SNP Model of Care Training Material
advertisement

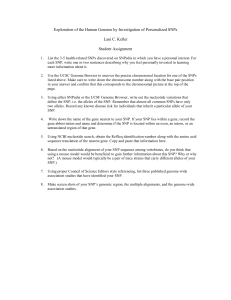
ATRIO Health Plans S NP Model of Care History of the SNP The Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA) authorized the creation of a type of Medicare Advantage (MA) plan referred to as a Special Needs Plan (SNP), to address the unique needs of certain Medicare populations. There are 3 categories of SNPs D-SNP (Dual Eligible; individuals who qualify for both Medicare Part A and Part B and full Medicaid benefits) I-SNP (Institutionalized; for individuals residing in nursing facilities or institutions) C-SNP (Chronic condition; for individuals with severe or disabling chronic conditions) ATRIO’s SNP beneficiaries are all classified as D-SNPs. DSNPs are the only kind of SNPs that ATRIO currently offers. In addition to meeting all the requirements of other MA plans, all SNPs, including D-SNPs, are required by the Centers of Medicare and Medicaid Services (CMS)---the agency in the Department of Health and Human Services (HHS) that administers Medicare and oversees Medicaid—to provide specialized services targeted to the needs of their beneficiaries, including a health risk assessment and an interdisciplinary care team for each beneficiary enrolled. SNPs, including D-SNPs, have been reauthorized several times since their establishment was first authorized in 2003. For example, the Medicare Improvements for Patients and Providers Act of 2008 (MIPPA) and the Patient Protection and Affordable Care Act (PPACA—effective January 1, 2012) both contain provisions reauthorizing and modifying SNPs. CMS requires D-SNPs to develop a model of care (MOC) that describes their approach to caring for their target population. The SNP MOC is a working framework (“the promise”) indicating how the SNP proposes to coordinate the care of SNP enrollees. The MOC in years past has included 11 Elements and for CY2015—NCQA & CMS have revised the MOC requirements to include 4 sections with a total of 15 elements. The 4 sections are: MOC 1: Description of SNP Population MOC 2: Care Coordination MOC 3: Provider Network MOC 4: MOC Quality Measurement and Performance Improvement It is a CMS requirement that all employed and contracted staff who provide indirect and direct care coordination services to SNP members complete an initial SNP MOC training as well as annual SNP MOC training thereafter. ATRIO will provide the annual SNP MOC training for all employed and contracted staff and maintain the documentation of completion of that training as required. ATRIO will provide the most current SNP MOC training to each of the SACs and delegates the responsibility that the SAC provide the initial SNP MOC training for any new hire who provides indirect or direct care coordination services to SNP members and to maintain the documentation of the completion of that training as required (for further information please refer to ATRIO’s SNP MOC Policy & Procedure). In order to access comprehensive this SNP MOC Training will be followed by a short quiz. MOC 1: Description of SNP Population A comprehensive description of ATRIO’s SNP-specific population that addresses the full continuum of care for current and potential SNP beneficiaries and describes the specially tailored services for these most vulnerable members. The description includes social, cognitive, environmental, living conditions and medical and health conditions including co-morbidities of ATRIO’s SNP population. Demographic Breakdown of ATRIO’s SNP Population SNP Gender M 41% F M F 59% *Data as of January 2015 Age 86-99 7% Age 100+ 0% SNP Age Distribution Age 0-50 24% Age 64-85 44% Age 51-63 25% Age 0-50 Age 51-63 Age 64-85 Age 86-99 Age 100+ Spanish 7% Russian 3% Vietnamese 1% SNP Languages Other 1% English 88% OTHER NATIVE AMERICAN 2% 1% AFRICANAMERICAN 1% ASIAN 2% SNP Ethnicity HISPANIC 7% AFRICAN-AMERICAN ASIAN CAUCASIAN HISPANIC NATIVE AMERICAN OTHER CAUCASIAN 87% SNP Low Income Subsidy 1 2 3 MOC 1 then goes on to detail the specially tailored services ATRIO provides to its most vulnerable members and established relationships with partners in the community to provide needed resources. Services and programs include: • • • • • • • • • • • TOC program (Transitions of Care) CCM program (Complex Case Management) ICT activities (Interdisciplinary Care Team) CHE programs (Comprehensive Home Evaluations) QIPs (Quality Improvement Programs) CCIP (Chronic Care Improvement Program) ENCC (Exceptional Needs Care Coordination) EDIT (Emergency Department Interdisciplinary Care Team) Medication Therapy Management Overutilization of Opioids Pharmaceutical Program CCSMP/Living Health Program (Chronic Care Self-Management Program) Community partnerships include: • • • • • • • • • • • • • • • • OHP (Oregon Health Plan) including the SAC CCOs Service area Behavioral and Mental Health Organizations NWSDS (Northwest Senior and Disabled Services) Service area Pharmacies Service area Provider practices Palliative and Hospice Care services Service area Hospitals Triplink Various not-for-profits Adult Foster Homes Skilled Nursing Facilities Assisted Living Facilities Rehabilitation Facilities Mental Health Inpatient and Outpatient Facilities Specialty Pain Clinics Meals on Wheels *For more details of what these programs and partnerships consist of please refer to ATRIO’s SNP MOC; MOC 1; Element B. MOC 2: Care Coordination Helps ensure that SNP beneficiaries’ health care needs, preference for health services and information sharing across the health care staff and facilities are met over time. Care coordination maximizes the use of effective, efficient, safe, high-quality patient services that ultimately lead to