Upper and Lower Extremity Provacative Testing
advertisement

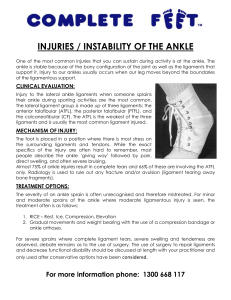
Provocative Testing & Diagnostics of Upper & Lower Extremity Conditions Tom Winters, MD, FACOEM, FACPM Chief Medical Officer CareGroup Occupational Health Network Walter Panis, MD Medical Director CareGroup Occupational Health Network June 6, 2002 Copyright 2002 CareGroup Occupational Health Network The Knee • Approx. 10.8 million knee injuries per year in general population • Why so many injuries – Largest joint in body – Dynamic nature of joint increases vulnerability – Very little bony stabilityrelies on normal ligaments, cartilage and tendons Ref: AAOS Research Dept., Pt. Visits for selected conditions, 1998 Anatomy of the Knee • Bones: – Femur – Tibia – Patella • Cartilage (shock absorbers) – Lateral Meniscus – Medial Meniscus – Articular cartilage is nerveless Anatomy of the Knee • Ligaments – 4 major ligaments (attach bone to bone) • • • • Anterior Cruciate Posterior Cruciate Medial Collateral Lateral Collateral Anatomy of the Knee • Patellar and Extensor tendons (attach Quadriceps to bone) – Major tendons • Synovium – Inner joint lining • Synovial fluid – Joint lubrication Types of Knee Injuries • ACL tear • Bursitis (“Housemaids knee”) • Collateral ligament tear • Posterior ligament tear • Meniscal tear • • • • Fracture of tibia Fracture of patella Sprain/strain Patellar/quadriceps tendinitis • Patellofemoral pain • Extensor mechanism rupture Types of Knee Injuries • Ligament Injuries – ACL: changing direction quickly, twisting, pivoting, deceleration activities – PCL: blow to front of knee (“dashboard injury”), hyperextension / hyperflexion – MCL: contact with outside of knee, valgus force (common) – LCL: knee forced laterally, varus force (less common) Types of Knee Injuries (cont.) • Meniscal Tears – Medial/Lateral Meniscal Tear: • Twisting,cutting, pivoting, rapid deceleration types of motions • Movement around a fixed lower leg (stationary) or planted foot Examination of the Knee • Inspection (always examine uninjured knee 1st!) – – – – – Note onset- acute/gradual Type/quality of pain Posture Bony deformities Muscle wasting • Quad wasting esp. in VM O seen with knee injury – Soft tissue swelling • Effusion of suprapatellar pouch, pre and infrapatellar bursae, palpable joint line swelling – Masses/lumps – Old scars – Pulses Examination of the Knee (cont.) • Palpation – Check bilaterally for temperature differences, inflammation – Palpate medial and lateral collateral compartments – Bursae – Medial/lateral meniscus – Medial/lateral ligament • Medial more common • “Bucket-handle” tear – Popliteal fossa Examination of the Knee (cont.) • Palpation (cont.) – Bony landmarks • Medial and lateral joint lines • Patello-femoral joint • Tibial tuberosity • Femoral condyles – Reflexes – Always check joint above and below (hip and ankle); hip pain may be referred to knee! Examination of the Knee (cont.) • Range of motion – Flexion = 130+ degrees – Extension = 0 (-10) degrees Special Knee Tests • Tests for ACL laxity – Anterior drawer sign – Lachman’s test – Pivot shift Anterior Draw Test Lachman’s Test Ref: Snider, R. The Essentials of Musculoskeletal Care. AAOS: 1997 Special Knee Tests (cont.) Posterior sag sign • PCL stress tests – – – – http://www.wokc2.com/topic3.htm Posterior sag sign Reverse Lachman’s Posterior draw sign Reverse pivot test Special Knee Tests (cont.) • McMurray’s/ Apley’s grind test (meniscus) • Apprehension test (patella) • Crepitus sub-patella • Pathological “locking/giving out” McMurray’s Test – Due to intra-articular fragment of bone or cartilage wedging between femoral & tibial condyles – Joint unable to fully extend (fixed flexion deformity) Ref: Hoppenfeld,S. Physical Examination of the Spine & Extremities. Prentice-Hall: 