20150312iPScellPancreasBetaCell
advertisement

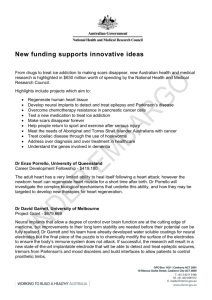
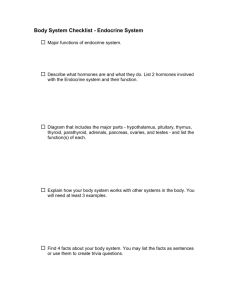
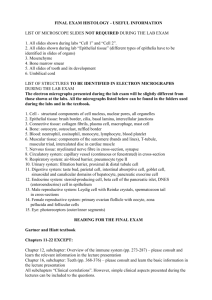
Journal Club Toyoda T, Mae SI, Tanaka H, Kondo Y, Funato M, Hosokawa Y, Sudo T, Kawaguchi Y, Osafune K. Cell aggregation optimizes the differentiation of human ESCs and iPSCs into pancreatic bud-like progenitor cells. Stem Cell Res. 2015 Jan 28;14(2):185-197. doi: 10.1016/j.scr.2015.01.007. Choi JA, Ko SH, Park YR, Jee DH, Ko SH, Park CK. Retinal Nerve Fiber Layer Loss Is Associated with Urinary Albuimin Excretion in Patients with Type 2 Diabetes. Ophthalmology. 2015 Feb 6. pii: S0161-6420(15)00003-2. doi: 10.1016/j.ophtha.2015.01.001. 2015年3月12日 8:30-8:55 8階 医局 埼玉医科大学 総合医療センター 内分泌・糖尿病内科 Department of Endocrinology and Diabetes, Saitama Medical Center, Saitama Medical University 松田 昌文 Matsuda, Masafumi Organogenesis of the murine pancreas. The pancreatic bud begins around day 9 of gestation (E9.5) in the mouse embryo. At E11.5 the pancreatic ductal epithelium grows and branches into the surrounding mesenchyme. The epithelial cells differentiate into exocrine and endocrine cells at E15.5. Ductal, acinar, and islet cells are clearly found by E18.5. Front. Physiol., 18 July 2013 | doi: 10.3389/fphys.2013.00170 Pancreatic cell lineage and the role of transcription factors during islet cell type development. All mature pancreatic cell types are derived from progenitors that express Pdx-1 and/or Ptf1a. Mnx-1 and Mib-1 act to regulate notch ligand activity. Ngn3 expression in pancreatic progenitor cells gives rise to ductal, acini, and endocrine progenitor cells. Nkx2.2 and Nkx6.1 work alongside other transcription factors including PDX-1, MafA Mnx1, Isl1 and NeuroD1 to regulate the formation of the majority of islet β-cells. Front. Physiol., 18 July 2013 | doi: 10.3389/fphys.2013.00170 Transcription factors Pdx-1. Pancreatic duodenal homeobox 1 (Pdx-1) is one of the first transcription factors expressed, with gene expression starting as early as E8.5 in the mouse in the foregut endoderm (Offield et al., 1996). All the cells derived from the endoderm have been shown to express Pdx-1 (Gu et al., 2002). Both the ventral and dorsal pancreatic buds express Pdx-1 at E9.5 (Offield et al., 1996). At approximately E10 expression of Pdx-1 mRNA is then downregulated with expression becoming restricted only to endocrine cells in the pancreas and this is maintained in adult β-cells (Ohlsson et al., 1993; Ahlgren et al., 1998). Pdx-1 itself is an essential mediator of mesenchymal signaling, necessary for the branching morphogenesis involved in ductal network formation of the pancreas at E10.5 (Ahlgren et al., 1996). Germline knockout studies have shown that while knockdown of Pdx-1 prior to E10.5 has no effect on pancreatic developmental processes (Wescott et al., 2009), the targeted pancreatic deletion at E10.5 or later results in pancreatic agenesis (Ahlgren et al., 1996; Offield et al., 1996). Pdx-1 contains three principal transcription initiation sites (Sharma et al., 1996) and in the β-cell each of these sites may be activated by the binding of a specific set of transcription factors (Melloul et al., 2002); FOXA2, HNF6, PTF1a, MNX-1, MAFA, HNF, SP1/3, USF1/2 and PDX-1 itself (Harrison et al., 1999; Melloul et al., 2002; Jacquemin et al., 2003; Gao et al., 2008; Vanhoose et al., 2008). Interestingly, reduced expression of the PDX-1 gene within the human pancreas has been linked with type 2 diabetes, a rare autosomal dominant form of type 2 diabetes called maturity onset diabetes of the young (MODY4) and pancreatic agenesis (Lin and Vuguin, 2012). Ptf1a/p48. Ptf1a (pancreas specific transcription factor 1a/p48) is a basic helix-loop-helix (bHLH) transcription factor (Beres et al., 2006). It was first identified as a subunit of the trimeric PTF1 transcription factor complex, and has been found to be crucial for the regulation of exocrine gene transcription (Ohlsson et al., 1993; Krapp et al., 1996). Endodermal expression of Ptf1a/p48 is pancreas specific throughout development; being expressed in endocrine, exocrine and ductal cell types (Kawaguchi et al., 2002). PTF1a protein has been detected as early as E8–8.75 in the ventral and dorsal pancreatic ducts (Hald et al., 2008) but by E13.5 expression becomes restricted to acinar precursor cells (Kawaguchi et al., 2002). In adult rodents, PTF1a/p48 transcription factor protein is expressed in acinar tissue and induces amylase and elastase gene expression. While a