Dec 14 Meeting notes - Seascale Health Centre
advertisement

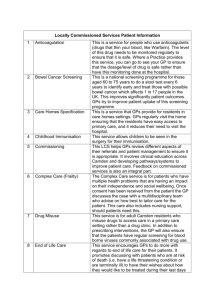
Seascale and Bootle Patient Participation Group Wednesday 3rd Dec 2014 3.00pm Meeting notes Attendees: Viv Stucke Betty Jacob Alan Jacob Neil Robson Ken Mawson Jane Fisher Colin Fisher Mary James Judith Gale Practice Staff: Lisa Drake Clare Temple Apologies: Dr Kathryn Illsley Liz Clegg Mike Harrington Alexandra Brassington Annette Barker Joan Marlow Marion Thornton Last meeting held – Jan 14. Presentation provided to U3A in April 2014. Due to staff and GP pressures in the practice, correspondence with group has taken place ‘virtually’ in throughout Summer and Autumn 2014. Notes are available on practice website under patient group pages. Agenda 1. West Cumberland Hospitals - move of services North Cumbria University Hospitals Trust (NCUH) meeting arranged for 24th November in Methodist Hall, at very short notice. Practice only heard about it on Fri 21st from EC which was too late to rearrange Drs lists to allow anyone to attend. HealthWatch Cumbria were facilitating, but said they were not allowed to give out dates until press release. Thank you to all who attended, with 40 people at meeting which was much better than any other meetings held to date, but further dates planned in Whitehaven. Purpose was for NCUH to present options for changes to service provision in following main areas; Paediatrics, maternity, A&E, elective operations. Further details are here: http://healthwatchcumbria.co.uk/seascale-engagement-event-a-great-success/ NCUH propose 3 viable options and are trying to get public opinion. The overwhelming response was 'everything we have now' and nothing less which seemed a surprise to NCUH. HealthWatch will write report to advise NCUH what the public want. These meetings are not deemed a formal consultation. NCUH will present to CCG the option that they prefer. The Patient group commented that there was no discussion on what has already been removed and we had been led to believe that the previous services changes were on a temporary basis. No attendance from the CCG at the meeting. HealthWatch said that if there was enough demand they will put on other meetings. NCUH proposed more 'low risk surgery' at WCH, with a centre of excellence with new theatres. No definition of 'seriously ill' had been provided or numbers of patients affected, but these cases would 1 Seascale and Bootle Patient Participation Group be sent to Cumberland Infirmary (CIC). NCUH state that they have the best consultants at CIC. The group suggested that Carlisle patients are unlikely to choose to have elective surgery at WCH for the same reasons as West patients not wanting to travel to CIC. Group commented that the latest proposals did not reflect 'Closer to Home' where it was agreed that CIC consultants would travel to WCH to treat seriously Ill patients and not move patients to CIC. University Hospitals Morecambe Bay trust (UHMBT) have recently bid for additional £17m to offset their overspend of £19m, stating that their deficit is 'due to running multiple hospitals which were far apart and have low volumes of patients due to rurality'. UHMBT seem to have a better local support and Barrow and South lakes appear more proactive with DH /Commissioners than NCUH, perhaps NCUH need to try to replicate? Recruitment continues to be a problem in West Cumbria for and it is affecting all areas of Health Care. NCUH use this as the reason for moving services as recent reviews have said WCH is not adequately staffed, therefore it is not safe. Whilst the group acknowledge the need for more serious cases to receive specialist care, if we lose these services from WCH totally, what happens to the next 'tier' of less serious cases? The groups main concern is that there wont be anyone left to treat a greater number of 'less serious' patients and moving them to CIC may have a detrimental affect. Local Drs may also need to adjust their decision making if patients have to travel to CIC and there is limited community support to allow patients to remain in their own homes. Patients are less likely to accept that admission is necessary if they know they will travel to CIC when unwell, or their families cannot visit. Just because of rurality, we do not need to accept second rate services. JG commented that Facebook has a campaign for 'Save West Cumberland Hospital'. The 'Millom Mums Baby pram push' had also taken place to raise awareness over our travel distances. Although these campaigns have been proactive, it was recognised that this will not reach those who don't use social media. These campaigns are often not widely covered in local media. The group commented on the proximity of Sellafield, the number of people based there and this is now the biggest building site in the country. How