Abdominal Aortic Aneurysm
advertisement

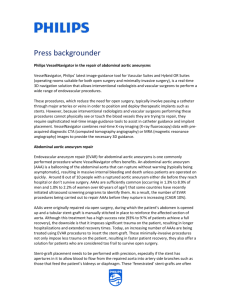
Abrupt Abdominal Pain HPI: C.B, a former heavy smoking 69 yo M with a h/o hypertension and COPD presents to the ED with sudden onset abdominal, lower back and R flank pain that started 45 min ago while at home watching TV. He also c/o feeling ‘dizzy’ and some nausea at the time. He denies LOC, chest pain, dyspnea, vomiting, difficulty urinating or blood in his stool. He has not ever had a pain like this before. The pain was a 9/10 initially, but is about a 6/10 after taking some Tylenol at home. His dizziness and nausea are improved at this time. ROS: HEENT: denies headache, visual changes CV: no chest pain Resp: denies dyspnea, chronic cough GI: Midline, peri-umbilical abdominal pain, nausea w/ pain initially, denies vomiting, diarrhea and blood in stool GU: no dysuria, hematuria Ext: denies leg pain, Some R flank and lower back pain Neuro: no LOC or weakness PMHx: COPD, Hypertension, Hyperlipidemia PSHx: appendectomy at age 20, ‘had a normal colonoscopy’ 3 years ago Medications: Spiriva, Metoprolol and hydralazine, simvastatin, Fish oil and daily multivitamin SocHx: Former 50 year 2 pack/day smoking history, has been smoke free for 6 months Moderate alcohol use Denies recreational drugs Married, retired truck driver FamHx: Mother – had hypertension Father – depression Brother – hypertension and ‘some surgery for an aneurysm’ Physical Exam Gen: mild distress HEENT: NCAT, PERRL, EOMI CV: RRR, no r/m/g, 2+ radial and dorsal pedis pulses Pulm: CTA, regular respirations Abd: mild peri-umbilical tenderness to palpation, pulsatile mass Ext: normal strength, no CVA tenderness Skin: no rashes or lesions Neuro: A&Ox3, no focal neuro deficits Differential Diagnosis? DDx: • Perforated viscus • Pancreatitis • Abdominal Aortic Aneurysm (AAA) • Urinary Calculi • Bowel obstruction • Musculoskeletal pain What would you order next? • Labs o o o o o o o Vitals Urine Hemoccult CBC Coagulation studies CMP Lipase and amylase • Imaging o Plain radiography o Abdominal Ultrasound o Abdominal CT w/ and w/o contrast if stable Results • Labs o Vitals – 100/60 115 37.5 97% on RA o Urine – normal o Hemoccult - negative o CBC 14 8.0 200 o PT/INR and PTT all normal o CMP - 140/ 4.0/ 100/ 24/ 15/ 1.0 / 95 o Lipase 25, Amylase 50, ALT 25, AST 35 Bedside Abdominal Ultrasound Imaging: Bedside US Imaging: Bedside US http://www.meddean.luc.edu/lumen/MedEd/Radio/curriculum/Surgery/aneurysm2.htm Abdominal CT http://www.medscape.com/content/2004/00/47/08/470838/470838_fig.html Diagnosis? Abdominal Aortic Aneurysm (AAA) • Bedside Abdominal US shows AAA 6.0 cm in • diameter Confirmed with Abdominal CT with contrast Treatment • C.B. is started on IVFs, given 02 by nasal • • cannula and vascular surgery is consulted Because of the sudden onset of pain, size of aneurysm, hypotension and feeling ‘dizzy’, there is concern C.B.’s AAA may be rupturing. He is admitted to vascular surgery for stabilization and urgent AAA repair. Abdominal Aortic Aneurysm Presentation • Flank, back or abdominal pain o • • • • • severe and abrupt onset, 50% describe pain as a ripping or tearing GI bleeding Syncope (10%) Extremity ischemia from embolization of a thrombus Shock: hemorrhagic Sudden death Atypical presentations may