The Impact on Caregivers of Young Adult Opioid

The Impact on Caregivers of
Young Adult Opioid Use
Sarah Bagley MD
Addiction Medicine Fellow
Clinical Addiction Research and Education Unit
Boston University School of Medicine
CREST Fellows Presentations
February 24, 2015
Supported by the Research in Addiction Medicine Scholars program
NIDA R25DA033211
Thanks to Alex Walley for background slides
Outline of Presentation
• CREST project
• Proposed K23 Specific Aims
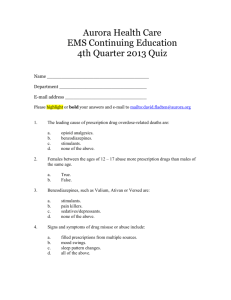
Drug Overdose Deaths in U.S. 1990-
2008
More Than Tripled
National Vital Statistics System. Drug overdose death rates by state. 2008.
Strategies to Address Overdose
Prescription monitoring programs 1
Prescription drug disposal 2
Safe opioid prescribing education 3
Opioid agonist treatment 4
1. Paulozzi LJ, et al. Pain Med. 2011 May;12(5):747-54.
2. Gray NE and Hagemeier JA. Arch Intern Med. 2012;172(15):1186-1187.
3. Albert S, et al. Pain Med. 2011 Jun;12 Suppl 2:S77-85.
4. Clausen T, et al. Addiction. 2009 Aug;104(8):1356-62.
Overdose Education and Naloxone
Distribution
• Initial efforts to implement OEN with people with use drugs
• >50,000 people trained to recognize and respond to an overdose between 1996-2010 1
• Overdose education and naloxone distribution
(OEN) effective response to reduce deaths 2, 3
• Study in 2010 indicated that caregivers may also be interested in receiving OEN 4
1. CDC. MMWR. 2012;61(6):101-105
2. Walley AY, Xuan Z, Hackman HH, et al. BMJ. 2013;346:f174.
3. Coffey PO and Sullivan SD. Annals Int Med. 2013;158(1):1-9
4. Strang et al. Drugs, Education and Policy. 2008;15(2):211-218.
Research Aims
Aim 1
Describe the characteristics of family members of opioid users who attend a support group for families affected by addiction who participate in OEN and those who do not.
Aim 2
Describe the motivations and benefits for family members of opioid users to receive OEN.
Aim 3
Describe the number of times trained family members have used naloxone to reverse an opioid overdose.
Methods
• Cross sectional study conducted between July
2013-September 2013
• Convenience Sample
• Setting: community support group for family members affected by addiction
Setting
• Learn to Cope: founded in 2004 by mother whose son had an opioid addiction
• Provides support and nonprofessional advice to family members
• In 2011, OEN offered at every meeting
• 10 meetings in Massachusetts in 2013
Methods
• Massachusetts Opioid Overdose Prevention
Pilot Program
– Started in 2006
– Provides OEN to community groups throughout
MA
– More than 28,000 people trained and > 3,300 rescues
Procedure
• Attendees at meeting given option to participate in an anonymous 15 minute survey
• $5 gift card for compensation
Instrument
• 42 items
• 5 domains: demographics, relationship to opioid user, experience with overdose, motivations to receive OEN, and naloxone rescue kit use
• Piloted with 5 Learn to Cope members prior to starting study
Aim One: Characteristics of Attendees
Age
(mean)
Female
White
Married
Parent
Total
N=125
OEN
Trained
N=99
Untrained
N=26
P-value
53.1
78%
95%
74%
85%
52.3
79%
94%
75%
91%
55.0
77%
100%
73%
65%
0.20
0.84
0.44
0.99
0.0056
Aim One: Characteristics of Attendees
P-value
Provide financial support
Daily contact
Applied for courtmandated treatment
Witnessed overdoes in past
Heard about naloxone before L2C
Total
(N=125)
52%
50%
35%
30%
47%
OEN Trained
(n= 99)
58%
54%
41%
35%
43%
Untrained
(n=26)
30%
33%
15%
12%
59%
0.0086
0.0041
0.04
0.07
0.14
Aim Two: Motivations for Receipt of
OEN
OEN Trained
(n=93)
72% Wanted to have in the
House
Encouraged by Education
Provided at L2C
Heard About Benefits from
L2C Members
Wanted More Information about OD
60%
57%
26%
Wanted Kit for Someone
Else
Previously Witnessed OD
19%
18%
Experienced Death of Loved
One
1.1%
Aim Two: Reported benefits of OEN
BENEFITS
Greater sense of security
Improved confidence to handle OD
Greater understanding of prevention and management of OD
Educate others about OEN
Ability to reverse an OD
OEN Trained
(n=92)
74%
62%
60%
33%
29%
Aim Two: Motivations for OEN among untrained
OEN Not Trained
(n=13)
69% Encouraged by education provided at L2C
Wanted to have in the house
Heard about benefits from
L2C members
Wanted more information about OD
Wanted kit for someone else
Previously witnessed OD
Experienced death of loved one
31%
31%
23%
7.7%
7.7%
0%
Aim Three: Use of Naloxone
N
5 Total Rescues
RELATIONSHIP
Parent
Grandparent
Stranger
Other
SETTING
Public
Private
CHARACTERISTICS
Survived
Called 911
Rescue Breathing
1
1
2
1
1
4
5
5
4
Conclusions
• High uptake of overdose education and naloxone rescue kits offered at the meetings.
• Trainees were parents who provided financial support, had daily contact, had applied for courtmandated treatment, and had witnessed an overdose.
• Among the minority who had not received OEN, almost half wanted to be trained.
• Several attendees had administered naloxone successfully
Limitations
• Cross-sectional
• Convenience sample
• Self-selected population
• Missing data
Implications
• Family members should be included in the response to the opioid related overdose epidemic
• More work needed to determine the most effective way to implement OEN programs in community settings
• How to expand OEN to families who are not coming to meetings?
Next Steps
• Observed consistent high burden of stress that family members experience
• Caregiver populations of patients with other chronic diseases find high levels of stress, poorer physical health outcomes should we be focusing on engaging families?
Next Steps
• Family members whose loved one use substances have higher morbidity and health care costs
• No data about specifically about impact of opioid use
• Treatment of addiction increasingly integrated into primary care settings
• Strategies exist to provide support for families but are not necessarily well implemented/disseminated in primary care
Research Question
What is the impact on caregivers of transitional age youth with opioid use disorders?
Aims
Aim One
Identify the physical and emotional impact on the primary caregivers of transitional age youth who use opioids.
Design and conduct a mixed methods study of caregivers of transitional age youth with opioid use disorders to identify the physical and emotional impact and to identify strategies to address the impact.
Aim Two
Design and conduct a statewide survey of medical directors at community health centers that provide integrated primary care and addiction care to understand if and how primary caregivers are engaged in treatment.
(Aim Three or R03)
Develop and implement a pilot intervention using data gathered from
Aims 1 and 2 for caregivers whose transitional age youth who use opioids to be delivered in primary care settings.
Acknowledgements
• Joanne Peterson and Learn to Cope
• Alex Walley MD, MSc
• Charlie Jose MPH
• Debbie Cheng ScD
• Emily Quinn MPH
• Patrick O’Connor MD, MPH
• Jeffrey Samet MD, MPH, MA
• Michael Silverstein MD