would they cope if a large accident happens (eg the scaffold collapse 1994)? New developments anticipate 5-8000 more people. The Roads and infrastructure would block and over the last month there have been 3 events where A595 is closed completely for up to 2 hrs. This again has led to major disruption in the Surgery as staff were unable to get into work or down to Bootle. In 2012 the snow closed the A595 between Muncaster and Bootle and GPs couldn't get to Bootle for 5 days because the train lines were also closed. There doesn't seem to be communication between the Local employers and the trusts etc. Although there is an Emergency planning group that prepare in event of worst case 2 Seascale and Bootle Patient Participation Group scenarios, the group are more worried about every day less serious events that still have big impact on primary and community care. Latest NICE report suggests that 'Low risk' pregnancies are better off at midwife led units, but only if the unit is closely linked to Consultant Led Obstetrics and Paediatrics - these units are not best if they are over 1- 2 hrs drive away. NCUH have said there were not enough live birth rates to sustain a maternity unit. VS questioned this and stated that the evidence is limited. This current process feels that we are being told what will be available, not what will be best for our community or not what GP Commissioners want. AJ commented that 'GPs are supposed to be in charge' and asked what the Drs here were doing about these proposed changes? LD provided a pictorial representation of how local GPs are involved in the decision making in Copeland and Cumbria to explain the complexity of the Health and Social Care Act changes. ACTION, LD to send paper copy to all of the group Cumbria - NHS Landscape - the old and the new Nov-12.pdf Local GPs had written a letter to Commissioners and NCUH about their increasing concerns and this had been published in the Whitehaven News. hospital letter 2014 Local residents had wondered why there were no signatures from Seascale GPs? LD explained that the GPs from Seascale had raised their concerns directly with CCG and Dr Juliet Rhodes (Fellview HealthCare) as the new Lead GP responsible for Copeland. Dr Rhodes is planning a visit to the practice soon. Dr Illsley attends the Locality Executive meeting on behalf of the practice along with other Copeland GPs and this is the place for issues such as these to be discussed. AJ asked how the community get feedback from what the GPs have put forward. The commissioners (CCG) are closely involved with the issues but don't appear to have the solutions. It feels as if the acute trusts as providers are leading the discussions with population but CCG will have to manage any public Consultation and that is where the concerns will be heard and feedback will be delivered. Also, a patient had asked if they could leave a 'Save West Cumberland Hospital' petition in the surgery, calling for patients to sign to stop the changes. Seascale GPs were concerned as the introduction to the petition contained 'alarming statements'. Whilst we understood this might be necessary to galvanise community support, the Drs felt it was a difficult 3 Seascale and Bootle Patient Participation Group balance to strike between reassuring patients and seeking support. We all support the need for continued high quality, safe services. LD stated that whilst the practice can raise issues through the local commissioning structure, she asked if it was possible for the group to work with Local Government to raise our concerns over the affects of these proposals on the rural community as a whole. Other items such as rural transport, loss of local banking, library services etc all have an effect on the population health. AJ asked LD to prepare a list of concerns/ questions for parish and local council so they could address members and seek councilor’s support and response, i.e. list the concerns and ask what has been done to address these. ACTION, LD VS has been checked the HealthWatch website to see if the presentations discussed at the meetings were available to circulate more widely. Can we have these available in the surgery? LD to check. Post meeting note; Presentations still not available on Healthwatch website. The 'Options proposals' include a 'Survey Monkey Link' for public to add their responses to a set of questions. Needs to be responded to before Dec 19th (see below) JG agreed to send on the suggested response as the questions were 'leading' and didn't provide much room to express real concern. LD to circulate to staff and patients group so it could be Due to high Demand the survey closing date has been extended to 9th January 2015. Please complete it and make your views known. Survey can be accessed here: http://www.surveymonkey.com/s/ncuhtsurvey