deficiency in PTF1a/p48 protein does not inhibit the initial formation of the pancreas it does cause a complete lack of acinar cell development (Krapp et al., 1998; Kawaguchi et al., 2002). Cell lineage studies have shown that this is through cells adopting an intestinal fate rather than becoming cells within the ventral pancreas (Kawaguchi et al., 2002). Defects in the human PTF1a protein are associated with permanent neonatal diabetes mellitus (Masui et al., 2007). It has recently been suggested that Ptf1a-mediated control of Delta-like ligand 1 (Dll1) expression is crucial for Notchmediated control of early pancreas development (Ahnfelt-Ronne et al., 2012). The Ptf1a activation of Dll1 within multipotent progenitor cells (MPC) stimulates proliferation and pancreas growth by maintenance of HES1 (hairy and enhancer of split 1) expression and PTF1a protein levels (AhnfeltRonne et al., 2012). Endocrine lineage specification Differentiation of the cells into each endocrine cell type found within the islet of Langerhans begins at specific time points during embryogenesis. For αcells this is E9.5, for β-cells E10.5, for δ-cells at E14.5 and lastly PP cells at E18.5. The critical window of differentiation of endocrine cells in humans is from weeks 7 to 23 of gestation (Lin and Vuguin, 2012). Glucagon-producing α-cells are found at week 7, followed by insulin-producing β-cells, somatostatin-producing δ-cells and pancreatic polypeptide PP cells at weeks 8–10 gestation (Lin and Vuguin, 2012). Importantly, the processes that control the development of each cell type are governed by a complex signaling cascade. Front. Physiol., 18 July 2013 | doi: 10.3389/fphys.2013.00170 Notch cell signaling. The notch cell signaling pathway is a well-conserved signaling pathway that regulates cell fate determination during embryonic development as well as the maintenance of tissue homeostasis during adult life (Bigas and Espinosa, 2012). During development Notch signaling must be regulated to balance the expansion of the progenitor pool with the differentiation of mature cell types (Greenwood et al., 2007), with genetic perturbations of this pathway resulting in a change in pancreatic cell fate (Apelqvist et al., 1999). Notch-mediated signaling ensures the appropriate maintenance of the progenitor cell population through the activation of the bHLH factor Hes1 (Jensen et al., 2000). Loss-of-function experiments have shown that Notch signaling promotes pancreatic progenitor cell self-renewal and/or exocrine lineage commitment (Murtaugh et al., 2003). A reduction in Notch signaling increases the expression of the pro-endocrine gene Ngn3, promoting an endocrine fate; while those cells exposed to Notch signaling express Hes-1 and p48 mRNA and adopt an exocrine fate (Apelqvist et al., 1999). Ngn3. Neurogenin 3 (NGN3) is one of the most important transcription factors for endocrine development. All endocrine cell types are derived from progenitor cells expressing the Ngn3 gene (Gu et al., 2002). The bHLH transcription factor is expressed in two distinct waves (Villasenor et al., 2008). The first phase of Ngn3 expression begins in murine pancreatic progenitor cells at E8.5–9 resulting in glucagon producing cells, while the second begins at E12 with expression peaking at E15.5 corresponding with endocrine cell differentiation (Gradwohl et al., 2000; Schwitzgebel et al., 2000). Ngn3 null animals are born without islets, and lack all endocrine cell types, develop type 1 diabetes and die 1–3 days after birth (Gradwohl et al., 2000). Ngn3 has been associated with several downstream factors involved in endocrine differentiation and cell subtype specification and maintenance, including Nkx2.2, Nkx6.1, Pax4 Isl1, b2/NeuroD1, Pax6 and Pdx-1 (Huang et al., 2000; Smith et al., 2003; Collombat et al., 2005). Pax4—Arx. The paired box containing gene 4 (Pax4) mRNA is first detected at E9.5 and is transiently expressed in all endocrine progenitors during pancreatic development, being downregulated shortly after birth (Lin and Vuguin, 2012). Pax4 is expressed downstream of Ngn3, with expression being lost in Ngn3 null mice but not vice versa (Gradwohl et al., 2000; Wang et al., 2004). Pax4 activity appears essential for the appropriate initiation of β-cell differentiation (Collombat et al., 2005). In the absence of Pax4, β- and δ-cells fail to develop and more α- cells are observed (Collombat et al., 2003, 2005; Sosa-Pineda, 2004). The loss of Pax4 prevents the expression of Pdx-1, HB9 and insulin mRNA in β-cell