apic05 - Sage Products Inc.
advertisement

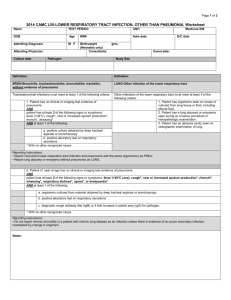
Improving Patient Safety, Clinical Quality and Unfunded Mandates: What ICPs Should Know Denise Murphy, RN, BSN, MPH, CIC Chief Patient Safety and Quality Officer Barnes-Jewish Hospital at Washington University Medical Center St. Louis, MO APIC 2005 Baltimore, MD Who Keeps Moving the Cheese? And WHY? Institute of Medicine Reports on Medical Errors (>100,000 lives lost annually) Quality Chasm (Safety, Government: Center for Medicare and Medicaid Services (CMS) Agency for Healthcare Research and Quality CDC Healthcare research Medical malpractice claims JCAHO sentinel event tracking Consumer’s Union and other advocacy groups Insurers: Pay4Performance Industry: Leapfrog Group I LOVE CHANGE! What Should ICPs Know About Quality Initiatives National Quality Forum, CMS, JCAHO and other agencies require patient safety and quality (PSQ) monitoring and reporting tied to reimbursement Consumers & payors demanding performance data Non- and for-profit organizations driving quality improvement (e.g., IHI, VHA) Infection prevention is included in improvement initiatives (local and national scorecards) What are Hospitals Responsible for in Terms of Quality & Compliance Indicators related to Clinical Quality Infection Prevention Patient Safety Operational Excellence and Customer Satisfaction Reporting Federal and State agencies, accreditation agencies, voluntary quality initiatives (AHA, IHI, etc.), insurers Governance boards Public reporting of hospital-acquired infections Reporting of other/all adverse events: stay tuned! Why Should ICPs Care? We are experts in monitoring, reporting and driving interventions related to adverse outcomes We are Quality Improvement and Patient Safety Professionals – organizational consultants, experts, and leaders in identifying risk mitigating and preventing adverse events If we bring our expertise to required, highly visible PSQ activities, we demonstrate our value to healthcare executives! WHAT IS BEING MEASURED Indicator and BY WHOM? ORYX/ CMS Core Measures -Current CMS/AHA & JCAHO Measures Anticipated Best-inClass 2004 Safety Culture1 Employee perception of management commitment to patient safety x Employee willingness to report errors x Patient Identification2 Surgical/procedural site ID compliance x Surgical/procedural time-out compliance x Patient rating of consistency of identification by care givers (survey) x Medication Safety2 Compliance with "Do Not Use" abbreviation list x Infection Control Trained medical direction in Infection Control x Antibiotic management program enhancements x Surgical patients receiving prophylactic antibiotic within standard x Hand hygiene policy and education x Reduce Catheter-related Bloodstream Infections in ICU (SIR < 1) x Reduce VAP Infections in ICU (SIR < 1) x Patient Identification Mislabeled/unlabeled lab specimens x Medication Safety Tall man lettering utilized at medication storage locations x NPSG Indicator JCAHO Core Measures Current JCAHO Core Measures Future Best-inClass 2005 CMS Annual Payment Update AMI Admission Treatment ASA within 24 hours of hospital arrival1 x x x Beta-blockers within 24 hours of hospital arrival1 x x x Cholesterol testing within 24 hours of hospital arrival x Discharge Treatment ACE-I/ARB prescribed at discharge for LV systolic dysfunction1 x x x ASA prescribed at discharge1 x x x Beta-blockers prescribed at discharge1 x x x Lipid-lowering agents prescribed at discharge x Reperfusion therapy within standard (Thrombolytic & PTCA)1 x x -Smoking cessation advice/counseling2 x x Inpatient mortality x Society of Thoracic Surgeons (STS) CABG ASA/antiplatelet prescribed at discharge x x Lipid-lowering agents prescribed at discharge x x ACE-I prescribed at discharge x Beta-blockers prescribed at discharge x Exercise program and/or cardiac rehabilitation therapy prescribed at discharge x Smoking cessation advice/counseling x x x Best-inClass 2005 CMS Annual Payment Update x x x Oxygenation assessment1 x x Initial selection of antibiotic x x Blood cultures before antibiotics2 x x Indicator JCAHO Core Measures Current JCAHO Core Measures Future CAP Antibiotic administration within 4 hours of hospital arrival1 Admission Treatment x Preventive Care Smoking cessation advice/counseling (adult/pediatric)2 x x Pneumococcal vaccine screening and/or vaccination1 x x Influenza vaccination3 x x x x x CHF ACE-I prescribed at discharge1 Antithrombotics Rx at discharge for patients with AFib x Discharge instructions2 x x LV function assessment1 x x Smoking cessation