communicated widely through local community. ACTION LD 2. North West Ambulance Service (NWAS) response to 999 ambulance requests. Currently, if the patient is in the surgery or if our GPs are with them at home, then NWAS 'deescalate' the call as the patients are deemed to be 'in a place of safety'. This can change an 8 minute response call to a 40 minute or longer response. This leads to major disruption in the surgery and potential delays in appropriate secondary care treatment. These events and other problems have all been notified to the Ambulance trust but the Practice have not received an acceptable reply and we are not sure if the CCG are handling these queries through their contract meetings with NWAS. If a patient resides in the top end of Eskdale, it could take 2 hours to get to Carlisle. 3. CQC Seascale were the first practice to be inspected under the new regime. Thank you to all those who provided comments. Inspectors commented that the practice and its connections with Community staff and rural population was unique and that they had not yet inspected 4 Seascale and Bootle Patient Participation Group anything similar. This reinforced the need to retain as many of the community services as possible to remain based in the surgery, i.e. DNs, Physio, Podiatry, Midwife, Health Visitor, Counsellors etc, as they could very easily be moved away from us. The practice haven't had another visit which is positive result. The inspectors were very reasonable. The report is available online at: http://www.cqc.org.uk/location/1-541106905 They gave us some positive feedback that we could in the practice. 4. GP Patient Survey The group reviewed the latest results. This is sent out each quarter from GP Survey and we always have a high number of patients who respond - thank you. Current results are available online https://gppatient.co.uk/practices/A82024?term=Seascale+Health+Centre+%28CA20+1PN%29 High levels of satisfaction are reported. A previous area of concern, i.e. Appointments, has improved and now 93% say the last appointment they got was convenient. Telephone Consultations are usually provided by the partners as they have know their patients best and the Locums are available to support and see patients who prefer not to have telephone consultations first. Partners still prefer to speak to patients before allocating them an appointment as they can advise if urine sample needed, patients should see nurse for tests or can avoid need for surgery visit altogether is patient can be supported over the telephone. One question that the practice feels they should improve is the Privacy in the Waiting and Reception area. Only 61% are satisfied with the level of privacy. We are considering moving the telephones into the back office. To avoid queues at the Reception desks, we have recently introduced the patient check in screens; over 1000 people have used it so far. We will move one of the computers and telephones into the back room and re- configure the work space. Online appointment booking (to open in Feb 2015) will hopefully mean there will be fewer phone calls and we have a plan to reduce Results phone calls also (see below). We are extremely grateful for a legacy donation from a patient and the Charity Committee have agreed that we can use some of these funds to improve this area. Occasionally, if the GP overruns, there is a wait. This was an issue for patients if they are using the 'community car service' and they have to leave before their appointment. We will ensure that Reception advise these patients if there is a delay so we will ask patients who use the Car Service to make this known to Reception when they arrive ACTION LD When we provided the flu clinics, patients were handed a small questionnaire and response about Service provision was overwhelmingly positive. 5 Seascale and Bootle Patient Participation Group 5. Friends and Family test This is introduced officially from 1st Dec 2014 but the practice has been gathering feedback from patients since Sept 2014. This allows patients to respond to the question 'would you recommend us to your friends and family?' So far results have been positive but we have had 2 comments about additional parking, despite having 22 spaces, this still seems to be an issue. Other comments: 'could we allow 2 months prescriptions at once? Could we have electronic opening doors into surgery? Can we improve the Options on the Telephone system to shorten length of time before getting through to Reception? All of these will be responded to with notices in the waiting room. LD asked if there were any other questions you would like to ask? Patient Group were happy with the final open ended question: ‘If we could change one thing about your care or treatment to improve your experience, what would it be’? Survey can be completed in practice using postcards or over practice website at: http://fft.mysurgeryintranet.co.uk/surveys/68/take-our-survey 6. Patient Access When we changed our Clinical system to EMIS web earlier this year, the 'online' services for patients are called Patient Access. Patients can order your repeat prescriptions online, view a summary of their medical record showing current medications, allergies and immunisations. 