Health - Michael
advertisement

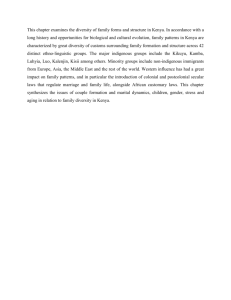
Policy Workshop Health Universitas Indonesia June, 2013 Michael Kremer Harvard University 1 Income per Capita (2005 dollars) Life Expectancy 80 6000 70 5000 60 50 4000 40 3000 30 2000 20 1000 10 0 0 United Vietnam States 1900 2009 SSA 2009 United States 1900 Vietnam 2009 SSA 2009 2 Two Themes • Preventative and non-acute care vs. acute care o Cost differences: provide to everyone vs. personalized specialized care o Behavioral differences? o Epidemiological transition • Consumer vs. supplier behavior Debate Over Cost Recovery Advocates: • The poor can pay at least some fees • Charging may increase valuation, screen out low valuation consumers • Fees vital to sustainability, motivating providers Critics: impact on access Compromise: small fees, variation by sector Decision framework? Since 1995, a wave of randomized evaluations: Any generalizable lessons? Grossman Model Health as Human Capital • Consumers invest if expected private benefit exceeds costs 5 Policy Implications • Potential government role when private and social benefits of health investment differ – Epidemiological externalities – Natural monopoly/public good – DWL of taxation: fiscal externality – Response of take-up to price affects optimal subsidy 6 Externalities: School-Based Deworming in Kenya • Disease externalities on neighboring schools, untreated in school – Disease prevalence – School attendance • Fiscal externality o Increased labor supply ten years later • Price response o 75% take-up when free, 18% with small user fee o No difference in take-up with family size despite per family fee structure o Sicker students not more likely to pay for drugs 7 Public Goods: Spring Protection • $1K capital cost, negligible marginal cost • Randomized trial suggests 25% reduction in diarrhea, switching to protected springs • Estimate that full private property would create large static losses, little dynamic benefit • This might be different at higher income levels 8 Health Human Capital Model • Testable implications? – Very flexible model? Tautological? – Investment responds to perceived benefits – Price response – Treatment/prevention equivalence – Information response – Alternative models? Policy implications? Impact of Price on Preventative Health Take-Up 10 Does Paying Makes People More Likely to Use Health Goods? • Widely believed by practitioners • Could arise due to sunk cost fallacy • No evidence – Bednets in Kenya & Uganda (Cohen & Dupas 2010; Hoffman et al 2009) – Water purification in Zambia (Ashraf et al 2010) • Importance of zero price point 11 Financial Incentives (Negative Prices) • Large negative prices in conditional cash transfer programs increase uptake of health and education – Health & education: Mexico (Gertler 2004; Schultz 2004) – Health: Tanzania (Evans et al. 2012) • Small incentives also have remarkable impact – HIV test results in Malawi (Thornton 2008) – Cash transfer in Malawi: Transfer amount does not affect outcomes (Baird et al 2011) – Implications for human capital model? 12 Information • Often, little impact of health education – Intensive school health education intervention had no impact on worm prevention behaviors in Kenya (Kremer & Miguel 2007) • But in some cases, dramatic impacts – Information on HIV prevalence by age in Kenya (Dupas 2011) • Some puzzles for learning model – Fade out of education campaign effect – Greater responsiveness to coarse information in Bangladesh (Bennear et al 2011) – People tested negative for malaria still buy malaria meds in Kenya (Dupas et al 2012) 13 Acute Treatment and Insurance • Substantial expenditure on health treatment of doubtful utility (Das and Hammer, 2005; Banerjee et al., 2004) • Consumers bear substantial health risk (Gertler & Gruber 2002) • Low take-up of voluntary health insurance in Nicaragua (Thornton et al 2010) • Limited and mixed evidence on effect of price of clinic visits on take-up, health – Exogenous increase in fees at clinics in Indonesia (Dow et al 2003) – Subsidized anti-malaria in Kenya (Cohen and Dupas 2011) – Mexican Seguro Popular health insurance program had no effect on healthcare utilization in short term (King et al 2009) 14 Behavioral Model: • Present bias – Small up-front costs can deter investments with immense long-run payoff • Limited attention, salience, habit and norm formation • Welfare economics? • Health planning approach? 15 Applying Insights from Behavioral Economics: Program Design and Testing • Water infrastructure often expensive, recontamination frequent • Chlorination safe, effective, low-cost, but single-digit take-up under social marketing • Design for free distribution, convenience, habit formation, norm formation 16 Chlorine Dispenser System • Majority of households test positive for chlorine, use sustained over time (Kremer et al 2011) • Very low cost 17 Health Care Provision: Background Chaudhury et al. (2006) 18 Poor Quality Physicians in Tanzanian hospitals… Physical exams per patient 1.5 Questions asked per patient 4 Minutes spent per patient 6.3 0 1 2 3 4 5 6 7 Das et al 2008 • Frequent use of unqualified providers in Tanzania and other countries (Leonard & Masatu 2007; Das & Hammer 2005) 19 Approaches to Addressing Government Failure in Service Delivery • Community mobilization for accountability • Provider Incentives • Paying for results • Contracting for health 20 Community Mobilization and Accountability • Community monitoring of health services in Uganda (Björkman & Svensson 2009) – Provider absence 14% lower in treatment facilities – Vaccination rates increased 46% – 46% more children received vitamin A supplements • Contrasting results in India education 21 Provider Incentives • Pay for performance program in Rwanda: Significant increase in quality prenatal care but no impact on number of visits (Basinga et al 2010) • Non-financial rewards motivate public health workers in Zambia (Ashraf et al 2012) • Monitoring program linked pay to nurse attendance in India (Banerjee et al 2008) – Initial attendance boost; disappears after 6 months (program undermined) 22 Paying Communities for Results? • Block grants to communities tied to results (Olken et al 2011) – Regular weight checks for children and iron tablets for pregnant women increased – Malnutrition fell by 2.2 percentage points 23 Contracting for Health in Cambodia • Management of healthcare contracted out to NGOs in some districts (Bhushan et al 2006) • Targeted health outcomes increased one standard deviation – 42% increase in vitamin A and 36% increase in prenatal care coverage – Decreased absence rates among providers • No change in non-targeted health outcomes • Increased government spending in contract districts offset by decrease in private health spending 24 Areas for Future Research • Optimization failure and normative analysis • Social norms in health, role of media (La Ferrara et al., 2008; Jensen and Oster, 2009) • Health care issues once low-hanging fruit is picked: aging, curative care, social insurance • Intersection of IO and health o Pharmaceutical markets (Goldberg, 2006; Yanagizawa-Drott, 2012; AMCs) o Private and public providers (Das et al. 2007) • Political economy of health (Miller, 2008; Fujiwara, 2010; Duflo and Chattopadhyay, 2004) 25 Policy Conclusions • RCTs and policy o CCTs o Deworming o Needs tremendous amount of additional work • Strong case for free, convenient provision of cost effective technologies for prevention of communicable disease • Improved provision of curative care is challenge for future o Promising approaches, but need more evidence 26 END 27 Child Mortality and Income 28