advice/counseling (adult)2 x x PCI ASA/antiplatelet prescribed at discharge x x x Indicator JCAHO Core Measures -Current JCAHO Core Measures - Future Best-inClass 2005 CMS Annual Payment Update SIP (Surgical Infection Prevention) Duration of prophylactic antibiotics3 x x x Duration of prophylaxis3 x x x Selection of antibiotic3 x x x Other HCAHPS (patient satisfaction survey)4 1 Publicly reported Q4 2003, Q1 2004 (Sept 2002 discharges) 2 Publicly reported beginning Q1 2005 (Q2 2004 discharges) 3 Publicly reported Summer 2005 (Q3 2004 discharges) 4 Publicly reported Fall/Winter 2005 (Q1 2005 discharges) x Indicator NPSG Improve accuracy of patient identification Use 2 patient identifiers when taking blood, administering medications or blood products, providing any other treatments or procedures x Prior to the start of any surgical or invasive procedure, conduct a final verification process, or "time out", to confirm correct pt., procedure, site using active communication techniques x Improve the effectiveness of communication among caregivers To verify telephone or verbal orders, or critical test results, the person receiving the order must "read back" the complete order or test result after transcription x Standardize abbreviations, acronyms and symbols used throughout the organization, including list of abbreviations, acronyms and symbols not to use x Measure, assess, and take action to improve the timeliness of reporting, and the timeliness of receipt by the responsible licensed caregiver of critical test results & values x Improve the safety of using medications Remove concentrated electrolytes (including, but not limited to, potassium chloride, potassium phosphate, sodium chloride >0.9%) from patient care units x Standardize and limit the number of drug concentrations available in the organization x Identify and, at a minimum, annually review a list of look-alike/sound-alike drugs x Eliminate wrong site, wrong patient and wrong procedure surgery Create and use a preoperative verification process, such as a checklist, to confirm that appropriate documents, (e.g., medical records, imaging studies) are available x Implement a process to mark the surgical site and involve the patient in the marking process x Indicator NPSG Improve the safety of using infusion pumps. Ensure free flow protection on all general use and PCA intravenous infusion pumps used in the organization x Improve the effectiveness of clinical alarm systems Implement regular preventive maintenance and testing of alarm systems x Assure that alarms are activated with appropriate settings and are sufficiently audible with respect to distances and competing noise within unit x Reduce the risk of healthcare-acquired infections Comply with current CDC hand hygiene guidelines x Manage as sentinel events all identified cases of unanticipated death or major permanent loss of function associated with a healthcare-acquired infection x Accurately & completely reconcile medications across the continuum of care Develop a process for obtaining & documenting a complete list of patient's current medications upon admission and with any involvement of the patient x A complete list of the patient's medications is communicated to the next provider of services when it refers or transfers a patient to another setting, service, practitioner or level of care x Reduce the risk of patient harm resulting from falls Assess & periodically reassess each patient's risk for falling, including the potential risk associated with the patient's medication regimen x Magnet Status *NDNQI Pressure ulcer prevalence x x Pressure ulcer occurrence x x Nursing care hours provided per patient day x x Nursing staff satisfaction x x Falls occurrence x x Fall injury occurrence x x - Nursing care x x - Pain management x x - Patient education x x - Overall care x x Skill mix of RN, LPN and unlicensed staff x x INDICATOR Patient satisfaction in relation to: *National Database of Nursing Quality Indicators Indicator ORYX/ CMS Core Measures Current CMS/AHA & JCAHO Measures Anticipated BestinClass 2004 Magnet/ NDNQI NQF Nursing-Sensitive Voluntary Consensus Standards Death among surgical inpatients with treatable serious complications (failure to rescue) X Pressure ulcer prevalence X x Falls prevalence X x Falls with injury X x Restraint prevalence (vest and limb only) X Urinary catheter-associated UTI for intensive care unit (ICU) patients X Central line catheter-associated blood stream infection rate for ICU and high-risk nursery (HRN) patients Ventilator-associated pneumonia for ICU and HRN patients