10% of practice patients are using it at the moment. 1500 patients regularly order their monthly repeat medications and around 650 are already registered to use Patient Access. We have been asked why we could not run the new and the old system at the same time. We couldn't do this because of the risk of receiving double requests and either dispensing twice or not at all. If patients are not yet registered, they can order on the telephone, then we will create new registration codes to log on in the next 14 days. We have asked for the system to be developed to nominate where patients would like to collect prescriptions: from the Pharmacy, Bootle or Seascale Dispensary Some patients have raised the issue with having separate accounts for all family members. We have explained that following RCGP guidance, it is not acceptable for a parent to have access to the records of their child over age of 16 for confidentiality reasons. We are guided to switch off access at 12 years old and the GP will decide on a case by case basis if access is appropriate between 12 & 16. If patients have problems with the system, or this decision, please contact the practice and we will try to help you through. We are looking at how we can provide electronic access to view 'Consultations', Test Results and letters in the future but this may take some time as we have lots of 'tidying' to do since our system changeover. Entries have not all transferred into the correct place. 6 Seascale and Bootle Patient Participation Group Whilst this isn't a risk to patient care as GPs and staff can still view without difficulty, when patients view these electronically, the 'viewer' heading are inconsistent. We will continue to work with EMIS to resolve this. 7. Results provision by Reception staff To improve use of GP time, we are investigating if Reception staff can provide results to patients that request these. A large number of telephone calls take place each day from patients enquiring if results are returned or from GPs advising patients that results are normal and there is no further action to take unless situations change. The group were asked if they would be satisfied if Reception staff dealt with these type of results? This will only be after a GP or Nurse has seen the result and provided an 'action' type reply to the Receptionist to pass on e.g. Normal, no further action, Satisfactory for patient, Retest is required, Please ask patient to book a further appointment etc. Reception staff will be trained by GPs on the types of results that can and cannot be given. Patient group were broadly in agreement that this is a sensible use of resources to free up GP time. Patient group advised that we would need to warn people before it happened. We would do this via WellWellWell, website and also from clinician to patient in consultation. To be started in the New Year. 8. AOB Ravenglass Road Closure - 30th Jan - 4th Feb, the main entrance road into village closed will be closed at the bridge. To access village, need to park in Ratty car park and walk over foot bridge. ACTION LD to Send message to CHOC & CPFT, NWAS that there will be 3 x 2 hours slots where no emergency access available. Dispensary delivery service, This needs to be driven by the local community but practice will support. Care Coordinators for Frail Elderly. We have two new care co-ordinators who visit patients in their home for initial assessment of needs, this has been welcomed by patients and will continue to at least Mar 15 when hopes are that this will be permanent roles in the practice Twitter. Practice now have a Twitter Account @SeascaleHC to broadcast general health and social care messages and share community information Millom hospital Update from NR - previously insufficient medical cover had stopped admissions. Millom community got together and have created the Millom health Alliance. GP surgery is now in the hospital. CPFT have purchased St Georges Hall to improve premises. Furness Commissioning Millom area with nursing supported from Barrow. 7 Seascale and Bootle Patient Participation Group Yoga now available at Eskdale. Britain’s Biggest Liar competition. Congratulations to Judith Gale, for winning 2nd place with a tale that was a wonderful attempt to address the serious issue of the WCH service move in a light hearted way. We will post her story on our website for you to enjoy. Thank you Judith! 8