precursors (Wang et al., 2004). PAX4 has an opposing action to the transcription factor aristaless-related homeobox gene (ARX) (Collombat et al., 2003). Arx gene expression begins at E9.5 during mouse pancreatic development and persists into mature α-cells (Collombat et al., 2003). Arx null mice lack α-cells despite having no changes in total islet cell number (Collombat et al., 2005). Therefore, it is the balance of Pax4 and Arx that is crucial for cell fate determination of both α- and βcells within the islet (Collombat et al., 2005). Nkx. Members of the NK homeodomain transcription factor family are critical regulators of organ development (Stanfel et al., 2005). Of these, Nkx2.2 and Nkx6.1 are involved in endocrine cell lineage and are likely to be the most important during pancreatic development. Nkx2.2 NKX2.2 is able to bind to both the insulin and Pax4 promoters (Cissell et al., 2003). The Nkx2.2 gene is initially dorsally expressed with Pdx-1 at E8.75 and ventrally at E9.5 (Jorgensen et al., 2007). However, by E15.5 its expression becomes restricted to only endocrine cells (Sussel et al., 1998). Nkx2.2 deficiency results in a reduction of α- and PP-cells, and the complete loss of β-cells (Sussel et al., 1998) and in the absence of Nkx2.2, β-cells fail to activate insulin gene transcription and lack Nkx6.1, suggesting that Nkx2.2 is essential for the specification of the mature β-cell phenotype (Sussel et al., 1998). Front. Physiol., 18 July 2013 | doi: 10.3389/fphys.2013.00170 Nkx6.1 Nkx6.1 pancreatic gene expression is similar to that of Nkx2.2. In mouse models Nkx6.1 is expressed in the prospective ventral pancreas domain at E8.75. By E9.0 Nkx6.1 expression switches from the ventral domain to the dorsal domain until E10.5, when ventral expression of Nkx6.1 reappears (Jorgensen et al., 2007) and then by E11.5, its expression becomes restricted to the central epithelium (Jorgensen et al., 2007). In adult murine islets, Nkx6.1 expression is restricted to β-cells (Jensen et al., 1996) where it suppresses glucagon expression and modulates glucose stimulated insulin secretion (Schisler et al., 2005). Nkx6.1 acts downstream of Nkx2.2 (Sussel et al., 1998) Not only do Nkx2.2 single mutant animals lack expression of Nkx6.1 within the β-cell (Sussel et al., 1998) but the Nkx6.1 promoter contains a conserved binding site for Nkx2.2 (Sander et al., 2000). In fact, Nkx6.1 deficiency does not affect early pancreas development, but it does result in compromised β-cell development (Sander et al., 2000) and mutant animals lacking both Nkx2.2/Nkx6.1 have a phenotype identical to that of Nkx2.2 knockout animals (Sander et al., 2000). Maintenance of β-cell identity NeuroD1/Beta2. NeuroD1/Beta2, a bHLH, is first expressed in mouse pancreatic cells from E9.5 (Naya et al., 1997). By E12.5, NeuroD1/Beta2 mRNA is found in both dorsal and ventral pancreatic buds and from E17.5 gene and protein expression is restricted to small clusters of endocrine cells and is rarely detected in ductal epithelial cells (Chu et al., 2001). In adult islets, NeuroD1/Beta2 is expressed in all endocrine cells of the islet, although its function still remains unknown. While it is believed that NeuroD1/Beta2 plays a role in regulating insulin (Sharma et al., 1999) and glucagon mRNA expression, mice lacking NeuroD1/Beta2 are still able to produce functional insulin and glucagon (Chu et al., 2001). Large Maf transcription factors. The Maf family of transcription factors belong to the basic leucine-zipper (bZIP) family that have been associated with the regulation of a number of differentiation processes (Hang and Stein, 2011). The Maf family is divided into two groups (small and large) based on their molecular size (Hang and Stein, 2011). The large Maf proteins MAFA, MAFB, c-MAF and NRL contain a transactivation domain in the N-terminal region and are key regulators of cellular differentiation (Yang and Cvekl, 2007; Hang and Stein, 2011). In adult islets, MAFA, MAFB, and c-MAF are expressed unlike NRL (Matsuoka et al., 2003), supporting a role for NRL in islet cell development. MafA. MafA gene expression starts at E13.5 and continues throughout adulthood in the mouse (Matsuoka et al., 2003). MafA knockout mice display no changes in pancreas development, but the mice do go on to develop glucose intolerance and type 2 diabetes as a result of reduced β-cell mass and increased β-cell apoptosis (Zhang et al., 2005). Furthermore, MAFA binds to the insulin promoter and through its interaction with PDX-1 and