Saman Hazany, MD¹², Daljit Mann (co-first author
advertisement

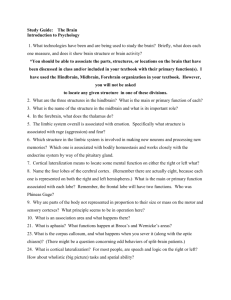
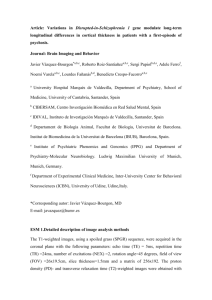
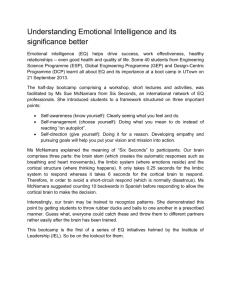
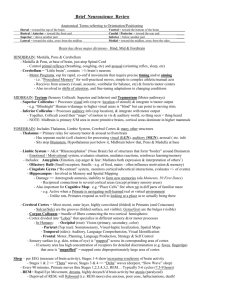
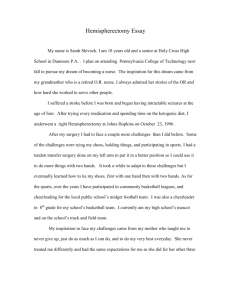
Changes in Neuroimaging as Result of Robotic Rehabilitation in Patients with Hemispherectomy Abstract #: EP-126 SAMAN HAZANY, MD¹², DALJIT MANN (CO-FIRST AUTHOR), BS²³; MINDY AISEN, MD¹²; STELLA DE BODE, PHD4; SUSAN SHAW, MD¹²; KRISTI CLARK, PHD³ 1. RANCHO LOS AMIGOS NATIONAL REHABILITATION CENTER. DOWNEY, CA. 2. UNIVERSITY OF SOUTHERN CALIFORNIA (USC). LOS ANGELES, CA. 3. INSTITUTE FOR NEUROIMAGING AND INFORMATICS (INI) – USC. LOS ANGELES, CA. 4. UNIVERSITY OF CALIFORNIA LOS ANGELES. LOS ANGELES, CA. Disclosure statement The authors of this electronic poster have no relevant financial relationships to disclose. Purpose To investigate anatomic changes in the brain (specifically cortical thickness changes) as a result of robotic rehabilitation in patients with hemispherectomy, by using structural MRI. Introduction Hemispherectomy is generally performed in patients with intractable – drug-resistant epilepsy secondary to conditions including perinatal stroke, hemimegalencephaly, multilobar cortical dysplasia, Rasmussen encephalitis, and Sturge-Weber syndrome. This procedure improves seizure control, however leads to sensorimotor deficits, visual, language and behavioral impairments[1, 2]. Many studies have shown residual motor function in the contralateral extremities after hemispherectomy [3, 4]. Areas of increased FDG uptake have been seen in posthemispherectomy subjects while performing a motor task in multiple places: premotor area, SMA, Secondary sensory area, and lingual gyrus[5]. Introduction Task-oriented training increases gray matter and white matter in healthy human brains [6, 7, 8]. Functional MRI study has shown functional sensorimotor cortex reorganization in the contralateral hemisphere with subjective improvements in behavior in setting of task-oriented locomotor rehabilitation [9]. Other studies have shown that motor skill learning is associated with structural brain plasticity, and that practice time and performance modulate the extent of structural brain changes evoked by long term training [10]. No other studies have looked at different methods of rehabilitation. The aim of this study is to investigate the efficacy of a 2 week high intensity rehabilitation program with help of robotics, by correlating changes in cortical thickness to fugl-meyer scores. Materials and Methods Patients 5 female patients with right-sided hemispherectomy; all right-handed (except one subject who was too young at time of surgery to determine handedness) with an average age of 10.8 years (Range: 10-12 years) at the time of therapy. The average age at first hemispherectomy surgery was 5.05 years (range: .25 – 9 years). List of diagnoses that led to hemispherectomy: Rasmussen’s Encephalitis Sturge-Weber Syndrome brain trauma secondary to prior neurosurgery Taylors Type 2 Cortical Dysplasia. Materials and Methods Training All subjects were enrolled in a high-intensity task-oriented robotic rehabilitation program for two weeks with four consecutive days each week. Subjects received three hours per day of robot-assisted therapy, consisting of one hour of Hocoma Lokomat, one hour of Interactive Motion Technologies (IMT) ARM, and one hour of IMT Anklebot training. All subjects also participated in value-added activities consisting of one hour per day of recreational therapy, one hour per day of adaptive yoga, one hour per day of virtual reality occupational therapy, and one hour per day of miscellaneous fun activities which included ice cream social, dance, making slime, and movies. Two subjects (1 and 2) also received an additional one hour of training with wrist