X x x x Smoking cessation counseling for AMI x x Smoking cessation counseling for HF x x Smoking cessation counseling for pneumonia x x Skill mix (RN, LVN/LPN, UAP, and contract) x x Nursing care hours per patient day (RN, LPN, and UAP) x Practice Environment Scale - Nursing Work Index x x Indicator ORYX/ CMS Core Measures Current CMS/AHA & JCAHO Measures Anticipated BestinClass 2004 JCAHO ORYX ICU Measures Ventilator-Associated Pneumonia (VAP Prevention – Patient Positioning) x Stress Ulcer Disease (SUD) Prophylaxis x Deep Vein Thrombosis (DVT) Prophylaxis x x Central Line-Associated Primary Blood Stream Infection x x Risk-Adjusted ICU LOS by type of ICU x Risk-Adjusted Hospital Mortality for ICU Patients x x Magnet/ NDNQI PROPOSED 2006 NATIONAL PATIENT SAFETY GOALS Goal #10: Reduce Influenza and Pneumonia Develop and implement protocols for administration and documentation of influenza and pneumonia vaccination. Goal # 13: Achieve and Maintain an Organization-wide Safety Culture Assess Culture of Safety and take action on results of assessment Encourage external reporting of adverse events Use external or expert information when designing new or modifying existing processes to improve PS and reduce risk for sentinel events Share lessons learned from root cause analysis conducted by the organization with all staff who provide relevant services or may be impacted by proposed solutions Increase awareness of and access to relevant patient safety literature and advisories for all organizational leaders and staff Goal #14: Involve Patients in their Own Care as a Patient Safety Strategy Provide appropriate patient education to guide patient’s awareness and involvement in their own care. (Assess health literacy level, language skills, ethnic and cultural factors) Provide copy of medications to each patient and assist them in tracking/reconciling medications. Implement comprehensive patient involvement program Encourage patient participation in organization’s committees that relate to planning or providing patient care services Engage patients in the process of transitions across the continuum of care, including a dialogue about their expectations and concerns about the next setting of care Define and communicate the means to report concerns about safety and encourage pts. to do so PROPOSED 2006 NATIONAL PATIENT SAFETY GOALS Goal #16: Prevent Healthcare-Associated Decubitus Ulcers Assess and periodically reassess each patient’s risk for developing a decubitus ulcer (pressure sore) and take action to address any identified risks Identify patients who enter the organization with a decubitus ulcer and provide appropriate medical, physical and nutritional management to facilitate healing What is Interventional Patient Hygiene? Webster defines hygiene as the science and practice of the establishment and maintenance of health. Interventional Patient Hygiene is a nursing action plan directly focused on fortifying the patients host defense through use of evidencebased care. It works best with a protocol (action plan) and PIP (measurement) So What Can ICPs Do? KNOW the big picture of PSQ and where you and your program fit in Position yourself as a leader in your organization’s PSQ program…you are a Patient Safety Leader! Volunteer your expertise to teams addressing other types of adverse outcomes of patient care Data management, analysis and reporting Intervention development Education and literature interpretation Evaluation of products and technologies Science-based, cross-functional, multi-disciplinary approach to problem solving Get involved…WHY? ICPs are Safety, Quality and Performance Improvement EXPERTS! Now, it is my pleasure to introduce you to our session experts… Robert Garcia, BS, MMT(ASCP), CIC Deborah Trau, RN, 6 Sigma Black Belt to further address the role of infection prevention in improving patient safety and clinical quality The Role of Oral and Dental Colonization on Respiratory Infection: Call for New Interventions in a Patient Safety World Robert Garcia, BS, MMT(ASCP), CIC The Brookdale University Medical Center, Brooklyn, New York High Risk, High Morbidity, High Cost VAP Facts Mechanical ventilation increases risk of pneumonia 6-21 times (1% per day) Attributable mortality is 27% and increases to 87% when etiologic agent is P.aeruginosa or Acinetobacter sp. Length of stay with VAP is 34 days and 21 days without VAP Garcia R., A review of the possible role of oral and dental colonization on the occurrence of healthcare-associated pneumonia: Underappreciated risk and a call for interventions. Accepted for publication. AJIC 2005 12 Steps to Prevent Antimicrobial Resistance: Hospitalized Adults Step 11: Isolate the pathogen Hospital-Onset Infection Rates in NNIS Intensive Care Units, 1990-1999 Type of ICU BSI* VAP* UTI* Coronary Medical Surgical Pediatric 43% 44% 31% 32% 42% 56% 38% 26% 40% 46% 30% 59% * BSI = central line-associated bloodstream infection rate VAP = ventilator-associated pneumonia rate UTI = catheter-associated urinary tract infection rate Source: National Nosocomial Infections Surveillance (NNIS) System. 