NEUROD1, activates insulin gene transcription (Olbrot et al., 2002; Aramata et al., 2005). MafB. In the adult mouse pancreas MafB is expressed within the islet α-cells where it regulates glucagon gene expression (Artner et al., 2006, 2007). Expression of MafB mRNA within the mouse pancreas begins as early as E10.5 in glucagon-positive cells, before expression in islet positive cells at E12.5 (Artner et al., 2006). MafB becomes progressively restricted to α-cells postnatally through the downregulation of its expression in β-cells in the first 2 weeks after birth and its expression is undetectable in these cells 3 weeks after birth (Artner et al., 2007). MAFB plays a pivotal role in the development and differentiation of α- and β-cells during pancreatogenesis by directly affecting the transcription of specific genes present in α- or βcells as opposed to genes which are more ubiquitously expressed in other islet cell types (e.g., Pax6, Isl1 and NeuroD1) (Artner et al., 2007). Mib-1. Mind bomb 1 (Mib-1) encodes an E3 ubiquitin ligase essential for Notch ligand activity (Itoh et al., 2003) that is required for correct proximodistal patterning in the developing pancreas as well as in β-cell formation Horn et al., 2012). Endodermal-specific inactivation of Mib-1 causes the proximal cells of the developing pancreas to adopt a distal fate resulting in a reduction in β-cells (Horn et al., 2012). Front. Physiol., 18 July 2013 | doi: 10.3389/fphys.2013.00170 Mnx-1. The homeodomain transcription factor MNX1 (HB9) plays a key role in pancreatic development and function (Harrison et al., 1999; Li et al., 1999; Dalgin and Prince, 2012). Murine Mnx-1 gene expression begins at E8 (Lin and Vuguin, 2012). Work in zebrafish suggests that Mnx-1 may suppress α- cell fate in β-cell precursors (Dalgin and Prince, 2012). Furthermore, Mnx-1 knockout mice fail to develop the dorsal lobe of the pancreas with the remnant pancreas having smaller islets of Langerhans with reduced β-cell numbers expressing low levels of Glut2 and Nkx6.1 (Harrison et al., 1999). Lbl-11/Isl-1. The transcriptional regulator Islet-1 (Isl-1) gene is expressed in the developing mouse pancreas at E8–8.5 (Lin and Vuguin, 2012) but is later restricted only to the endocrine cells of adult islets, where it is involved in the maturation, proliferation and survival of the second wave of islet cells (Du et al., 2009). Isl-1 directly regulates MafA, a potent regulator of the insulin gene and β-cell function (Du et al., 2009). Isl-1 deficient animals fail to develop functional β-cells, and have a reduced ability to expand their endocrine cell mass postnatally and consequently become diabetic (Du et al., 2009). A nonsense mutation of the ISL-1 gene has been found in a case of human type 1 diabetic patient. Activation of Isl-1 is regulated in part by the transcriptional co-regulator, LIM domain-binding protein 1 (LBL-1) (Hunter et al., 2013). Front. Physiol., 18 July 2013 | doi: 10.3389/fphys.2013.00170 Aims/Hypothesis: Embryonic pancreatic bud cells, the earliest pancreas-committed cells, generated from human embryonic stem cells (hESCs) and induced pluripotent stem cells (hiPSCs) have been shown to differentiate into mature pancreatic β-cells in vivo, indicating the feasibility of hESC/iPSCbased cell therapy for diabetes. However, the key factors required for the differentiation of these cells into pancreatic bud cells are incompletely understood. The purpose of this study was to establish culture conditions that efficiently induce PDX1+NKX6.1+ pancreatic bud cells from hESCs/iPSCs. Methods: In vitro differentiation of hESCs/iPSCs Immunostaining Flow cytometry Quantitative real-time reverse transcriptionpolymerase chain reaction (qRT-PCR) Animal studies and transplantation experiments Statistical analysis In vitro differentiation of hESCs/iPSCs The maintenance culture of a hESC line, KhES-3 (Suemori et al., 2006), and five hiPSC lines; 585A1, 604B1, 692D2, 648B1 and 409B2 (Okita et al., 2011 and Kajiwara et al., 2012) was performed as described previously (Mae et al., 2013). For feeder-free cultures, cells were maintained with Essential 8 medium (Thermo Fisher Scientific, Waltham, MA) according to the manufacturer's instructions. Experiments with hESCs/iPSCs were approved by the ethics committee of the Department of Medicine and Graduate School of Medicine, Kyoto University. Cells were directed into key stages of pancreatic development, including definitive endoderm (Stage 1), primitive gut tube (Stage 2), posterior foregut (Stage 