1976. Grading Ligament Injuries • Grade I (sprain): – Micro-tearing or stretching – Joint is stable • Grade II (sprain): – – – – Partial disruption of ligament Painful to stress joint Joint laxity with endpoint Mild effusion • Grade III (tear): – Complete tear – Joint laxity without endpoint – effusion Diagnostic Procedures • X-ray – Indications • MRI – Best to view: • Meniscus, ligaments, soft tissue – Indications • CAT Scan – Best to view: • Bone – Indications Diagnostic Procedures • Arthrogram (infrequently performed) • Arthroscopy (preferred method) Treatment of Knee Injuries • • • • • Rest Ice Compression Elevation Anti-inflammatories – NSAIDs – COX-2 Types of Knee Braces • Types of bracing: – Prophylactic – Functional – Rehabilitative/knee immobilizer – Patellorfemoral • Often work better in lab than in real life use • Functional and Rehabilitative seem to be of most use • Stretching, strengthening,and technique improvement more important in long Anatomy of the Foot and Ankle • Bones – “True ankle joint” • Tibia • Fibula • Talus A. Second part of ankle • Subtalar joint • Calcaneus (heal) – Foot • Tarsals • Metatarsals • Phalanges Ref: http://www.soarmedical.com/medical-library/foot&ankle/ Anatomy of the Foot and Ankle (cont.) • Cartilage & ligaments – Articular cartilage (1) – Anterior tibiofibular (2) • Connects tibia to fibula • Most commonly injured – Collateral lateral ligaments (3) • Attaches fibula to calcaneuslateral stability – Deltoid ligaments (4) • Connect tibia to talus and calcaneus- medial stability Ref: http://www.scoi.com/anklanat.htm Anatomy of the Foot and Ankle (cont.) • Tendons – Achilles tendon – Anterior tibial tendon – Posterior tibial tendon Examination of the Ankle and Foot • Inspection – Ecchymosis, bony abnormalities, soft tissue swelling, effusion – Note type of footwear- note wear pattern on soles – Gait • Palpation – Tenderness- certain areas of foot normally tender i.e.sinus tarsi, distal aspect of ball between metatarsals – Neurovascular status- Pulses, sensation – Crepitation – Tinel’s sign (+ peroneal nerve injury) • Range of motion Special Tests of the Ankle and Foot • • • • • • Eversion stress (Medial stress test) Drawer test Anterior drawer test (tests stability-ATF ligament) Lateral stress External rotation test (Kleiger test) Squeeze test (testing for fx of tibia or fibula) • Heel tap test Types of Ankle and Foot Injuries • Plantar fasciitis • Tarsal tunnel syndrome (ladders) • Insertional Achilles tendinitis • Stress fracture of calcaneus • March fracture (stress fx) • Sesamoiditis • Fracture of the sesamoid Sprain versus Strain • Sprain: twisting of joint that stretches or tears ligaments, no dislocation of bones, may damage nearby blood vessels, muscles, tendons, swelling and hemorrhage • Strain: less serious injury, overstretched tendon or partially torn muscle Types of Ankle Injuries: Sprains • 1st degree: no (mild) edema, point tenderness, ligament stretching, no rupture (maybe crutches/cane) • 2nd degree: partial ligament rupture, edema, point tenderness, difficulty/inability to weight bear on ankle (crutches,splint) • 3rd degree: complete disruption one or more ligaments/other structures, edema, ecchymosis, general tenderness, inability to bear weight (crutches,splint, cast, surgery) Ankle Sprains • Forced inversion strain – Stretch, tear or rupture of lateral collateral ligament complex (possibly anterior talofibular lig.) • Forced eversion strain – Stretch, tear or rupture of medial collateral ligament • Lateral ankle compartment more commonly injured than medial Foot and Ankle Fractures • Types – Jones (fx of proximal metaphysis of 5th metatarsal) • Diagnosis – Routine use of x-rays to rule out sprain vs. fx “to do or not to do”clinical indications – Ottawa rules for foot and ankle radiographs (see web