12 Steps to Prevent Antimicrobial Resistance: Hospitalized Adults Prevalence of Antimicrobial-Resistant (R) Pathogens Causing Hospital-Onset Intensive Care Unit Infections: 1999 versus 1994-98 Organism Fluoroquinolone-R Pseudomonas spp. 3rd generation cephalosporin-R E. coli Methicillin-R Staphylococcus aureus Vancomycin-R enterococci Imipenem-R Pseudomonas spp. # Isolates % Increase* 2657 1551 2546 4744 1839 49% 48% 40% 40% 20% * Percent increase in proportion of pathogens resistant to indicated antimicrobial Source: National Nosocomial Infections Surveillance (NNIS) System. ICU Rates of VAP, NNIS Study, Jan 2002-Jun 2004 Pooled means: Medical – 4.9 Med-Surg – 5.4 Surgical – 9.3 Cost of VAP Retrospective matched cohort study using data from large U.S. database 9,080 patients; 842 with VAP (9.3%) Patients with VAP had significantly longer duration of mechanical ventilation, ICU stay, and hospital stay. VAP associated with increase of >$40,000 in mean hospital charges Rello J et al., Epidemiology and outcomes of VAP in a large US database. Chest. 2002;122:2115-2121. HICPAC guidelines on preventing pneumonia Issued 3/26/04 Evidence-based Expert review Recommendations categorized www.cdc.gov/mmwr/preview/mmwrhtml/rr5303a1.htm HICPAC categories Category IA. Strongly recommended for implementation and strongly supported by well-designed experimental, clinical, or epidemiologic studies. Category IB. Strongly recommended for implementation and supported by certain clinical or epidemiologic studies and by strong theoretical rationale. Category IC. Required for implementation, as mandated by federal or state regulation or standard. Category II. Suggested for implementation and supported by suggestive clinical or epidemiologic studies or by strong theoretical rationale. No recommendation; unresolved issue. Practices for which insufficient evidence or no consensus exists about efficacy. Guideline for the Prevention of Intravascular-Associated Infections, CDC, 3/26/04. What strategies have been advocated in preventing VAP? Do not change routinely the ventilator circuit…Change the circuit when it is visibly soiled or mechanically malfunctioning. Cat. IA Heat Moisture Exchanger No recommendation can be made for the preferential use of either HMEs or heated humidifiers…Unresolved issue. No recommendation can be made about the frequency of routinely changing the in-line suction catheter of a closed suction system – Unresolved issue. Photographs courtesy of D. Ryan In the absence of medical contraindications, elevate at an angle of 30-45° the head of the bed of a patient…receiving mechanically assisted ventilation…Cat. II Stress Ulcer Prophylaxis Theory has it that modifying stomach acid effects the bacterial colonization level HICPAC: No recommendation can be made for the preferential use of sucralfate, H2-antagonists, and/or antacids for stress-bleeding prophylaxis in patients receiving mechanically assisted ventilation (unresolved issue). Livingston DH, Prevention of ventilator-associated pneumonia. Am J Surg. 2000;179(suppl 2A):12S-17S. “After all of this time and study, it is likely that neither drug has any advantage in significantly maintaining gastric flora and reducing VAP.” Selective Digestive Decontamination Preventive decolonization on the theory that the gut is a major source of VAP HICPAC: No recommendation can be made for the routine selective decontamination of the digestive tract (SDD) of all critically-ill, mechanically ventilated, or ICU patients (unresolved issue). 