3) and pancreatic bud (Stage 4). The final protocol was as follows (Fig. 1A): Stage 1 hESC/iPSC colonies grown on a feeder layer were first deprived of feeder cells and dissociated into single cells as described previously (Suemori et al., 2006). The cells were resuspended with Stage 1 medium containing RPMI 1640 medium (NACALAI TESQUE, Kyoto, Japan) supplemented with 2% (vol/vol) growth factor reduced B27 (GFR-B27, Thermo Fisher Scientific), 50 U/ml penicillin/streptomycin (P/S, Thermo Fisher Scientific), 100 ng/ml activin A (R&D Systems, Minneapolis, MN), 3 μM CHIR99021 (Axon Medchem, Groningen, Netherlands) and 10 μM Y-27632 (Wako, Osaka, Japan), seeded on Matrigel (Becton Dickinson, Franklin Lakes, NJ)-coated plates at a density of 1 × 105 cells/cm2 and cultured for one day. For the next three days, the cells were cultured in RPMI 1640 medium with 2% GFR-B27, 50 U/ml P/S, 100 ng/ml activin A and 1 μM CHIR99021. Stage 2 The cells were exposed to Improved MEM Zinc Option (iMEM) medium (Thermo Fisher Scientific) supplemented with 1% GFR-B27, 100 U/ml P/S (iMEM-B27) and 50 ng/ml keratinocyte growth factor (KGF; R&D Systems) for three days. Stage 3 The cultures were continued for three days in iMEM-B27 with 0.5 μM 3-Keto-N-aminoethyl-N′aminocaproyldihydrocinnamoyl cyclopamine (KAAD-CYC; Toronto Research Chemicals, Ontario, Canada), 0.5 nM 4-[(E)-2-(5,6,7,8-Tetrahydro-5,5,8,8-tetramethyl-2-naphthalenyl)-1-propenyl]benzoic acid (TTNPB, Santa Cruz Biotechnology, Dallas, TX) and 100 ng/ml NOGGIN (Pepro-tech, Rocky Hill, NJ). Stage 4 The cells were cultured for four to 20 days in iMEM-B27 with 100 ng/ml KGF, 100 ng/ml NOGGIN and 50 ng/ml epidermal growth factor (EGF, R&D Systems). For monolayer and aggregation cultures, the cells after Stage 3 treatments were dissociated into single cells by gentle pipetting after treatment with 0.25% trypsin–EDTA. The same inducing factors were used as described above, except for the addition of 10 μM Y-27632 to the Stage 4 treatments. For monolayer cultures, the cells were seeded on Matrigel-coated plates at a density of 6–48 × 104 cells/cm2. To evaluate various extracellular matrices, the cells were seeded on laminin-111 (10 μg/ml; BioLamina, Sundbyberg, Sweden), fibronectin (5 μg/ml, Merck, Whitehouse Station, NJ), Synthemax (Corning, Corning, NY) and collagen I plates (Becton Dickinson). For aggregation cultures, the cells were seeded on a low-binding plate at a density of 3–30 × 103 cells/well. Figure 1. PDX1+NKX6.1+ cells are localized at aggregated areas. (A) A schematic diagram of the procedures used for the differentiation of pancreatic bud cells from human ESCs. (B–D) A hESC line, KhES-3, was differentiated into definitive endoderm, primitive gut tube endoderm, posterior foregut and pancreatic bud, and was analyzed by immunostaining for representative markers. (D) A magnified image of (C). Note that only the aggregated areas of PDX1high cells co-expressed NKX6.1. SOX17, SRY (sex determining region Y)-box17; FOXA2, forkhead box protein A2; HNF, hepatocyte nuclear factor; PDX1, pancreatic and duodenal homeobox 1; GATA4, GATA binding protein 4; NKX6.1, NK6 transcription factor related, locus 1. Scale bars, 300 μm in B and 100 μm in C and D. Immunostaining The cells were fixed with 4% paraformaldehyde (PFA) for 20 min at 4 °C. Then, immunostaining was performed as described previously (Mae et al., 2013). The primary antibodies used are detailed in Supplementary Table 1. The cell aggregates or implanted grafts were fixed with 4% PFA for one to two days at 4 °C. After washing with PBS, the samples were equilibrated in a 10–30% sucrose solution at room temperature for 1 h, and then mounted and frozen. The frozen blocks were sectioned at 10–30 μm, and immunostaining was performed after removing the mounting medium. For quantification of the Ki-67+ and cleaved-Caspase3+ cell ratios, immunostained cells were analyzed using an image analyzer CellInsight NXT (Thermo Fisher Scientific, Waltham, MA) or manual counting. Flow cytometry The cells were dissociated into single cells with 0.25% trypsin–EDTA treatment, fixed, permeabilized and blocked with a BD Cytofix/Cytoperm Kit (Becton Dickinson). Then, cells were stained with the antibodies detailed in Supplementary Table 1. Quantitative real-time reverse transcription-polymerase chain reaction (qRT-PCR) Total RNA was isolated from the cells with an RNeasy kit (Qiagen, Venlo, Netherlands), and cDNA was prepared with a ReverTra Ace qPCR RT Master Mix (TOYOBO, Osaka, Japan) and oligo (dT)20 