complicate the diagnosis: • • • • • Flank, groin or isolated quadrants of abdominal pain Nausea, vomiting Bladder pain Hip pain Tenesmus Diagnosis Physical Exam: Palpable abdominal mass (only present in 2%) Tender abdomen Hypotension Decreased femoral pulses Look for peri-umbilical ecchymosis (Cullen sign) or flank ecchymosis (Grey Turner sign), which indicate acute rupture Labs: H&H may not be affected • • • • • Treatment/Management • Symptomatic AAAs require an emergency vascular surgical consult for repair o o • Concurrent stabilization with IVFs, O2 and bedside diagnosis with US (>90% sensitive for demonstrating presence and measuring diameter Classic triad of symptom: abdominal and/or back pain, a pulsatile abdominal mass, and hypotension only occur in ~1/3 of patients with ruptured AAAs. Non-symptomatic AAAs o o o Prompt outpatient referral to vascular surgeon and BP control. AAAs between 4-5cm in diameter are associated with a 1% per year risk of rupture, monitoring every 6 months with US or CT scans. Any Aneurysm >5.5cm in diameter should be repaired. Gross Pathology - AAA Gross Pathology – Ruptured AAA Microscopic Images - AAA Fibrosis Inflammation A microscopic image of the abdominal aortic aneurysm shows intense inflammatory change and fibrosis in the adventitia (H and E, original magnification ×40). Microscopic Images - AAA Inflammatory cells are mainly lymphocytes, plasma cells, and eosinophils (H and E, original magnification ×400). Microscopic Images - AAA Obliterative phlebitis is observed (EvG, original magnification ×200) Microscopic Images - AAA Immunostaining of IgG4 reveals numerous IgG4-positive plasma cells within the lesion (immunostaining of IgG4, original magnification ×400). Bedside US Bedside US Imaging: Plain radiography http://www.meddean.luc.edu/lumen/MedEd/Radio/curriculum/Surgery/aneurysm2.htm CT without IV contrast Ruptured Abdominal Aortic Aneurysm an abdominal aortic aneurysm (A) with high density blood (arrows) indicating rupture. http://www.meddean.luc.edu/lumen/MedEd/Radio/curriculum/Surgery/aneurysm2.htm References: 1. 2. 3. 4. Prince LA, Johnson GA. Chapter 63. Aneurysms of the Aorta and Major Arteries. In: Tintinalli JE, Stapczynski JS, Cline DM, Ma OJ, Cydulka RK, Meckler GD, eds. Tintinalli's Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York: McGraw-Hill; 2011. http://www.accessmedicine.com/content.aspx?aID=6359748. Accessed November 6, 2012. Elefteriades JA, Olin JW, Halperin JL. Chapter 106. Diseases of the Aorta. In: Fuster V, Walsh RA, Harrington RA, eds. Hurst's The Heart. 13th ed. New York: McGraw-Hill; 2011. http://www.accessmedicine.com/content.aspx?aID=7836581. Accessed November 7, 2012. Images from http://www.meddean.luc.edu/lumen/MedEd/Radio/curriculum/Surgery/aneurysm2.htm Yasushi Matsumoto, Satomi Kasashima, Atsuhiro Kawashima, Hisao Sasaki, Masamitsu Endo, Kengo Kawakami, Yoh Zen, Yasuni Nakanuma, A case of multiple immunoglobulin G4–related periarteritis: a tumorous lesion of the coronary artery and abdominal aortic aneurysm, Human Pathology, Volume 39, Issue 6, June 2008, Pages 975-980, ISSN 0046-8177, 10.1016/j.humpath.2007.10.023. (http://www.sciencedirect.com/science/article/pii/S004681770700576X) Keywords: IgG4; Autoimmune pancreatitis; Retroperitoneal fibrosis; Aneurysm; Arteritis