30+ studies to date Eggimann P, Pittet D. Infection control in the ICU. Chest 2001;120:2059-2093: “…This selective pressure on the epidemiology of resistance definitely precludes the systematic use of SDD for critically ill patients.” Weaning Duration, duration, duration!!! Cook D, Meade M, Guyatt G, Griffith L., Booker L, Criteria for Weaning from Mechanical Ventilation. Evidence Report/Technology Assessment No. 23 (Prepared by McMaster University under Contract No. 290-97-0017). AHRQ Publication No. 01-E010. Rockville MD: Agency for Health Care Research and Quality. November 2002. Evidence-Based Guidelines for Weaning and Discontinuing Ventilatory Support. A Collective Task Force Comprised of Members of the American College of Chest Physicians, the American Association for Respiratory Care and the American College of Critical Care Medicine. Chest 2001;120:375S-395S. Is there scientific evidence that links oropharyngeal and dental colonization with respiratory illness? Prevention or Modulation of Oropharyngeal Colonization HICPAC: Oropharyngeal cleaning and decontamination with an antiseptic agent: develop and implement a comprehensive oral-hygiene program (that might include the use of an antiseptic agent) for patients in acute-care settings or residents in long-term-care facilities who are at high risk for health-care-associated pneumonia. Cat. II Schleder B, Stott K, Lloyd RC, The effect of a comprehensive oral care protocol on patients at risk for ventilator-associated pneumonia. J Advocate Health 2002;4:27-30. Yoneyama T, et al., Oral care reduces pneumonia in older patients in nursing homes. J Am Geriatr Soc. 2002;50:430-3. 1. Oral Cavity vs. Gastric Colonization Prospective study of 86 mechanically vented ICU patients to assess relationship between oropharyngeal colonization and subsequent occurrence of pneumonia Patients oral and gastric specimens were collected on admission and twice weekly When pneumonia suspected, bronchoscopic specimens were taken with protected specimen brush In 31 cases of pneumonia identified, DNA genomic analysis demonstrated that oropharyngeal colonization was the predominant factor in the development of pneumonia compared with gastric colonization. Garrouste-Orgeas M, et al., Oropharyngeal or gastric colonization and nosocomial pneumonia in adult intensive care unit patients. A prospective study based on genomic DNA analysis. Am J Respir Crit Care Med. 1997;156:164. Acquired bacterial colonization: Location of the microorganisms in the 44 carrier patients Colonizing microorganisms Patients with OC Patients with GC Patients with BC Colonized patients A. baumanii 7 0 1 8 K. Pneumoniae 12 0 3 15 Enterobacteriaceae 9 5 8 22 Psuedomonadaceae 8 2 1 11 S. aureus 17 0 3 20 2 1 1 4 22 5 17 Enterococcus sp. Total OC = oropharyngeal colonization; GC = gastric colonization; BC = both OC/GC colonization Garrouste-Orgear M, et al., Am J Resp Crit Care Med 1997. Oropharyngeal Rather Than Gastric Colonization: Further Support Kerver AJ, et al., Colonization and infection in surgical intensive care patients – a prospective study. Intensive Care Med. 1987;13:347-51. Bonten MJM, et al., Risk factors for pneumonia, and colonization of respiratory tract and stomach in mechanically ventilated ICU patients. Am J Resp Crit Care Med. 1996;154:1339-46. Ewig S, et al., Bacterial colonization patterns in mechanically ventilated patients with traumatic head injury. Am J Resp Crit Care Med. 1999;158:188-98. 2. Decontamination of the Oropharynx Prospective, randomized, double-blind study of ICU patients to determine VAP while manipulating oropharyngeal colonization and without influencing gastric or intestinal colonization 87 given topical antibiotics (study group), 139 given placebo (control group) Results: VAP in study group: 10% VAP in control group: 27% Bergmans D, et al. Prevention of ventilator-associated pneumonia by oral decontamination. Am J Resp Crit Care Med. 2001;164:382-88. Additional Studies and Reviews Using Antibiotic Pastes or Solutions Rodriguez-Roldan JM, et al., Prevention of nosocomial lung infection in ventilated patients: use of an antimicrobial nonabsorbable paste. Crit Care Med. 1990;18:1239-42. Pugin J, et al., Oropharyngeal decontamination decreases incidence of ventilator-associated pneumonia: a randomized, placebo-controlled, double-blind clinical trial. J Am Med Assoc. 1991;265:2704-10. Bonten MJ, et al., Role of colonization of the upper intestinal tract in the pathogenesis of ventilatorassociated pneumonia. Clin Infect Dis. 1997;24:309-19. 3. Oral Decolonization: Use of Chlorhexidine Prospective, randomized, double-blind, placebo-controlled trial testing the effectiveness of oral decontamination on nosocomial infection 353 patients undergoing coronary bypass surgery Used chlorhexidine gluconate (0.12%) as oral rinse to prevent nosocomial infections Randomized to receive CHG or placebo Results: Overall reduction in nosocomial infections of 65% when using CHG Respiratory infections were reduced 69% in CHG group DeRiso AJ II, et al., Chlorhexidine gluconate 0.12% oral rinse reduces the incidence of total nosocomial respiratory infection and non-prophylactic systemic antibiotic use in patients undergoing heart surgery. Chest 1996;109:1556-61. 