primer, according to the manufacturer's instructions. The qRTPCR analysis was carried out with SYBR Premix Ex Taq II (Takara, Otsu, Japan). The expression of each gene was normalized to the level of glyceraldehyde-3-phosphate dehydrogenase (GAPDH) expression. The primer sequences used are shown in Supplementary Table 2. Animal studies and transplantation experiments All animal experiments were performed in accordance with the Guidelines for Animal Experiments of Kyoto University. Male seven- to 14-week-old NOD.CB17-Prkdcscid/J mice (NOD–SCID, Charles River Laboratories Japan, Yokohama, Japan) were maintained on a 12-h light/dark cycle with ad libitum access to a standard irradiated diet. Mice were anesthetized with inhalable isoflurane and received implants of hESCderived cell aggregates after Stage 4. Stage 4 day 4 cell aggregates (30 × 103 cells/aggregate) were cultured in Stage 4 medium with or without an ALK5 inhibitor (Santa Cruz) for one to two additional days before implantation. Then, two hundred cell aggregates per mouse were implanted under a kidney subcapsule. At 30– 210 days after implantation, the mice were sacrificed and the serial sections of grafts were examined by immunostaining, as described above. The graft function was assessed by measuring human C-peptide levels in mouse plasma in response to glucose administration. The mice were fasted for > 5 h, and a 30% glucose solution was administered by intraperitoneal injection at a dose of 3.0 g/kg body weight. Blood samples were collected prior to and at 30 min after the glucose administration via a tail vein into heparinized capillaries. The plasma human C-peptide level was analyzed by an ELISA (Mercodia, Uppsala, Sweden), according to the manufacturer's instructions. All metabolic analyses were performed in conscious and restrained animals. Statistical analysis The statistical analyses were performed using paired t-tests (SigmaStat 3.5, Systat, San Jose, CA). The differences between groups were considered significant for values of p < 0.05. Figure 2. Cell aggregation cultures promote PDX1+NKX6.1+ cell induction from PDX1+ posterior foregut cells. (A) A schematic diagram of the procedures used to assess the effects of the cell density on the cultures with regard to the induction of pancreatic bud cells. Posterior foregut cells differentiated in adhesion cultures were treated with the soluble factors required for pancreatic bud induction (KGF, NOGGIN and EGF), either with only a medium change (S4F) or with re-seeding at different cell densities for monolayer cultures (6– 48x104 cells/cm2, S4F-2D) or to form cellular aggregates (3-30x103cells/aggregate) (S4F-AG). (B) Representative bright field images of the three culture formats. (C) Quantification of the PDX1+NKX6.1+ cell ratio. After the induction of pancreatic bud cells in the three culture conditions described above, cells were examined by flow cytometry. (D) The mRNA expression of pancreatic bud markers, PDX1, PTF1A and NKX6.1, was assessed by quantitative real-time polymerase chain reaction (qRTPCR) before and during pancreatic bud induction with cell aggregation (black circle, solid line) and in monolayer cultures (open circle, dotted line). The data are presented as the fold-change in gene expression relative to the peak value. (E) A hESC line (KhES-3) and five hiPSC lines (585A1, 604B1, 692D2, 648B1 and 409B2) were differentiated into posterior foregut cells in adhesion cultures. Then, the foregut cells were dissociated, reseeded either for monolayer cultures (12 × 104 cells/cm2, 2D) or to form cellular aggregates (3 × 103 cells/aggregate, AG) and were treated with KGF, NOGGIN and EGF to induce pancreatic bud cells. After the differentiation, the PDX1+NKX6.1+ cell ratio was measured by flow cytometry. The data are presented as the mean ± S.E.M. from three to seven independent experiments in C and from three independent experiments in D and E. Scale bar, 300 μm. Figure 3. PDX1+NKX6.1+ cells emerge from PDX1high cells in cellular aggregates. Cell populations were analyzed by flow cytometry after 0–20 days of aggregation culture at Stage 4. (A) Representative dot plots indicating that NKX6.1+ cells emerged from PDX1high cells. (B) Quantification of the induction rate of PDX1+NKX6.1+ (black circle, solid line) and the total PDX1+ cells (open circle, dotted line). The data are from three independent experiments presented as the mean ± S.E.M. Figure 4. PDX1+NKX6.1+ cells in cellular aggregates coexpress multiple pancreatic bud markers. The localization