Relationship between total
cholesterol and 90-day mortality
after acute myocardial infarction
in patients not on statins
Rishi Parmar
2nd year Medicine Resident
Introduction
• In most patients, there is a positive correlation
between total cholesterol (TC) and long-term risk
of myocardial infarctions (MI).
• However, in chronic heart failure patients, there is
an inverse relationship between TC and mortality.
• In acute MI, most researchers have found no
relationship between TC and mortality.
• We used the Optimal Trial in Myocardial Infarction
with Angiotensin II Antagonist Losartan
(OPTIMAAL) to evaluate the relationship between
TC and survival at 90-days and the end of the
study (median 2.7 years).
Study Population
• Of the 5,447 patients in the OPTIMAAL study, 5,206
patients were selected for our analysis based on
our inclusion criterion that recorded values for the
following variables:
– Age, gender, Killip Class, ejection fraction, smoking
history, past medical history of ischemic heart disease,
Myocardial Infarction, Heart Failure, stroke, peripheral
vascular disease, Chronic Obstructive Pulmonary
Disease, diabetes, atrial fibrillation, Coronary Artery
Bypass Grafting, angioplasty, TC, serum creatinine, and
aspartate aminotransferase.
• Recorded values for the variables in the study were
obtained at randomization, which was within 10
days of the acute MI.
Data Analysis
• Using the SPSS version 18.0, the study
population was analyzed using the
multivariate Cox models analysis
• Data was assessed for a linear or Ushaped relationship [(TC-nadir risk TC)2]
with all cause mortality
Population Characteristics
•
•
•
•
The mean age was 67 years
71% of the patients being men
17% diabetics
30% statin users
Lower TC was associated with older age, male
gender, Killip Class IV, lower AST, EF <35%,
lower BP, history of ischemic heart disease,
prior MI, diabetes, atrial fibrillation, prior cardiac
bypass, and use of beta-blocker.
Hazard ratios (in mmol/L) between lipids and
mortality at 90 days and end of study
Non-statin users
90 days
U shaped TC
(mmol/L)2
TC
(mmol/L)
HDL (mmol/L)
LDL
(mmol/L)
Unadjusted
HR
(95% CI)
*Adjusted
HR
(95% CI)
Univariate
p value
1.094
(1.058 -1.132)
1.068
(1.031 - 1.107)
0.910
(0.809 - 1.024)
0.694
(0.449 - 1.072)
0.937
(0.831 - 1.055)
0.611
(0.390 - 0.956)
0.990
(0.881 - 1.112)
Statin users
Multivariate
p value
Unadjusted
HR
(95% CI)
*Adjusted
HR
(95% CI)
Univariate
p value
Multivariate
p value
<0.001
0.001
1.024
(0.964 - 1.088)
1.019
(0.954 - 1.088)
NS
NS
NS
NS
NS
0.03
1.009
(0.809 - 1.258)
0.687
(0.297 - 1.588)
NS
NS
0.944
(0.764 - 1.167)
0.995
(0.456 - 2.174)
NS
NS
0.991
(0.879 - 1.118)
NS
NS
1.039
(0.852 - 1.267)
1.095
(0.883 - 1.357)
NS
NS
1.078
(1.051 - 1.105)
1.048
(1.020 - 1.076)
<0.001
0.001
0.978
(0.914 - 1.048)
0.975
(0.904 - 1.040)
NS
NS
0.915
(0.854 - 0.980)
0.951
(0.886 - 1.020)
0.011
NS
0.880
(0.765 - 1.012)
0.948
(0.819 - 1.098)
NS
NS
0.655
(0.509 - 0.844)
0.680
(0.522 - 0.885)
0.001
0.004
0.871
(0.523 - 1.451)
0.709
(0.415 - 1.213)
NS
NS
0.999
(0.934 - 1.069)
1.014
(0.946 - 1.088)
NS
NS
1.004
(0.884 - 1.141)
1.046
(0.910 - 1.201)
NS
NS
End of study
U shaped TC
(mmol/L)2
TC
(mmol/L)
HDL
(mmol/L)
LDL
(mmol/L)
* Model adjusted for age, gender, and smoking, Killip class, log of serum AST,
serum creatinine, systolic and diastolic blood pressure, heart rate, ischemic heart
disease, MI, heart failure, stroke, peripheral vascular disease, chronic obstructive
pulmonary disease, diabetes, atrial fibrillation, coronary artery bypass graft,
angioplasty and use of aspirin, b-blocker, and thrombolytics at randomization.
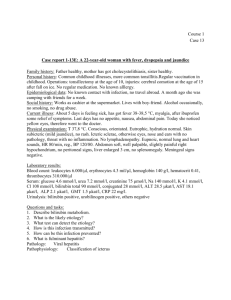
Unadjusted relationship between
TC and Mortality
The Hazard ratio of the U-shaped relationship
between mortality and TC level at 90 days and
end of study
Conclusions
• Our retrospective analysis of the OPTIMAAL database
suggests that in patients not taking a statin at the time
of acute MI there is a U-shaped relationship between
TC and mortality.
• The nadir risk was at 250mg/dL (6.4 mmol/L) (Figure
2), with the relationship present as early as 90 days
post MI.
• A 100 mg/dL increase or decrease from 250 mg/dL
was associated with ~60% increase in mortality.
• In statin users, there was no relationship between TC
and mortality.
• Statin use was associated with a 20% mortality
reduction (multivariate p value =0.022) with the benefit
appearing after 6 months.
Study Limitations
• The OPTIMAAL database doesn’t contain
the inflammatory markers such as CRP
that could help delineate the causes of the
U-shaped relationship between TC and
mortality.
Acknowledgements
• Team members:
– Wayne Levy, MD (Mentor)
– Alec Moorman, MD
– Kenneth Dickstein, MD (Norway)
– John Kjekshus, MD (Norway)
 0
0