site) http://www.aafp. org/afp/980201ap/wexler.html • Treatment – ORIF – Casting Foot and Ankle Fractures Traumatic Injury • Direct trauma = external force strikes the foot • Indirect trauma = force transmitted to stationary foot so that weight of body becomes a deforming force by torque, rotation or, compression Ref: http://www.aafp.org/afp/980700ap/burrough.html Pain • Why are ankle injuries so painful? – Rich nerve supply (pain and proprioception is enhanced) – All ligaments have poor blood supply: slow to heal, heals with scar tissue, retains stretched condition Non-Surgical Treatment of Ankle Injuries • • • • Rest Ice Compression Elevation Types of Ankle Support • Non-rigid (1st degree sprains): – Elastic wrap/neoprene • Not OSHA recordable • Purpose: compression, nonsupportive • Rigid: (1st, 2nd, 3rd degree sprains) – Lace-up, Aircast • Purpose: support, proprioception – Bracing • • • • AFO (ankle foot orthosis) Walking boot Cast shoe Cast Physical Therapy for Knee and Ankle Injuries • Does every lower extremity injury require physical therapy? – Benefits – How soon after injury should it be ordered? • Home exercises versus clinic therapy program – Nature of injury – Patient compliance issues Goals of Rehabilitation • Restoration of comfort – Decrease edema • R.I.C.E. – Address pain • NSAIDs • COX-2 agents • Refer complications early • Maintain Mobility – Active ROM & strengthening • Restore proprioception – Wobble board, minitrampoline • Work-hardening program or job specific exercise programs • Prevent future reinjury – Education • Understand injury, treatment, rehab and prevention strategies Upper Extremity Evaluation 1) 2) 3) • History Exam Diagnostic studies Key is putting all three together to make a “total” picture Low Back Pain • Most commonly seen musculoskeletal injury • In normal population 80% of us will have an LBP episode in their lifetime • 3-4% per yr. Will be temporarily disabled • 1% of working population will be permanently disabled Ref: www.emedicine.com/neuro/topic516.htm Myths of Low Back Pain • True or false: – All people with LPB need an x-ray – Rest is good for pain – MRI or CT must be done to provide definitive diagnosis – Vast majority of patients improve in 2-6 weeks with or without treatment (approx. 90%) Anatomy of the Lumbar Spine • No lateral support in lumbar spine (> mobility in sagittal and coronal planes) • Bony vertebrae – Transverse and spinous processes • Intervertebral disc – Outer annulus fibrosis – Inner nucleus pulposus Anatomy of the Lumbar Spine • Anatomical relationship between L4, L5 and S1 Anatomy of the Lumbar Spine • Specific nerve roots have specific functions and will elicit specific symptoms Diagnosing Low Back Pain: Sprain/Strain Injury • Vast majority of LBP is a sprain/strain injury – Ligamentous – Tendonitis • LBP most often over R lumbar sacral area – Tends to be localized – Referred pain not typically seen – Described as “aching” Diagnosing Low Back Pain: Nerve Root Compression • Back pain due to nerve root compression/radiculopathy less common – “Sciatica” is not a good term • Sciatic nerve= combination of tibial and peroneal nerve- forms well outside spinal canal where most back problems occur Diagnosing Low Back Pain: Nerve Root Compression • Impingement compression pathology of spinal nerve root – Initial complaint may be “electric shock down leg” • Mechanism= ICP due to intrathoracic pressure venous outflow from brain ICP pressure on nerve from disc causing burning/shooting pain – Parethesias • Numbness/tingling – Bowel/bladder involvement • Cauda Equina Syndrome • Medical/surgical emergency Diagnostic Studies for Low Back Pain • X-rays – ? value • MRI and CT scans – Asymptomatic disc herniations are commonly found on What is diagnostic value of this? – When should MRI or CT be done? Two