robot, focusing on wrist flexion, wrist extension, ulnar deviation and radial deviation. The wrist training occurred on the same days as the other robotic training, however HW participated in the wrist training for 7 days while AM participated all 8 days. Fugl-Meyer assessment of physical performance (used in previous studies[1–3]) was also applied in this study to assess behavioral changes in upper extremity motor function before and after the therapy. Materials and Methods MRI scan: 3D FSPGR (fast spoiled gradient echo) magnetic resonance imaging of each subject was performed 1 day before and 1 day after period of two weeks training on a General Electric (GE) Signa HDx 1.5 Tesla MRI scanner at Rancho Los Amigos National Rehabilitation Center located in Downey, California, United States with the following parameters: TR: 9.3 msec TE: 3.7 msec Flip Angle: 13 NEX: 1 Field of view: 24 x 26.8 cm Matrix: 256 x 256 Slice thickness: 1 mm with no space Number of slices in sagittal direction : variable (about 200) Materials and Methods Image post-processing and analysis: Image post processing was performed at Institute for Neuroimaging and Informatics (INI); University of Southern California (USC) located in Los Angeles, California, United States. Each subject had different amounts of their right hemisphere removed during surgery . In order to process images with the analysis software, the whole hemisphere was duplicated and flipped and final analyses were run focusing on the intact left hemisphere. Free-surfer was used to estimate a two-timepoint change in brain volume by aligning the two brain images and performing tissue-type segmentation to find brain/non-brain edge points. Next, perpendicular edge displacement between the two timepoints was calculated and the mean displacement was converted into an estimated cortical thickness change. Finally, a group paired t-test was used to calculate an average change in cortical thickness across all five patients. Figure1: Example subject before and after hemisphere duplication. Results Upper extremity fugl-meyer score changes following training Subject number Before training After training Difference 1 31 38 +7 2 22 22 0 3 21 24 +3 4 21 23 +2 5 20 21 +1 Results Figure 2 demonstrates average results of all 5 subjects with red color representing areas of increased cortical thickness, and blue color representing areas of decreased cortical thickness when comparing pre-training to post-training 3D FSPGR MRI sequences. Images are inflated to expand the sulci. Gyri appear light gray and inflated sulci appear dark gray. The clusters indicated by the arrows are in locations including the Supplementary Motor Area and PreMotor Area (16, 35, 42), central sulcus near hand knob (33) and Sensory Associative Zones (26). Figure 2. Subject 1 Figure 3: Increased cortical thickness is observed in the sensory associative areas (a) with biggest contribution to cluster 42 (b). Figure 3a. Figure 3b. Subject 2 Figure 4: Increased cortical thickness is observed in the sensory cortex and sensory associative areas (a) with biggest contribution to clusters 33 and 26 (b). Figure 4b. Figure 4a. Subject 3 Figure 5: Increased cortical thickness is observed in the motor cortex, sensory cortex and sensory associative areas (a) with biggest contribution to clusters 26 and 42 (b). Figure 5a. Figure 5b. Subject 4 Figure 6: Increased cortical thickness is observed in the motor cortex including the hand knob, sensory cortex and sensory associative areas (a) with biggest contribution to clusters 26, 33, and 42 (b). Figure 6a. Figure 6b. Subject 5 Figure 7: Minimal increased cortical thickness is observed in the sensory associative areas (a) with small contribution to clusters 26, 33, 42 (b). Figure 7b. Figure 7a. Limitations Small number of subjects makes drawing statistical conclusions unreliable. We do not have an explanation