4. Link Between Oral Pathogens & Respiratory Infection A review article 6 articles cited as support for a relationship between poor oral health and respiratory infection Bacteria from colonized dental plaque may be aspirated into the lower airway Scannapieco, FA., Role of oral bacteria in respiratory infection. J Periodontol. 1999;70:794-802 5. Dental Plaque as a Bacterial Source of VAP Study on dental plaque colonization and ICU nosocomial infections. 57 patients studied Results: Dental plaque occurred in 40% of patients Colonization of dental plaque was highly predictive of nosocomial infection Salivary, dental, and tracheal aspirates cultures were closely linked Fourrier E, et al., Colonization of dental plaque: a source of nosocomial infections in intensive care patients. Crit Care Med. 1998;26:301-8. Additional Evidence Linking Colonized Dental Plaque and Respiratory Infection Scannapieco FA, et al., Colonization of dental plaque by respiratory pathogens in medical intensive care patients. Crit Care Med. 1992;20:740-45. Fitch JA, et al., Oral care in the adult intensive care unit. Am J Crit Care. 1999;8:314-18. Sumi Y, et al., Colonization of denture plaque by respiratory pathogens in dependent elderly. Gerontolog. 2002;9:25-9. Russel SL, et al., Respiratory pathogen colonization of the dental plaque of institutionalized elders. Spec Care Dentist. 1999;19:128-34. Major Areas of Oropharyngeal Colonization Lips & Gums Teeth Tongue Tissues Secretions A Case Study Reduction of Microbial Colonization in the Oropharynx and Dental Plaque Reduces VAP R Garcia, L Jendresky, L Colbert Brookdale University Medical Center, Brooklyn NY Abstract presented at the 2004 APIC Education Conference, Phoenix, AZ. The Brookdale University Medical Center Prioritization & Action Comparison of VAP rates with NNIS data indicated MICU rate above 50th percentile (6.0 cases per 1000 VD) Interventions taken prior to 2002 did not have sufficient effect to reduce rate below the benchmark ICP conducting VAP surveillance Interventional Epidemiology methodology applied: interviews and observations VAP Reduction Task Force Director of Nursing, Critical Care Nurse Manager, Critical Care Front Line Nurses Medical Director, Critical Care Emergency Room Physicians Respiratory Therapy Materials Management Infection Control Assessment Interviews of front line workers Observation of procedures Review of products Review of policies Review of literature, guidelines People Communication Between Providers Procedures Analysis of System Components Influencing the Occurrence of Ventilator-Associated Pneumonia Intubation/Extubation Physicians VAP surveillance rounds (observational periods between IC and nurses) Suctioning (closed/oral) Nurses Oral Care Respiratory Therapists Relay surveillance data to healthcare providers Cleaning & maintenance of ventilator and components Pharmacists Feedback from healthcare providers Handwashing Nutritional Specialists Placement & maintenance of nasogastric tube VAP Mechanical ventilator (Heated humidifier or HME) Vent circuits, filters Closed suction system, oral suction catheters, water, other suction devices, suction canisters/tubing Tracheostomy devices Nasogastric tubes Nebulizers Multidose vials Laryngoscopes Resusitation bags Definition of VAP Intubation/Extubation Self-extubation Closed suctioning Semi-recumbent positioning Handwashing Oral & Dental Care Cleaning of Use of H2 ventilator/other devices antagonists/sucralfate Tracheostomy care Ventilator circuits Filters Cleaning of laryngoscopes Nebulizers Suction canisters Enteral feeding Resuscitation bags Weaning Placement and care of nasogastric tubes Barrier equipment Equipment & Devices Policies Identification of Needs A uniform education program for nurses and respiratory therapists Standards for oral assessment Standards for oral care Standards for dental care Standardization of oral care solutions Keeping a closed system CLOSED Reduce environmental exposure Key Strategy #1: Education Handout created, includes answers to the following questions: Why is prevention of VAP important? What is hospital’s (unit’s) current rate? How do you compare with national benchmark? What are major interventions implemented to date? What role does bacterial colonization play in the development of respiratory infection? What new products/techniques will be implemented to address oral bacterial colonization? Tip: Applicable HICPAC Recommendation I. Staff Education