Common Presentations of Low Back Pain • History: – 38 year old male experienced the following after lifting a 100 pound box from the floor to a shelf at work – 1) Localized back pain » OR – 2) Very specific burning pain radiating to leg Complaint #1 • Physical exam findings – – – – – – Non-specific Reflexes normal ROM, gait, posture Palpation of spine Response to light touch Provocative testing done • Straight leg raise • Heel to toe walk, squat and rise • Palpation of sciatic notch Complaint #1 • Diagnostic testing – Not usually indicated unless red flags are present i.e. fever, wght. loss, hx of cancer, use of steroids etc. • Likely diagnosis – Low back strain/sprain Complaint #1 • Treatment – NSAIDs – Physical therapy – May need modified duty/work restrictions – Importance of developing trusting relationship with patient to optimize outcome • Lou Millender, MD – “Love ‘em back to health!” Complaint #2 • Physical exam – Specific – Motor weakness in specific distribution – Abnormal reflexes – Sensory loss – Provocative testing • ? Cauda Equina syndrome if unable to heel toe walk or squat • + straight leg raise Complaint #2 • Diagnostic testing – X-rays not useful – MRI after 6 weeks of conservative treatment unless neuro symptoms – Electrophysiology studies • What are they • When are they done • What will they show • Likely diagnosis – Radiculopathy Complaint #2 • Treatment – – – – – Most improve on own Pain control Physical therapy Prednisone/epidural steroids May need to be out of work for 1-2 days during acute symptoms – Surgical intervention – May require work restrictions/modified duty Provocative Testing of the Shoulder • Apley scratch test – Maneuver = touch superior/inferior aspects of opposite scapula – Positive result (< ROM) = rotator cuff problem • Neer’s test – Maneuver = place arm in forced flexion with arm fully pronated – Positive result (pain) = subacromial impingement Neer’s Provocative Testing of the Shoulder • Crossed arm test – Maneuver = raise arm to 90 degrees then actively adduct armforces the acromion into the distal end of the clavicle – Positive result (pain) = disorder of acromioclavicular joint CROSSED ARM Provocative Testing of the Shoulder • Hawkin’s test – Maneuver = elevate arm forward to 90 degrees while forcibly internally rotating shoulder – Positive result (pain) = subacromial impingement or rotator cuff tendonitis • Drop arm test – Maneuver = Passively abduct shoulder, observe pt. lowering arm to waist – Positive result (arm will drop to side) = rotator cuff tear HAWKIN’S Provocative Testing of the Elbow and Hand • Phalen’s test – Maneuver = press back of hands together with wrists fully flexed, hold 60 seconds – Positive result (numbness/tingling) = carpal tunnel syndrome, median nerve Provocative Testing of the Elbow and Hand • Tinel’s sign – Maneuver = tap over the carpal tunnel area (hand) or tap ulnar notch between olecranon process and medical epicondyle (elbow) – Positive result (pain, tingling or electric sensation in hand) = carpal tunnel syndrome, median nerve in hand or ulnar nerve compromise in elbow Case Studies • MRI case study – Terminology • T1 and T2 weighting – What to look for in the report • Electromyelogram case study – How they are done – What to look for in the report References • http://.bledsoebrace.com/education/cp03001 2.htm • http://bledsoebrace.com/products/products.h tm • http://www.fpnotebook.com/ORT55.htm • http://orthoinfo.aaos.org References • Karen Muller, MPT, Journal of Orthopaedic & Sports Physical Therapy, 2000;30(3): 138-142 • The Physician and Sports Medicine: Patellofemoral pain • mmg.Sechrest.com • www.kneeguru.co.uk • Taylor, S., P.T., “Diagnosis, Management and Treatment of Knee Disorders: The Extensor Mechanism”, PowerPoint Presentation, New England Baptist Hospital, 2001.