CHF Case Study
advertisement

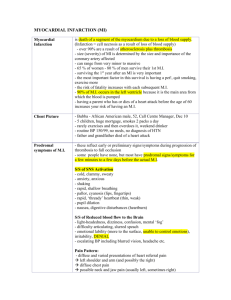
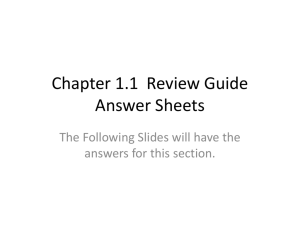
Congestive Heart Failure (CHF) in a 79-Year Old Male How does distance walked in 6 minutes relate to re-hospitalization? Clinical Problem Solving I Kaylea Kirven Purpose: • To describe the physical therapy – ▫ ▫ ▫ ▫ Examination Evaluation Plan of care Outcomes • To examine research related to my prognostic question – ▫ Is 6-minute walk test distance a prognostic indicator for re-hospitalization in elderly male patients with severe congestive heart failure? “Mr. C” • 79 year old male • Admitted to hospital presenting with: ▫ ▫ ▫ ▫ ▫ Abdominal pain Shortness of breath Dizziness Dysphagia Weight gain of 23 lbs • Past Surgical History: ▫ CABG x 4 (1981) ▫ Tonsillectomy “Mr. C” • Comorbidities: ▫ ▫ ▫ ▫ ▫ ▫ ▫ ▫ Coronary Artery Disease (CAD) Hypertension (HTN) Diabetes Degenerative Joint Disease Chronic Kidney Disease Chronic Atrial Fibrillation Previous Stroke (CVA) Dementia • Diagnosis: ▫ Ingested foreign object ▫ Congestive Heart Failure (CHF) Diastolic: NYHA Class I Systolic: NYHA Class IV (Ejection Fraction: 25%) NYHA Classifications: NYHA Grading Functional Capacity Class I: Asymptomatic Dysfunction Class II: Mild CHF Class III: Moderate CHF Class IV: Severe CHF No limitations Ordinary physical activity does not cause fatigue, dyspnea, or palpitations Slight limitations Ordinary physical activity results in fatigue, dyspnea, & palpitations Marked limitations Less than normal physical activity results in symptoms Unable to carry out any physical activity w/o discomfort Symptoms present @ rest Physical Therapy Evaluation: • Prior Level of Function: ▫ Ambulation: RW ▫ 24 hr. care EVAL CRITERIA AROM • Elderly Mobility Scale: ▫ 10/20 “Patient is borderline in terms of safe mobility & independence in ADLs & requires help with some mobility maneuvers.” WFL Shoulder flexion Hip abduction • Review of Systems: ▫ Bilateral lower leg edema (2+) ▫ Breathing discomfort while supine w/ head of bed down FINDINGS PROM MMT Generalized Weakness Decreased tolerance for activity PT Initial Evaluation: Continued Bed Mobility: Rolling L/R Modified Independence (HOB raised + Rail utilization) Balance: Sitting Static Balance Good Sitting Dynamic Balance Not Tested * Standing Static Balance Fair– with Rolling Walker Standing Balance with Gait Fair – with Rolling Walker + CGA HOB: Head of Bed CGA: Contact Guard Assistance * Should have been performed Impairments: • Edema (2+) • Pain (2/10) • Decreased ROM Right > Left • Decreased Strength • Decreased Endurance Disabilities: • Decreased independence with ADLs Functional Limitations: • Decreased independence with transfers & ambulation Treatment:Ambulation Distance Day 1 Day 2 Day 3 3/10 2/10 1/10 Therapeutic - Charleston 600 Exercises in Sitting - Toe Taps (1 set of 10 reps) - Heel Taps 500 - Seated Marches - Long Arc Quads SAME SAME 400 Transfers Minimal Assistance Sit <-> Stand x2 With300 Rolling Walker Minimal Assistance Contact Guard x2 Assistance x 1 700 Distance (ft.) Pain (NRPS) 200 Ambulation 100 0 RW: Rolling Walker +time & verbal cues + verbal cues + verbal cues 125 ft. (~38 meters) 300 ft. (~91 meters) 657 ft. (~200 meters) + RW, CGA, Verbal Cues + RW, CGA, Verbal Cues Balance Losses: 2 Balance Losses: 2 Reached 6 min. of continuous walking + RW, CGA + 4 Breaks DayLOBs: 1 Loss of Balances Day 2 Day 3 Patient-Centered Goals: Within 7 days, the patient will… ▫ Supine to sit with modified independence ▫ Transfer from bed to chair with minimal assistance + contact guard assistance while holding onto rolling walker ▫ Sit to stand with minimal assistance + contact guard assistance ▫ Ambulate with contact guard assistance + rolling walker 750 ft. (~228 meters) PT to see patient 4 x/week • Treatment Outcomes: ▫ Improving & progressing towards goals • Prognosis: ▫ Good – Expected to return to previous level of function Factors Influencing Rehabilitation Potential: 1. Medical Condition (-) 2. Safety Awareness (-) 3. Age (-) 4. Comorbidities (-) 5. Mental Status (-) 6. 