and Involvement in Infection Prevention Educate health-care workers about the epidemiology of, and infection-control procedures for, preventing health-care—associated bacterial pneumonia to ensure worker competency according to the worker’s level of responsibility in the health-care setting, and involve the workers in the implementation of interventions to prevent health-care—associated pneumonia by using performance improvement tools and techniques. Cat IA Key Strategy #2: Reduce Oral and Dental Colonization Maintaining a Closed System Covered Yankauer Policy: Use as needed Yankauer Proper storage Keep yankauer covered when not in use Assists in decreasing the risk of environmental contamination Replace every day and PRN Suction Catheter Policy: Every 4 hrs. or as needed The device manufacturer does not market or approve of its use below the vocal cords Suction Toothbrush with Sodium Bicarbonate Policy: 2 X per day Suction Swab with Moisturizer Policy: Every 6 hrs. Feeling fuzzy??? Photographs courtesy of D. Ryan 0.0 Rate Mean Nov-04 Sep-04 Jul-04 May-04 Mar-04 Jan-04 Nov-03 Sep-03 Jul-03 May-03 Pre-intervention Period Mar-03 Jan-03 Nov-02 Sep-02 Jul-02 May-02 Mar-02 Jan-02 Nov-01 Sep-01 Jul-01 May-01 Mar-01 Jan-01 VAP per 1000 ventilator days VAP Rates, MICU, BUMC, 2001-2004 Post-intervention Period 25.0 20.0 15.0 10.0 5.0 VAP Rates, MICU, BUMC VENT DAYS RATE (VAP/ 1000 VD) % PTS WITH VAP PERIOD # PTS # VAP CASES Jan 2001Dec 2002 859 44 5262 8.3 5.1 Jan 2003Dec 2004 755 20 5147 3.8 2.6 Cost Avoidance Attributable cost of a healthcare-acquired pneumonia is estimated to be $40,000 (Rello, Chest, 2002). Based on the avoidance of approximately 10 VAP cases per year, BUMC estimates that the annual avoided extra cost to the institution to be: [10 x $40,000 (infection cost)] – [$56,606 (product cost)] = $343,394. Let’s Summarize VAP can be a serious and costly infection National quality initiatives are being directed specifically at this type of infection There now exists strong scientific evidence that controlling oropharyngeal colonization reduces respiratory disease in varied populations The speaker gratefully acknowledges the supreme effort of all the critical care nursing staff, the resident staff, and especially Mr. Trevor Grazette, Director of Nursing, Ms. Althea Bailey, Nurse Manager, and Ms. Henrietta Basanez, Nurse Educator. Robert Garcia, BS, MMT(ASCP), CIC Assistant Director of Infection Control Brookdale University Medical Center One Brookdale Plaza, Brooklyn, NY 11212 718-240-5924 rgarcia@brookdale.edu Utilizing Assessment and Interventional Strategies to Reduce the Risk of Skin Breakdown and Impact Patient Safety Debbie Trau, RN, 6 Sigma Black Belt OSF Saint Francis Medical Center Peoria, IL Applying 6 Sigma in Hospital Setting Quality improvement methodologies to enhance core patient care processes Define Measure Analyze Improve Control Reliability Unreliability “Sigma’s” (approximate) 0.9 10-1 1 0.99 10-2 2 0.999 10-3 3 0.9999 10-4 4 0.99999 10-5 5 0.999999 10-6 6 Reducing VAP with 6 Sigma, Nursing Management, June 2004 Prevalence vs. Incidence Rates How is one different than the other? Why does it matter? Why do we try to improve outcomes? Does JCAHO make us do this? Why We Are Here? Example: National average prevalence rate of pressure ulcers in acute care: 9% Clinical data: $500 -$50,000 average incremental costs per episode Pressure ulcers increase LOS by 2 to 5 times Average size hospital opportunity cost $400,000 to $700,000 Lyder C, Basic Pressure Ulcer Care. Advance for Providers of Post-Acute Care. March/April 2005. Beckrich K, Nursing Economic$, Sept/Oct 1999, Vol. 17, No. 5 Robinson C, et al., Ostomy/Wound Management 2003 Critical Issues Facing Hospitals PU’s are a growing cause of hospital morbidity and mortality Hospitals spend up to $5-$8.5 billion per year in incremental costs related to treating PU’s The trend towards Mandatory Reporting will require further quantification of PU incidence Regulatory agencies are making hospitals and their senior management accountable for infection control Beckrich K, Nursing Economic$, Sept/Oct 1999, Vol. 17, No. 5 Early Identification Stage I Stage II Stage III Stage IV A Stage I wound costs about $1 per day A Stage II wound jumps to $1,300 to $3,700 Stage III wounds can cost up to $50,000 The highest incidence is in acute care Key is to catch them early . . . Lyder C. Basic Pressure Ulcer Care. Advance for Providers of Post-Acute Care. March/April 2005. Early Identification Awareness of risk factors Tools to trigger Trained eyes always looking and