improved health care outcomes. The first Element A of MOC 2 is all about the SNP Staff Structure. There has at times been a misconception that care coordination consists of only the nurses and specially the SAC (Service Area Contract) NCM (Nurse Case Managers) and this is not at all accurate. With over 5000 SNP members it takes much more than the efforts made by the SAC NCMs to coordinate care services for our SNP members. Element B of MOC 2 addresses the HRAT (Health Risk Assessment Tool). The HRA is a comprehensive document used by the Plan to identify the specialized needs of its beneficiaries and to coordinate care that reflects the member’s personal preferences. The HRA questionnaire assesses medical, psychosocial, cognitive, and functional needs as well as the SNP member’s medical and mental health history. The SAC NCMs and other ICT members use the HRAs to develop ICPs (Individualized Care Plans) by assisting in the identification of prioritized needs, specific goals and appropriate interventions. Per CMS requirements each SNP member is sent an initial HRA at the time of a new enrollment and annually thereafter. Home visits in the form of CHEs (Comprehensive Home Evaluations) are also conducted on a regular basis to collect HRA information on high risk SNP members. SNP members who are unable to complete the written form of the HRA or participate in a CHE can also always request HRA completion assistance over the phone with one of our NCMs. Element C of MOC 2 addresses the ICP (Individualized Care Plan). ATRIO has adopted the CMS definition of a care plan meaning “a set of information about the patient that facilitates communication, collaboration and continuity of care across settings”. ATRIO has developed a customizable ICP within the designated case management software (TCS Acuity). The components of this ICP include: • SNP member demographic information including contact information • Primary Care Provider & contact information • A list of other providers the members has seen in the past 12 months • Current health insurance coverage and eligibility information • A list of allergies • A list of medications • A list of care diagnoses • A Case Management note from the assigned NCM • A list of active goals and associated interventions • A list of ICT members ATRIO delegates the responsibility of development and management of the ICP to the SAC assigned NCM. The ICPs are contained within the case management software and are generated using SNP member specific information from a variety of sources including but not limited to: claims, the HRA, CHE, medical records and information gathered by the NCM and other ICT members from the SNP beneficiary and/or caregiver(s). The case management software serves as the central location for the documentation of care management and care coordination activities. Element D of MOC 2 addresses Interdisciplinary Care Teams (ICT). ATRIO has adopted the CMS definition of an Interdisciplinary Care Team to refer to “a team of professionals from multiple disciplines who work together to coordinated and facilitate patient focused care”. ATRIO delegates this process to its Service Area Contractors (SAC). Each SAC is responsible to follow the specific ATRIO ICT policy and procedure (located within the SNP CM Policy and Procedure) as well as the framework outlined in the SNP MOC. SNP members are assigned to a NCM within their service area. NCMs take the lead in the responsibly of forming the ICTs for SNP members. ICTs will at a minimum and whenever feasible include the assigned NCM, the SNP member and/or primary caregiver and the member’s PCP. The final Element E of MOC 2 addresses Care Transitions Protocols. ATRIO has adopted the following CMS definitions used to explain care transitions: Health care settings: The provider from whom or setting where a member receives health care and health-related services. In any setting, a designated practitioner has ongoing responsibility for a member’s medical care. Transition: Movement of a member from one care setting to another as the member’s health status changes. For example, moving from home to a hospital as the result of an exacerbation of a chronic condition or moving from the hospital to a rehabilitation facility after surgery. Transitions process: The period of identification of a member who is at risk for a care transition through completion of a transition. This process includes planning and preparation for transitions and the follow-up care after transitions are completed. ATRIO makes special effort to coordinate care when SNP members move from one health care setting to another, such as when they are discharged from a hospital. Without coordination, such transitions often result in fragmented and unsafe care for the older or disabled and particularly vulnerable SNP beneficiary. ATRIO’s Transitions of Care program is designed with the intent to minimize risks associated with health care transitions. ATRIO delegates the responsibility of coordination of the care transitions processes to the SAC assigned NCMs. Each SAC is responsible to follow the specific ATRIO TOC policy and procedure (located within the SNP CM Policy and Procedure) as well as the framework outlined in the SNP MOC. The case management software serves as the central location for the documentation of care management and care coordination activities including the care transitions processes. MOC 3: Provider Network The SNP provider network is a network of health care providers who are contracted to provide health care services to SNP beneficiaries. SNPs must ensure that their MOC identifies, fully describes and implements the following element for their SNP