24 hr. care @ home (+) 7. Supportive Wife (+) Discharge Site: Home Health Since lives in a 24 hr. care facility Clinical Question: Is 6-minute walk test distance a prognostic indicator for re-hospitalization in elderly male patients with severe congestive heart failure? • Important to consider disease severity & hemodynamic status in CHF patients • Help identify which CHF patients will likely require intensive therapy? Promote more effective use of therapies Help optimize treatment in the CHF population CHF Statistics: • Heart failure is the leading cause of hospitalization among adults > 65 years old ▫ Annually: > 1 million patients are hospitalized for heart failure [Medicare Expenditure = $17 billion] ▫ Within 6 Months of Discharge: > 50% of patients are readmitted to hospital Article 1: Prediction of Mortality and Morbidity With a 6-Minute Walk Test in Patients With Left Ventricular Dysfunction Journal of the American Medical Association, 1993 Bittner et al. Bittner et al. • Purpose: ▫ To study the potential usefulness of the 6-MWT as a prognostic indicator in patients with left ventricular dysfunction • Methods: Prospective Cohort Study ▫ 898 patients enrolled in the Studies of Left Ventricular Dysfunction (SOLVD) Registry Ejection Fraction < 0.45 (45%) &/or radiological evidence of CHF Ischemic Cause or Hypertensive Cause ▫ 6-MWT performed at baseline ▫ Follow-up Period: 242 days Information provided by 895/898 patients Bittner et al. Walkers: N = 833/898 Substudy Patients Age 60 + 12 Sex (%) 78% males / 22% females Ejection Fraction (%) 37 + 14 NYHA I (%) 35% NYHA II (%) 47% NYHA III (%) 14% NYHA IV (%) 1% * Note: Most participants were in LOWER NYHA classifications Bittner et al. • Levels: ▫ Level 1: < 30o meters ▫ Level 2: 30o – 374.9 meters ▫ Level 3: 375 – 449.9 meters ▫ Level 4: > 450 meters 80%: Level 1 & Level 2 While distance was consistent with functional status at the extremes of the NYHA classification system, this graph demonstrates a substantial range in the broad class of mild impairment (NYHA Class II) Bittner et al. Note: Hospitalization for any reason & hospitalization for CHF INCREASED significantly as distance walked decreased Performance Level 1: MORE total hospitalizations MORE hospitalizations for CHF Article 2: Prognostic Usefulness of the SixMinute Walk in Patients With Advanced Congestive Heart Failure Secondary to Ischemic or Nonischemic Cardiomyopathy American Journal of Cardiology, 2001 Shah et al. Shah et al. • Purpose: ▫ To analyze the ability of the 6-minute walk test to predict death & hospitalization in patients with NYHA Class III or IV CHF • Methods: ▫ 471 patients (initially) 440 patients NYHA Class III or IV Ejection Fraction <25% ▫ 6-MWT protocol was followed Performed at baseline ▫ Follow-up Period: @ 52 weeks Shah et al. • Results: How Evaluated? ▫ Cox Proportional-Hazards Model Provides an estimate of the hazard ratio & its confidence interval Hazard Ratios: The chance of events of a hazard occurring at a group relative to the other Provide confidence in the reliability of the trial data Shah et al. 6-Minute Walk Test Baseline Distance: Baseline 6-MWT Distance N = 365 Median: 218 meters Unable to