of PDX1+NKX6.1+ cells in aggregates was assessed. Cryosections of cellular aggregates at Stage 4, days 4 (A) and 12 (B), were stained for the indicated markers of pancreatic buds (PDX1, NKX6.1, SOX9 and GATA4) and endocrine cells (INS, GCG, SST and GHR). Pancreatic bud cells were distributed throughout the entire aggregates, and were segregated from endocrine compartments. SOX9, SRY (sex determining region Y)box9; INS, insulin; GCG, glucagon; SST, somatostatin; GHR, ghrelin. Scale bar, 100 μm. Figure 5. Both cell aggregation cultures and soluble factor treatment are required for the efficient induction of PDX1+NKX6.1+ cells. (A) NKX6.1 expression was assessed by qRT-PCR in the cells treated with various combinations of soluble factors (100 ng/ml KGF, 100 ng/ml NOGGIN and 50 ng/ml EGF) for four days of Stage 4 aggregation culture. Cell aggregation alone did not induce the expression of NKX6.1. Treatment with all soluble factors with aggregation cultures most potently induced the expression of NKX6.1. (B) NOGGIN or all of the soluble factors (KGF, NOGGIN and EGF) was/were removed at the indicated periods during 12 days of aggregation culture at Stage 4. (Upper) A schematic diagram of the procedures used to assess the specific timing requirements for the soluble factors. (Lower) The quantification of the induction rate of PDX1+NKX6.1+ (black bars) and PDX1+NKX6.1− (white bars) cells. The data are from three independent experiments presented as the mean ± S.E.M. n/a, not applicable. Figure 6. The PDX1+NKX6.1+ cells generated with aggregation cultures differentiate into branched pancreatic epithelia in vivo. Cellular aggregates a Stage 4, days 4–5, were implanted into the kidney subcapsules of NOD–SCID mice. (A) An image of a host kidney harvested 30 days after implantation. The arrow indicates the location of the graft. (B–D) Cryosections of grafts were stained for the indicated markers Representative images of human pancreatic cells are shown. Asterisks indicate the host mouse kidney in B and C. HuN, human nuclei. Scale bars 100 μm in B and D and 300 μm in C. Figure 7. PDX1+NKX6.1+ cells generated with aggregation cultures mature into functional β-cells in vivo. A total of six million cells at Stage 4, day 5, of aggregation cultures that had been pretreated with an ALK5 inhibitor were implanted under the kidney subcapsule of NOD–SCID mice. (A) The average plasma human C-peptide levels in host mice were measured 30 min after glucose injection (3.0 g/ kg body weight, i.p.) at various time points after implantation, as indicated. (B) The average plasma human C-peptide levels after > 5 h of fasting (before) and 30 min after glucose injection (after) in the host mice were examined on day 150 after implantation. (C) A representative image of hESC-derived islet-like endocrine clusters on day 210 after implantation. The data are presented as the mean ± S.E.M. of 13 mice from four independent cohorts of implantation experiments in A and four mice from two independent cohorts of implantation experiments in B. *P < 0.05. Scale bar, 100 μm. Results: We differentiated a hESC line, KhES-3, into pancreatic lineages with a stepwise protocol recapitulating developmental process. The induction rate of PDX1+NKX6.1+ cells was correlated with cell density in adherent cultures, and markedly improved with cell aggregation cultures. The positive effects of cell aggregation cultures on the differentiation of pancreatic bud cells were reproduced in multiple hESC/iPSC lines. The human PDX1+NKX6.1+ cells developed into pancreatic epithelia after implantation into immunocompromised mice. Moreover, human C-peptide secretion into mouse bloodstream was stimulated by glucose challenges after in vivo maturation. Conclusions: Taken together, these results suggest that cultures with high cell density are crucial for the differentiation of pancreas-committed progenitor cells from hESCs/iPSCs. Our findings may be applicable for the development of hESC/iPSCbased cell therapy for diabetes. Message 糖尿病治療に向けてヒトES/iPS細胞から移植用の膵細胞を効率よく作製する方法を開 発 豊田太郎助教(京都大学CiRA増殖分化機構研究部門)、長船健二教授(京都大学 CiRA増殖分化機構研究部門)らの研究グループ ヒト多能性幹細胞(ES細胞およびiPS細胞)を膵臓の元となる膵芽(すいが)細胞へ と高効率に作製する培養条件を確立し、さらに作製した細胞が移植後に血糖値に応じ たインスリン分泌をする細胞へと成熟可能であることを示しました。この研究成果は 2015年1月28日(英国時間)に「Stem Cell Research」にオンライン公開されました。 膵臓は、膵前駆細胞と呼ばれる一層の細胞シートから膵芽と呼ばれる細胞の塊をつ くることで初めて形として認識することができます。つまり、膵芽は膵臓の最初の組 織であると考えられます。このため、膵芽細胞は糖尿病に対する細胞移植療法をはじ めとした膵臓再生医療の基盤となる細胞源として期待されています。これまでにヒト 多能性幹細胞から膵芽細胞を作製する方法はいくつか報告されていますが、分化の仕 組みが完全には分かっておらず、安定性、効率などの点について改良の余地がありま した。 