for areas of decrease in cortical thickness. Motor outcomes of hemispherectomy patients after therapy is highly variable, and the recovery mechanisms and results will depend on factors like structural properties of the lesion itself, the age at which it was acquired, the exact pre-operateive level of functioning, and the effects of the intractable seizures on the remaining hemisphere [9]. Discussion and conclusions Our average results show increase in cortical thickness in supplementary motor area, pre-motor area, and sensory associative zones which is in agreement with previous studies [5, 9, 11] These older studies have shown only functional reorganization using fMRI BOLD or PET imaging and our findings support older studies with physical increases in cortical thickness underlying the same areas. Prior view that higher order cortical areas have an increased capacity for sensorimotor reorganization than primary motor areas [5] is supported by our findings. Discussion and conclusions This study shows an objective physical increase in cortical thickness that coincides with behavioral improvements proven with increases in upper extremity fugl-meyer score. These findings support the notion that intensive training, for as little as two weeks, may induce cortical changes years after hemispherectomy. References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. Liégeois F1, Connelly A, Baldeweg T, Vargha-Khadem F. Speaking with a single cerebral hemisphere: fMRI language organization after hemispherectomy in childhood. Brain Lang. 2008 Sep;106(3):195-203. doi: 10.1016/j.bandl.2008.01.010. Epub 2008 Mar 7. Moosa AN, Jehi L, Marashly A, Cosmo G, Lachhwani D, Wyllie E, Kotagal P, Bingaman W, Gupta A. Long-term functional outcomes and their predictors after hemispherectomy in 115 children. Epilepsia. 2013 Oct;54(10):1771-9. doi: 10.1111/epi.12342. Epub 2013 Aug 23.) De Bode S1, Firestine A, Mathern GW, Dobkin B. Residual motor control and cortical representations of function following hemispherectomy: effects of etiology. J Child Neurol. 2005 Jan;20(1):64-75. Zhang J, Mei S, Liu Q, Liu W, Chen H, Xia H, Zhou Z, Wang L, Li Y. fMRI and DTI assessment of patients undergoing radical epilepsy surgery. Epilepsy Res. 2013 May;104(3):253-63. doi: 10.1016/j.eplepsyres.2012.10.015. Epub 2013 Jan 20. Bernasconi A, Bernasconi N, Lassonde M, Toussaint PJ, Meyer E, Reutens DC, Gotman J, Andermann F, Villemure JG. Sensorimotor organization in patients who have undergone hemispherectomy: a study with (15)O-water PET and somatosensory evoked potentials. Neuroreport. 2000 Sep 28;11(14):3085-90. Bezzola L1, Mérillat S, Gaser C, Jäncke L.Training-induced neural plasticity in golf novices. J Neurosci. 2011 Aug 31;31(35):12444-8. doi: 10.1523/JNEUROSCI.1996-11.2011. Boyke J, Driemeyer J, Gaser C, Büchel C, May A. Training-induced brain structure changes in the elderly. J Neurosci. 2008 Jul 9;28(28):7031-5. doi: 10.1523/JNEUROSCI.0742-08.2008. Hofstetter S1, Tavor I, Tzur Moryosef S, Assaf Y. Short-term learning induces white matter plasticity in the fornix. J Neurosci. 2013 Jul 31;33(31):12844-50. doi: 10.1523/JNEUROSCI.4520-12.2013. de Bode S, Mathern GW, Bookheimer S, Dobkin B. Locomotor training remodels fMRI sensorimotor cortical activations in children after cerebral hemispherectomy. Neurorehabil Neural Repair. 2007 Nov-Dec;21(6):497-508. Epub 2007 Mar 16. Sampaio-Baptista C, Scholz J, Jenkinson M, Thomas AG, Filippini N, Smit G, Douaud G, Johansen-Berg H. Gray matter volume is associated with rate of subsequent skill learning after a long term training intervention. Neuroimage. 2014 Aug 1;96:158-66. doi: 10.1016/j.neuroimage.2014.03.056. Epub 2014 Mar 26. Graveline CJ, Mikulis DJ, Crawley AP, Hwang PA (1998) Regionalized sensorimotor plasticity after hemispherectomy fMRI evaluation. Pediatr Neurol 19:337–342. doi: 10.1016/S0887-8994(98)00082-4