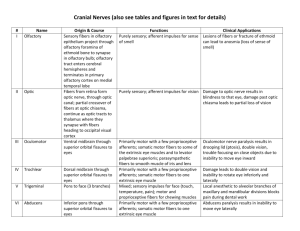
cranial nerves
advertisement

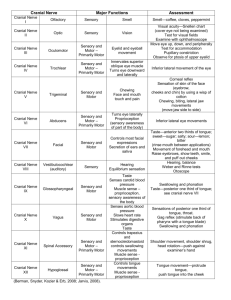
Brain Forebrain Midbrain ( brainstem) Hindbrain CN III, CN IV Cerebral hemispheres Pons (brainstem) CN I CN V Diencephalon (epithalamus, thalamus, hypothalamus Medulla oblongata (brainstem) CN IX, CN X, XII CN II Spinal Cord CN XI Cerebellum Cranial nerves can have: 1. Motor (efferent) fibers • Voluntary (striated) muscle • Involuntary(smooth) muscle or glands – by parasympathetic division of ANS: CN III, VII, IX, and X. • Preganglionic fibers emerge from brain and synapse in a parasympathetic ganglion outside CNS. • Postganglionic fibers continue to smooth muscle/glands. 2. Sensory (afferent) fibers • General sensation – touch, heat, pressure, etc. • Sensation from viscera (heart, GI tract, etc.) • Unique sensations – taste, smell, and those for vision, hearing, balance Cranial Parasympathetic ganglia GENERAL ORGANIZATION OF CRANIAL NERVES Olfactory Nerve : CN I Exits the nose → cribiform plate in ethmoid bone → olfactory bulb in anterior cranial fossa → olfactory tracts → cerebral cortex ∙sense of smell Fracture of ethmoid bone/ leisons of olfactory fibers may result in partial or totat loss of smell, anosmia [an-oz-me-ah]= an inability to detect odors) this may also dull the sense of taste. Anosmia may also be caused by the common cold, allergic rhinitis, frontal lobe tumors, trauma, aging. After head trauma, patient complains of runny nose (rhinnorhea): test nasal drip with dextrose or urine test strips --WHY? Fibers from nasal half of retina relay info from temporal field of that eye. Fibers from temporal half of the retina relay info from the nasal field of that eye. Nasal fibers cross at chiasm. http:// www.e-advisor.us/ visual_fields.php ciliary ganglion. Pupil Involvement with CN3: Oculomotor palsies often have pupillary involvement because the parasympathetic nerves innervating the iris travel with the third nerve. Pupillary involvement is a crucial diagnostic sign — compressive lesions tend to involve the pupil, while vascular lesions actually spare it! CN III palsy • Largest cranial nerve • Principal somatic sensory nerve to the face • Emerges from lateral pons by a large sensory and small motor rootsensory root leads to trigeminal ganglion. Motor root bypasses ganglion to become part of CN V3. Sensory Root: Ophthalmic (V1)– exits by sup orbital fissure to give sensation to cornea, skin of forehead, scalp, eyelids, nose. Ciliary ganglion associated with V1. Corneal reflex tests V1. Maxillary (V2)– exits by foramen rotundum to give sensation over maxilla, upper lip and teeth. Pterygopalatine (parasymatetic ) ganglion is associated with V2 lacrimal glands, glands of nose and palate. Mandibular (V3)– exits by foramen ovale to give sensation over mandible and lower lip and teeth, ant 2/3 of tongue. Otic and submandibular (parasymp) ganglia associated with V3. Motor Root: exits with V3 via foramen ovale to supply m. of mastication, mylohyoid, ant belly of digastric, tensor tympani and tensor veli palatini m. • Injury : by trauma (dental, cranial), tumors, aneurysms, infection (herpes zoster ophthalmicus) can all cause numbness • Paralysis of m of mastication with deviation of mandible toward side of lesionMotor branch of V3 Emerges from between pons and medulla exits through sup orbital fissure to enter the eye Supply motor fibers to lateral rectus m of eyeball (abducts eye) • • • supplies LR6: unable to look LATERALLY (OUTWARDS) develop double vision when looking to the side of the lesion medial deviation of eye Most caused by increased intracranial pressure or vasculopathic etiologies (Diabetes, Hypertension). • Greater petrosal n. • N. to stapedius • Chordae typmani n. • Somatic Motor fibers • Presynaptic Parasympathetic motor fibers Special Sensory fibers With a peripheral(LMN) 7th n lesion: paralysis of ALL facial muscles on IPSILATERAL side: pt cannot close eye, wrinkle that side of forehead or raise that corner of mouth = Bell’s Palsy With central (UMN) 7th n lesions: paralysis of LOWER facial muscles on CONTRALATERAL side (forehead wrinkling possible)--- ex common in stroke Other signs of 7th n lesions: loss of taste to anterior 2/3 of tongue; dry cornea equilibrium and motion hearing Lesions of CN VIII may cause: tinnitus (ringing of ears), vertigo (dizziness), loss of hearing. Lesions may involve either vestibular or cochlear or both divisions of CN VIII. Emerges from medulla jugular foramen Motor(efferent) fibers to stylopharyngeus, and presynaptic parasym fibers to Otic ganglion for parotid gland innervation. Sensory fibers to post 1/3 tongue for taste and general sensation, and sensory to pharynx, carotid sinus and body Lesions of CN IX: gag reflex absent on side of lesion or loss of taste on post 1/3 of tongue (i.e., infection/tumors). Tumors usually involve IX, X, XI –jugular foramen syndrome • Motor • Sensory Longest course and most extensive distribution of all cranial n. Pharyngeal Plexus of CN X • Pharyngeal Plexus of Vagus Nerve: network of nerve fibers innervating most of palate, larynx, and pharynx. Located on the surface of the middle pharyngeal constrictor muscle. Composed of fibers from CN IX, X, XI (all leave jugular foramen together) • Sensory Innervation: – Oropharynx and laryngopharynx • Motor Innervation: – – – – all muscles of pharynx(except stylopharyngeus (direct IX)) all muscles of soft palate(except tensor veli palatini(V3)) pharyngeal constrictors Palatoglossus (extrinsic tongue and palatine m) Arise as rootlets from the sides of the spinal cord pass through jugular foramen. Motor fibers to SCM and trapezius Arise from the medulla by rootlets exits cranium via hypoglossal canal runs inferiorly and anteriorly to tongue Motor fibers supply all extrinsic and intrinsic muscles of tongue except palatoglossus CN X: isolated lesions uncommon; paralysis of recurrent laryngeal n (cancer of larynx or thyroid gland; surgery) Injury of the recurrent laryngeal n: hoarseness, dysphonia due to paralysis of vocal cords Deviation of uvula to normal side CN XI: injury causes drooping of shoulder CNXII: injury causes paralysis to ipsilateral side of tongue—tongue deviates toward affected side Hypoglossal N Palsey: Isolated left LMN leison Anatomy of Cranial Nerves and foramina of skull: http://www.youtube.com/watch?v=US6oemgNHGQ Cranial Nerve and foramina quizzes/tutorials: http://www.gwc.maricopa.edu/class/bio201/cn/cranial .htm