-based analgesia
where possible or
administered topically
• Mark the Operative
interventions you already have in place
You should also consider when, where and how they
are provided and whether
Admission there is further opportunity
for/ improvement
•Optimised health
medical
condition
•Informed decision making
•Pre operative health & risk
assessment
•PT information and
expectation managed
•DX planning (EDD)
•Pre-operative therapy
instruction as appropriate
•Minimally invasive surgery
•Use of transverse incisions
(abdominal)
•No NG tube (bowel surgery)
•Use of regional / LA with
sedation
•Epidural management (inc
thoracic)
•Optimised fluid management
Individualised goal directed
fluid therapy
Intrayou Operative
need to
• Identify the interventions
establish
and start to consider the sequence for
Postimplementation
Operative
•DX when criteria met
•Therapy support (stoma,
physio)
•24hr telephone follow up
Follow
Up
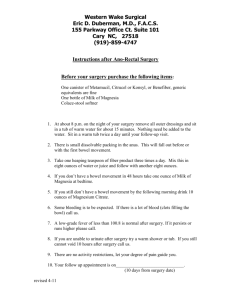
Understanding and improving systems and processes
Patient Pathway
Undertake mapping and tracking
Increasing level of detail
Measuring and understanding the baseline
Measurement
Aspect
Improvement
Accountability
Research
Aim
Improvement of care
Comparison, choice,
reassurance, spur for
change
New knowledge
Methods:
Tests are observable
No test; merely
evaluate current
performance
Test blinded or controlled tests
Bias
Accept consistent bias
Measure and adjust to
reduce bias
Design to eliminate bias
Sample Size
“Just enough” data,
small sequential
samples
Obtain 100% of
available, relevant
data
“Just in case” data
Flexibility of
No hypothesis
Fixed hypothesis
Hypothesis
Hypothesis flexible,
changes as learning
takes place
Testing Strategy
Sequential tests
No tests
One large test
Determining if a
Change is an
Improvement
Run charts or control
charts
No change focus
Hypothesis, statistical tests (t-test,
F-test, chi square),
p-vlaues
Confidentiality of
the Data
Data used only by
those involved with
improvement
Data available for
public consumption
and review
Research subjects’ identities
protected
Test Observability
Measures for improvement
• Outcome
– Length of stay
– Patient experience
• Balancing
– Re-operations
– Readmissions
– Complications
• Process
– ER pathway interventions
Benefits Realisation
Using Measures for improvement - Activity
Look at the list of programme measures:
•How will you make your baseline measurement?
•How will measure on an on going basis?
•How you will use the measures to drive improvements?
Steps for Improvement
- Right first time and every time
• First step - Reduce defects
such as avoidable infections
• Second Step – Reduce waste (cost)
such as losing and repeating a blood test
• Third Step – Enhancements or new features
such as a new treatment or cure
Invest in Quality Improvement
- the Sand Cone Model
Ferdows and De Meyer 1990
Model for improvement
What are we trying to
accomplish?
How will we know that a
change is an improvement?
What changes can we make
that will result in the improvements
that we seek ?
Copyright IHI 2000
Act
Plan
Study
Do
aims
measures
change principles & ideas
testing ideas before
implementing changes
Using multiple tests of change
D
S
A
T
A
A
D
A P
D S
P A
Changes that
result in
improvement
S D
P
A P
Hunches
theories
ideas
S D
Need to start small!!
Managing improvement
low
Test on
a very
small
scale
Agreement
amongst the
key players
Just
do it
JDI
high
high
Certainty
that the change
will work
low
MeasuringChanging
the impact of
the tests of change
process
Journey Time (hours)
25
Changed
Process
20
Second
Process
Change
15
Third Process Fourth
Change
Process
Change
10
5
0
Jan
Apr
Jul
Oct
Jan
Apr
Month
Jul
Oct
Jan
Apr
Jul
What will be your first test of change?
Remember the importance of a quick win as well as a
plan for sustainability
Critical Factors for Sustainability
©NHS Institute for Innovation and Improvement 2006
Making it Happen
• Will
• Ideas
• Execution
IHI Framework for Leadership for Improvement 2008
Advice guidance and support
• Literature and toolkits
• AQuA ER Network
• Websites - AQuA Portal
• Who in your local organisation can help?
 0
0