Classification of the Essential Medicines List (EML) according to BCS
 according to BCS")
Multisource (generic) products and Interchangeability
Training Workshop on Dissolution,
Pharmaceutical Product Interchangeability and Biopharmaceutical Classification System.
Hotel Bratislava
1 Malyshko Street
Kyiv, Ukraine
Date: 25 to 27 June 2007
WHO Prequalification Programme June 2007
Pharmaceutical Development
Classification of the Essential Medicines List
(EML) according to BCS
Presenter: Marc Lindenberg
Analytical Development (PTDF-A)
F. Hoffmann-La Roche Ltd.
Basel, Switzerland
E-mail: marc.lindenberg@roche.com
WHO Prequalification Programme June 2007
What does BCS stand for?
Biopharmaceutics Classification System
Class I
Highly soluble
Highly permeable
Class III
Highly soluble
Poorly permeable
Class II
Poorly soluble
Highly permeable
Class IV
Poorly soluble
Poorly permeable
WHO Prequalification Programme June 2007
Criteria for „high“ solubility - FDA
Highest single dosage strength divided by the solubility of the compound over the pH range 1-7.5 at 37 °C
<250 ml „highly“ soluble
250 ml: Amount of fluid present in the upper GI-tract when administering the drug in the fasted state
Method of choice: saturation shake-flask method
Other methods are accepted if shown to produce similar results to the shake-flask method
WHO Prequalification Programme June 2007
Criteria for „high“ permeability - FDA
Permeability > 90% „highly“ permeable
Measured in humans, animals or suitable cell lines
(Caco II cells)
Determination in Caco II cells only applicable to passively absorbed substances
Traning set to validate the cell experiments required
WHO Prequalification Programme June 2007
Biowaiver - FDA
Approval of SUPAC changes or of a generic product on the basis on in vitro tests alone
Requires:
Class I compound
>85% dissolved within 30 minutes in media which mimic physiological pH values (pH 1.2 – 6.8) @ 50 rpm paddle or @ 100 rpm basket
No addition of lecithin, bile salts or enzyme
WHO Prequalification Programme June 2007
BCS – WHO classification
Differences to FDA requirements:
Solubility determination at pH 1.2 – 6.8
Permeability > 85 % leads to a „highly“ permeable classification
Biowaiver: Class III copmound are eligible biowaiver if they dissolve within 15 minutes in buffer media pH 1.2 –6.8 (75 rpm)
Biowaiver: Class II acids with D:S ratio < 250 ml in at pH 6.8 and >
85 % dissolved within 30 minutes at pH 6.8 (75 rpm)
WHO Prequalification Programme June 2007
WHO Essential Medicines List (EML)
Minimum medicine needs for a basic health system (core list)
Complementary list includes medicines which require specialized equipment (e.g. for monitoring) or specialist training
Selected by relevance, safety and cost-effectiveness
Newest version may be downloaded here:
http://www.who.int/medicines/publications/EssMedList15.pdf
WHO Prequalification Programme June 2007
Methods
Literature search for suitable solubility and permeability data
Missing or insufficient solubility data was supplemented by experimental determination
WHO Prequalification Programme June 2007
Solubility determination: Sources
Literature: Martindale, Merck Index, Florey`s Analytical
Drug Profiles,…
Internet: Medline with different keywords (e.g. aqueous, solubility…)
Experiments: Saturation shake-flask method
WHO Prequalification Programme June 2007
Solubility determination: Experiments
Excess of substance is weighed into a vessel (2-3 times expected solubility)
Exact amount of buffer medium is added
Put on an orbital shaker for a specified amount of time at
37 °C
Measure concentration at specific time points
Ensure that no degradation occurs or that degradation is detected via analytical method
WHO Prequalification Programme June 2007
Solubility determination: Problems with literature data
Solubility only tested in water
Solubility tested only at room temperature
Only one pH value tested
Was the pH value kept constant throughout the whole experiment?
Was the pH value measured in a buffered medium or only adjusted by addition of acid or base?
WHO Prequalification Programme June 2007
Solubility determination: Flow Chart
Determine solubility experimentally
D:S ratio above 250 ml at any pH value
(1-7.5) based on literature data?
yes
„
Low“ solubility no
Potential
„high“ solubility
Dependent on D:S ratio and pKa value „high“ solubility was assumed
D:S ratio < 250 ml at pH 1 –7.5 at 37
°C -> „high“ solubility
Solubility deemed uncertain
WHO Prequalification Programme June 2007
Permeability determination: Sources
Literature: Martindale, Merck Index, Florey`s Analytical
Drug Profiles,…
Internet: Medline with different keywords (e.g. permeability, bioavailability…)
WHO Prequalification Programme June 2007
Determination of permeability data from literature
Permeability data from humans was prefered
Data from Caco II cells was only used as additional confirmation
Animal data was only used if no other data could be found
Computer simluated data (clogP...) was not used as the
FDA currently does not accept this data for biowaiver decisions
WHO Prequalification Programme June 2007
Human permeability data
Bioavailability studies
Urin recovery
Radioactively marked substances
Perfusion studies in humans
WHO Prequalification Programme June 2007
Human permeability data
Bioavailability studies showing absolute bioavailability
> 90%
Urin recovery of the compound and its metabolites
> 90 %
Human perfusion studies providing direct permeability data
These data led to a reliable classification
WHO Prequalification Programme June 2007
Human permeability data - problems
Bioavailability below 90 %
Possible reasons:
Degradation in GI-tract
First pass effect
Solubility limited bioavailability
Poor absorption
WHO Prequalification Programme June 2007
Human permeability data - problems
Urinary recovery below 90 %
Possible reasons:
Biliar excretion
Solubility limited bioavailability
Poor absorption
Missing i.v.
