FIN – 2100 CPT Coding – Evaluation and Management Services
advertisement

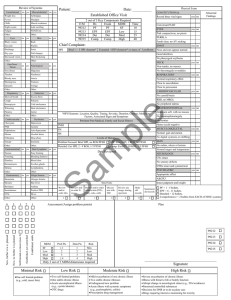
POLICY: EVALUATION AND MANAGEMENT: GENERAL GUIDELINES Policy Number: FIN – 2100 Page(s): 1 of 2 Approved by: Effective Date: PURPOSE: Evaluation and Management Services are some of the most misused and improperly coded services utilized in all healthcare practices. POLICY: Follow 1995 Guidelines for coding E/M Services to ensure that all services are properly documented and that documentation supports the level of service that is billed to insurance carriers. New Patient Any patient who has not been seen in the practice in the previous three years by a physician of the same specialty Codes 99201 through 99205 Established Patient Any patient who returns to the office that HAS been treated by a physician of the same specialty within the past three years. Codes 99211 through 99215 Seven Components of E/M Services 1. History 2. Examination 3. Medical Decision Making 4. Counseling 5. Coordination of Care 6. Nature of Presenting Illness 7. Time (least important in determining level of service) Key Components are the History, Examination, and Clinical Decision Making as these are the primary factors used to determine the level of service to be billed for. When coding for E/M services, the charts and decision making tool on the following pages will be utilized, depending on whether the service is for a “new” or “established” patient. Evaluation and Management Decision Tool NOTE: This tool is based on 1995 Documentation Guidelines for Evaluation and Management Services (DGs) by CMS. New Patient – Patient is new to your office or has NOT been seen in the past 3 years by you or someone else in your practice with the same specialty or subspecialty. ALL E/M code levels require a Chief Complaint. E/M Code History (Requires 3 of 3) Exam MDM Time Level HPI ROS PFSH 1-3 N/A N/A 1 Straightforward 10+ min 99201 1-3 1 N/A 2-7 Straightforward 20+ min 99202 4+ 2-9 1 2x-7x Low 30+ min 99203 4+ 10+ 3 8+ Moderate 45+ min 99204 4+ 10+ 3 8+ High 60+ min 99205 NOTE: Requires 3 of 3 key factors (History, Exam, MDM) to be met or exceeded. Time is ONLY considered the determining key factor when 50% or more is spent on counseling and/or coordination of care and documented appropriately. Established Patient – You, or someone else in your practice with the same specialty or subspecialty have seen the patient in the past 3 years. ALL E/M code levels require a Chief Complaint. E/M Code History (Requires 2 of 3) Exam MDM Time Level HPI ROS PFSH N/A N/A N/A N/A N/A 5+ min 99211 1-3 N/A N/A 1 Straightforward 10+ min 99212 1-3 1 N/A 2-7 Low 15+ min 99213 4+ 2-9 1 2x-7x Moderate 25+ min 99214 4+ 10+ 2+ 8+ High 40+ min 99215 NOTE: Requires 2 of 3 key factors (History, Exam, MDM) to be met or exceeded. Time is ONLY considered the determining key factor when 50% or more is spent on counseling and/or coordination of care and documented appropriately. HISTORY History of Present Illness (HPI) Elements A chronological description of the development of the patient’s present illness from the first sign and/or symptom or from the pervious encounter to the present. It includes: Location Quality, Severity, Duration, Timing, Context, Modifying Factors, and Association Signs and Symptoms. Review of Systems (ROS) Elements An inventory of body systems obtained through a series of questions seeking to identify signs and/or symptoms, which the patient may be experiencing or has experienced. The following systems are recognized: Constitutional (e.g. fever, weight loss), Eyes, Ears/Nose/Mouth/Throat, Cardiovascular, Respiratory, Gastrointestinal, Genitourinary, Musculoskeletal, Integumentary (skin and/or breast), Neurological, Psychiatric, Endocrine, Hematologic/Lymphatic, Allergic/Immunologic Past, Family, and/or Social History (PFSH) Elements PFSH consists of a review of 3 areas: 1. Past history (patient’s past experiences with illnesses, operations, injuries, and treatments); 2. Family History (review of medical events in patient’s family, including diseases which may be hereditary or place the patient at risk); and 3. Social History (age appropriate review of past and current activities) EXAMINATION For purposes of examination, the following body areas are recognized: Head (including face), Neck, Chest (including breast and axilla), Abdomen, Genitalia/Groin/Buttock, Back (including spine), Each Extremity For purposes of examination, the following organ systems are recognized: Eyes, Ears/Nose/Mouth/Throat, Cardiovascular, Respiratory, Gastrointestinal, Genitourinary, Musculoskeletal, Skin, Neurologic, Psychiatric, Hematologic/Lymphatic/Immunologic COMPLEXITY of MEDICAL DECISION MAKING (MDM) The levels of E/M services recognize four types of MDM (straightforward, low complexity, moderate complexity, and high complexity) and require 2 of 3 elements listed below to be met or exceeded: 1. Number of possible Diagnoses and/or number of management options that must be considered; 2. Amount and/or complexity of medical records, diagnostic tests, and/or other information that must be obtained, reviewed and analyzed; and 3. Risk of significant complications, morbidity and/or mortality as well as comorbidities, associated with the patient’s presenting problem(s), the diagnostic procedure(s) and/or the possible management options.