本研究では、ヒトの膵発生過程において膵芽細胞が出現する際に細胞の塊をつくる ことに着目し、それを培養皿上で再現しました。その結果、細胞密度と相関して膵芽 細胞(PDX1+ NKX6.1+ cell)への分化が促進し、細胞塊を作製して培養することでさ らに効率よく分化することを発見しました。また、細胞塊の形成で分化誘導に効果が 見られたことから、細胞間相互作用を介した新たな分化の仕組みが存在することも示 唆されました。さらに、作製した膵芽細胞をマウスに移植すると、生着して胎児の膵 臓に似た組織構造を形成し、最終的には血糖値に応じてインスリンを分泌する成熟し た膵β細胞へと分化しました。 網膜神経線維層欠損 視神経乳頭部から扇状に広がる、周りの網膜の色と比 べて少しくすんで見える部分が網膜神経線維層欠損部 です。網膜神経線維層欠損は最も早期に生じる緑内障 性眼底変化といわれ、その部位に一致する視野障害を 認めることが多い所見です。 網膜神経線維層欠損(白黒写真) 網膜神経線維層欠損を無赤色フィルター光にて撮影す ると、その部分が周りの網膜に比べ暗く写り、通常の検 査よりはっきりと観察することが可能となります。 緑内障を疑う重要な所見です。文字通り神経が減っている所見です。神経が減っている ところは眼から脳への情報が伝えられませんので、視野が欠損します。 http://www.ningyocho-ganka.com/?page_id=42 1 Department of Ophthalmology, St. Vincent’s Hospital College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea. 2 Division of Endocrinology and Metabolism, Cheonan Chungmu Hospital, Cheonan, Republic of Korea. 3 Division of Endocrinology and Metabolism, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea. 4 Department of Ophthalmology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea. DOI: http://dx.doi.org/10.1016/j.ophtha.2015.01.001 Objectives To identify the factors associated with retinal nerve fiber layer (RNFL) loss in patients with type 2 diabetes. Design Cross-sectional study. Participants Ninety-six nonglaucomatous patients with type 2 diabetes without renal impairment (estimated glomerular filtration rate, ≥60 ml/minute per 1.73 m2). Methods Eyes were divided into 2 groups based on the presence or absence of RNFL defects detected by red-free retinal fundus photography. All participants underwent an eye fundus examination, and the urinary albumin-to-creatinine ratio (ACR) was determined. A cardiovascular autonomic function test was performed using the following heart rate variability parameters: expiration-to-inspiration ratio, response to the Valsalva maneuver, and standing. Multiple logistic regression analyses were performed to determine potential risk factors related to the presence of RNFL defects in these patients. Main Outcomes and Measures Main Outcomes and Measures The association between RNFL defects and diabetic complications. Figure 1. Red-free fundus photograph showing a representative case of retinal nerve fiber layer (RNFL) defect in a 43year-old man with type 2 diabetes. A narrow RNFL defect is shown at the 1-o’clock position in the red-free photograph (white arrows). A cotton-wool spot is seen on the inferior-temporal side of the retina. In this study, we excluded eyes with a glaucomatous optic disc because an RNFL defect is also a characteristic feature of glaucoma. Consistent with previous studies, we found that RNFL defects occurred predominantly in the optic disc on the superior side. The locations of the RNFL defects in patients with diabetes seemed to be clearly different from those resulting from glaucomatous RNFL damage, which occurs predominantly in the inferior temporal retina. Results Among the patients, 43 (44.8%) had localized RNFL defects (group 1), whereas the others (55.2%) did not (group 2). The RNFL defects occurred more frequently on the superior side (75.6% and 71.0% in right and left eyes, respectively) compared with the inferior side (13.8% and 0.0% in right and left eyes, respectively). Patients with RNFL defects (group 1) had significantly higher rates of diabetic retinopathy (60.5%) compared with those without RNFL defects (group 2; 32.1%; P = 0.007). The urinary ACR was significantly higher in patients with RNFL defects than in those without defects (45.3±72.1 μg/mg vs. 15.4±17.3 μg/mg creatinine, respectively; P = 0.015), whereas autonomic function test grading was similar between the groups. The urinary ACR was the only factor related to visual field defect location in both univariate (P = 0.021) and multivariate (P = 0.036) logistic regression analyses after adjusting for age; gender; presence of diabetic retinopathy; diabetes duration; smoking; statin use; and antiplatelet, angiotensin-converting enzyme inhibitor or angiotensin receptor blocker treatment. Conclusions Urinary albumin excretion was associated with nerve fiber layer loss in patients with type 2 diabetes. Careful examination of the optic nerve head may be necessary, particularly in patients with type 2 diabetes exhibiting albuminuria. Message 腎障害のない非緑内障の2型糖尿病(DM)患者96 人を対象に、網膜神経線維層(RNFL)欠損の関 連因子を横断研究で特定。RNFL欠損発生率は 44.8%だった。糖尿病性網膜症および尿中アル ブミン/クレアチニン比(ACR)はRNFL欠損なし 群に比べ、欠損あり群で有意に増加した。尿中 アルブミン排泄量がRNFL欠損と関連すると示唆 された。 もともと糖尿病で網膜神経線維層(RNFL)欠損 が言われていた。眼圧正常者を集めているが、 少なくとも眼圧は表示すべきだろう。 http://www.m3.com/clinical/journal/15179