participate in 6-MWT Default Score: 0 meters (Too ill to walk) N = 75 NYHA HR SBP DBP Shah et al. Cox Proportional-Hazards Model: Distance covered on the baseline test significantly predicted re-hospitalization 0.85/100 m increase HR 95% CI Chi Square p-value Heart failure patients who increase their walking distance by 100 meters are 0.15 times less likely to be re-admitted to the hospital (or have a 15% lower risk of re-hospitalization) Relative Risk Reduction: 1 – (HR)- Δ distance +100 meters 17.6% +150 meters 27.6% +200 meters 38.4% Shah et al. 365 Baseline Walkers: • 217/365 hospitalized (60%) • 252/365 combined endpoint (69%) Limitations: Bittner et al. • Small sample size among NYHA Class III/IV Shah et al. & Bittner et al. • 6-MWT’s performed by a variety of staff members ▫ Reproducibility NOT formally assessed • Patients only assessed once (at baseline) • Small percentage of women ▫ May affect generalizability to both genders • Sub-max Test ▫ Patients DO NOT achieve a peak O2 consumption ▫ Hard to compare to maximal exercise testing • Assistive devices utilized? • What were the participants doing between baseline testing & follow-up? Conclusions: Bittner et al. Shah et al. • 6-MWT distance strongly & • Baseline distance walked significantly predicts independently predicts hospitalization in patients hospitalization rates among with advanced CHF NYHA Class I & II CHF patients • Higher hospitalization rate during follow-up • Hospitalization during ▫ Participants had Severe follow-up was lower CHF ▫ Fewer severe heart EF of 0.25 or less failure patients EF of 0.45 or less Baseline distance walked is inversely related to NYHA Class How Does This Research Relate to My Patient? • Article 2 (Shah et al.) relates better to my patient ▫ Mr. C met all inclusion criteria NYHA Class III/IV Ejection Fraction < 25% • Mr. C walked 200 meters (657 ft.) in 6 minutes ▫ First Study: Performance Level 1 (< 300 meters) ▫ Second Study: Shy of Median Distance Walked (218 meters) = His distance walked IS a prognostic indicator for his risk of re-hospitalization (Actually re-admitted 3 months after I saw him) In the Future: 1. Do changes in test performance over a 1-month period add further prognostic information? If so, what change from baseline is clinically significant for a better prognosis? 2. Utilize the 6-MWT to develop/monitor rehabilitation & progression 3. If a patient is too ill to walk, what else can be used to determine exercise capacity? Conclusion: • Simple, non-invasive method to: ▫ Risk-stratify patients with CHF • Objective measure to: ▫ Guide clinical judgment & management of CHF patients • Safer alternative to cardiopulmonary exercise testing ▫ Most CHF patients are unable to perform a maximal symptom-limited exercise test ▫ Correlates better with daily activity effort References: • Bittner V, Weiner DH, Yusuf S, Rogers WJ, McIntyre KM, Bangdiwala SI, et al. Prediction of mortality and morbidity with a 6-minute walk test in patients with left ventricular dysfunction. SOLVD Investigators. Jama. 1993;270(14):1702-7. • Pollentier B, Irons SL, Benedetto CM, Dibenedetto AM, Loton D, Seyler RD, et al. Examination of the six minute walk test to determine functional capacity in people with chronic heart failure: a systematic review. Cardiopulmonary physical therapy journal. 2010;21(1):13-21. • Shah MR, Hasselblad V, Gheorghiade M, Adams KF, Jr., Swedberg K, Califf RM, et al. Prognostic usefulness of the six-minute walk in patients with advanced congestive heart failure secondary to ischemic or nonischemic cardiomyopathy. The American journal of cardiology. 2001;88(9):987-93. Questions?