comparison or missing metabolite assessment
WHO Prequalification Programme June 2007
Example of a reliable classification
Solubility
Minimum solubility at pH 1-8:
BCS Class
III
Permeability
“Low” permeability in human perfusion studies
6 mg/ml at 37 °C absolute BA 61% (oral vs iv)
D:S < 34 ml
Paracellular transport
Cimetidine
(200 mg)
WHO Prequalification Programme June 2007
Example of an uncertain classification
Solubility
Minimum solubility at pH 1-8:
BCS Class
IV
Permeability absolute BA 25% (oral vs iv)
0.8 mg/ml at 37 °C
BA study conducted in horses (!)
D:S > 312 ml
Acetazolamide
(250 mg)
WHO Prequalification Programme June 2007
Results – Classification according to FDA requirements
Of the 130 orally available medicines on the EML
(April, 2002):
64 could be classified reliably
25 could be classified provisionally
41 could not be classified unambiguously, but could be narrowed down on two classes
WHO Prequalification Programme June 2007
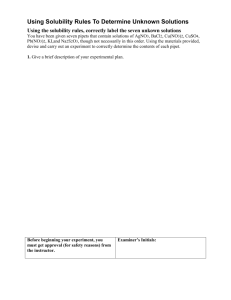
Results – Classification according to FDA requirements
9%
37%
38%
Class I
Class II
Class III
Class IV
16%
38 % could be classified as class I and are therefore potential biowaivers
75 % of the compounds show „high“ solubility
WHO Prequalification Programme June 2007
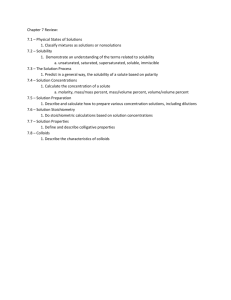
Results – Classification according to WHO requirements
9%
32%
43% Class I
Class II
Class III
Class IV
16%
Allopurinol, ascorbic acid, promethazine among others move from class III to class I (6 substances in total)
75 % of the compounds show „high“ solubility and are potential biowaiver
Weak acids in class II are also potential biowaiver
WHO Prequalification Programme June 2007
Potential biowaiver according to WHO criteria
Solubility pH 1.2: 0.04 mg/ml pH 5.5: 0.09 mg/ml pH 6.8: 2.47 mg/ml
D/S pH 6.8
: 162 ml
BCS Class
II
Permeability
BA 100%
“High” permeability in Caco II cells
Ibuprofen
(400 mg)
WHO Prequalification Programme June 2007
Biowaiver decision
Additional parameters for selecting compounds as biowaivers not covered by the list :
Excipients used in the formulation (surfactants..)
Excipient interaction with the compound
Therapeutic index
Therapeutic indication
Risk assessment
WHO Prequalification Programme June 2007
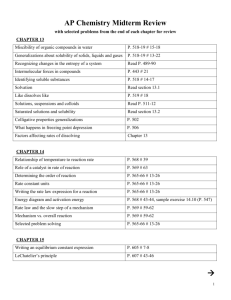
WHO Biowaiver monograph –
Ethambutol hydrochloride
Solubility
BCS Class
III
800
700
600
500
400
300
200
100
0
Solubility > 700 mg/ml
D/s ratio
400mg
< 0.7 ml
Biowaiver
With specific indications for monitoring of vision
120
100
80
60
40
20
0
0
USP SGF pH 1.2
10 time [min] phosphate buffer pH 4.5
20 30
USP SIFsp pH 6.8
“Very rapidly dissolving”
400 mg pure substance
Dissolution
Permeability
60-80% Urinary excretion after
144 h
12-19% recovery in the feces
Dose-proportional absorption
4-50 mg/kg
Indication: Long-term treatment of TB
Toxicity: Ocular
Monitoring of vision
Risks
WHO Prequalification Programme June 2007
Biowaiver decision
Detailed biowaiver monographs are available for various substances from the FIP
Monographs cover solubility, permeability, food and excipient interaction and pharmacokinetic behavior among others
Give advice on how to design meaningful dissolution tests
Published in Journal of Pharmaceutical Sciences
Or available from: http://www.fip.org/www2/sciences/index.php?page=pharmacy_sci ences&pharmacy_sciences=sciences_bioavail_groupbcs
WHO Prequalification Programme June 2007
References
Lindenberg et al.
„Classification of orally administered drugs on the World
Health Organization Model list of Essential Medicines according to the biopharmaceutics classification system.
EJPB; 2004 Sep; 58(2):265-78
WHO Prequalification Programme June 2007