provider network: Specialized Expertise, Use of Clinical Practice Guidelines and Care Transitions Protocols and MOC Training for the Provider Network. ATRIO has established a vast network of providers and healthcare facilities allowing the Plan to provide exceptional access and care services to the often vulnerable SNP beneficiaries. ATRIO regards the primary care provider (PCP) as the expert in determining the health care needs of the SNP beneficiary. Each SNP member is required to have an identified PCP and our SAC NCMs, Customer Service Representatives and Provider Relations staff make special effort to match SNP members with a PCP they can be most aligned and satisfied with. In addition to our extensive network of primary care providers ATRIO has established an equally robust network of specialty and ancillary care providers for our SNP members. These include: Medical Specialists: Allergy & Immunology, Anesthesiology, Audiology, Cardiology, Chiropractic, Dermatology, Dietary, Endocrinology, Gastroenterology, Gerontology, Gynecology, Infectious Disease, Nephrology, Neurology, Obstetrics/Gynecology, Oncology, Ophthalmology, Oral Surgeon, Orthopedics, Otolaryngology, Pain Management, Podiatry, Psychiatry, Pulmonology, Rheumatology, and Urology Behavioral & Mental Health: Drug Counselors, Clinical Psychologists, Licensed Clinical Social Workers and other mental health professionals Nursing professionals: Registered Nurse and Nurse Practitioners Allied Health Professionals: Pharmacies, Physical Therapists, Occupational Therapists, Speech Therapists, Pathology, Radiology Specialists and Hospice care givers and coordinators Facilities: Inpatient, Outpatient, Rehabilitative, Long Term Care, Psychiatric, Laboratory, Radiology/Imaging, Dialysis, Home Health, Urgent Care, Durable Medical Equipment Supplier. MOC 4: MOC Quality Measurement and Performance Improvement The goal of performance improvement and quality measurement is to improve the SNP’s ability to deliver highquality health care services and benefits to its SNP beneficiaries. Plan leadership, managers and governing bodies of the SNP organization must have a comprehensive quality improvement program in place to measure its current level of performance and determine if organizational systems and processes must be modified, based on performance results. ATRIO has a quality improvement process by which various data sets collected from multiple sources are used to evaluate, measure, stratify and report on the Plan’s Full-Dual Special Needs Plan Model of Care. The Quality Assurance Committee with authority from the Board of Directors is responsible for monitoring and evaluating the SNP MOC effectiveness. The QA Committee is charged with: • Recommend outcomes to be monitored and establish benchmarks for ongoing monitoring and oversight of the SNP MOC. • Evaluate the timeliness and response rate of the HRAs for SNP beneficiaries’ participation in the creation/management of individualized care plans. • Annually evaluate the associated HEDIS, CAHPS and HOS data results • Assist in the identification of the most vulnerable SNP beneficiaries • Evaluate the Plan’s ability to effectively communicate the results and effectiveness of the MOC to all stakeholders and recommend enhanced training if need be. • Recommend improvements to the SNP MOC and the evaluation process ATRIO’s MOC measurable goals and health outcomes revolve around the areas of access to care services, affordability, coordination of care, care transitions and utilization of services for preventative health and chronic conditions. The following are ATRIO’s current measurable goals: Measurable Goal—ATRIO will achieve a score of ≥ 87% (est. 5 star level) on annual CAHPS results for the following questions. • Ease of getting an appointment with a specialist • Getting care, tests, or treatment necessary Measurable Goal—ATRIO will achieve a ≥ 99% (est. 5 Star level) for the MPF (Medicare Pharmacy Finder) price accuracy measure. Measurable Goal—ATRIO will achieve a score of ≥87% (est. 5 star level) on annual CAHPS results for the following questions • • • • Doctor had medical records or other information about your care Doctor talked about prescription medicines Got help managing care Doctor informed and up-to-date about specialty care Measureable Goal—ATRIO will achieve a ≥80% return rate (est. 5 star level) for the HRA return rate (SNP Care Management Star Measure) Measurable Goal—ATRIO will achieve <9% (est. 4 star level) for Plan All-Cause Readmissions (readmissions to a hospital within 30 days of being discharged) Measureable Goal-- ATRIO will achieve ≥80% of diabetic SNP members whose most recent HbA1c level is less than or equal to 9% (est. 4 star level) Measurable Goal—ATRIO will achieve a ≥60% (est. 4 star level) for Osteoporosis Management. ATRIO operates under a continual process of quality improvement for all of our programs and especially those directly involving our most vulnerable SNP members. ATRIO’s QA Committee and SNP Leadership prioritize mechanisms of improvements to the SNP MOC and respond to lessons learned and implement those improvements in as timely a manner as possible with the end goal of assisting our SNP members in achieving the highest level of quality care. For more information on any of the topics included here please refer to ATRIO’s full copy of the SNP MOC. If you do not currently have a copy of ATRIO’s SNP MOC and would like one for your reference please make a request from ATRIO’s SNP Program Manager who can be reached via ATRIO’s Customer Service Department at 1-877-672-8620. Customer Services hours are Monday-Friday 8 am- 5 pm Pacific Time Questions & Answers??????