communication with patient and family members (everyone is responsible) Thorough assessment of the patient by all members of the healthcare team Consistent scoring and communication tools Communication Transitioning from task to outcome focused Tools and resources for staff Documentation or is it a lack of documentation Outcomes to inspire staff or keep the momentum Our Patient’s Risk Factors Over 60 Incontinence Atherosclerosis Malnutrition Diabetes or other Obesity conditions that make skin more susceptible to infection Diminished sensation or lack of feeling Heart problems Paralysis or immobility Poor circulation Bedridden Spinal cord injury http://www.healthatoz.com/healthatoz/Atoz/ency/bedsores.jsp Empowering the Nursing Staff Quality issues for patient care Publicly reported scorecards Incorporate standardized assessment More importantly: Make it simple and easy for them to understand and implement What Simple Interventional Patient Hygiene Activities Affect Outcomes? Nurse-sensitive activities: 1. The bathing process for bed ridden patient 2. Incontinence cleansing and protection Why is the Bath Given? Social Control patient odor Provide patient well-being Bryant R, Rolstad B, Ostomy Wound Management 2001: 47(6), 18-27. Why is the Bath Given? Comfort Provide sensory stimulation Bryant R, Rolstad B, Ostomy Wound Management 2001: 47(6), 18-27. Why is the Bath Given? Health/Clinical Cleanse and moisturize the skin Reduce gross bacterial count Complete full skin assessment / monitoring Bryant R, Rolstad B, Ostomy Wound Management 2001: 47(6), 18-27. Who’s Providing the Bath? Non-licensed personnel? Are they trained and empowered to know what to look for? Who’s Providing the Care? How much more susceptible to injury and infection is the patient if this develops? What can we do? Bathing Process Solution Partner with Wound Care Nurse Empower non-licensed personnel Define 1. Issue 2. Expected outcome Provide 1. Training and education 2. Simple communication tools 3. Cleansing and moisturizing in one Measure, Analyze, Improve, Control Measure, Analyze, Improve, Control Incontinence Management Utilize the tools to “help us do our jobs” If it gets to this stage, it’s too late! Pilot Survey of Incontinence and Perineal Skin Injury Prevalence in Acute Care 35% with a Foley Catheter 3% 976 Total Number of Patients Surveyed Urinary Incontinence 13% Stool Incontinence 5% Dual Incontinence Sage Products Inc. Unpublished data 2005. Used with Permission. Pilot Survey of Incontinence and Perineal Skin Injury Prevalence in Acute Care 976 Total Number of Patients Surveyed 198 Number of Incontinent Patients 27% 33% 18% Perineal Dermatitis Pressure Ulcers Fungal Infection Sage Products Inc. Unpublished data 2005. Used with Permission. Incontinence Management Program Providing a skin protectant prophylactically Supported by the 1992 AHRQ guidelines Look for products that make it easy for the nursing staff. Products that save time Make cleaning and applying a skin barrier one easy step Early intervention prevention Incontinence Process Solution Partner with Wound Care Nurse Empower non-licensed personnel Define 1. Issue 2. Expected outcome Provide 1. Training and education 2. Cleansing and protection in one Measure, Analyze, Improve, Control Measure, Analyze, Improve, Control Quality Improvement Initiative Reduce PU Incidence Rates Early identification (the bath) Red skin is the warning sign Guaranteed communication between non- licensed and RN responsible (protocol) Measurements / Interventions (PIP) Outcome rather than task focused BACK to the BASICS approach Process Strategies for Change See what is out there: “Nurse I See Red” AHRQ guidelines Need a “believer” Highly motivated staff with administrative support Partner with companies that make it easy to do business with and can provide solutions Getting Started Education to non-licensed caregivers Triggers all caregivers in assessment and recognition Create a “safety net” for our patients Standardized practice strategy Assessment tool during the cleansing and each patient contact Use products that support your protocol Measuring Results and Celebrate your Success Drives compliance Personalize your rates Staff take ownership Benchmark against yourself Use the data to inspire staff or to keep the momentum Your Focus? Emphasis on outcomes rather than tasks! Study Guide on Interventional Patient Hygiene One CE Credit Debbie Trau, RN 6 Sigma Black Belt OSF Saint Francis Medical Center 530 NE Glen Oak, Peoria, IL 61637 (309) 671-1540 Deborah.A.Trau@osfhealthcare.org www.sageproducts.com