Downloaded from www.cozaar.ae
RENAAL
Altering the Course of Renal Disease
in Hypertensive Patients with
Type 2 Diabetes and Nephropathy
with the AII Antagonist Losartan
Slide 1
Downloaded from www.cozaar.ae
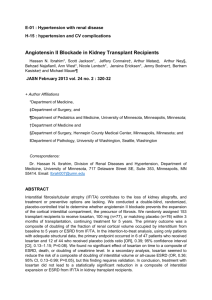
Angiotensin II Drives Pathology
in Hypertension
Vascular Dysfunction
Endothelial dysfunction
Remodeling/hypertrophy
Fibrosis
Tissue
Atherosclerosis
Cell loss
Hypertension
Dysfunction
Fibrosis
Remodeling
Ischemia
Heart
MI, HF
Kidney
ESRD
Brain
Stroke
Genetics, risk factors (diabetes, hypercholesterolemia)
Environment (diet, smoking, stress)
MI=myocardial infarction; HF=heart failure; ESRD=end-stage renal disease
Adapted from Weir MR, Dzau VJ Am J Hypertens 1999;12:205S-235S; Timmermans PB et al Pharmacol Rev 1993;45(2):
205-251; and Jessup M, Brozena S N Engl J Med 2003;348:2007-2018.
Slide 2
Downloaded from www.cozaar.ae
Clinical Endpoint Data for ESRD in Type 2
Diabetes with ACE Inhibitors Are Lacking
Endpoints Studied
ACE Inhibitor Trials
in Type 2 Diabetics
with >1 Year Follow-Up
Ravid et al Ann Intern Med 1993
Lebovitz et al Kidney Int 1994
Bakris et al Kidney Int 1996
Ahmad et al Diabetes Care 1996
Nielsen et al Diabetes Care 1997
UKPDS et al Br Med J 1998
Fogari et al J Hum Hypertens 1999
ABCD Diabetes Care 2000
Ruggenenti et al (REIN)
Total
Sample
Reduction of
Proteinuria
Reduction of Reduction in Risk
GFR Decline
of ESRD*
94
121
52
103
36
758
107
470
352 (27)**
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
No
No
Yes
Yes
No
No
No
No
No
No
No
No
Yes**
3577
Yes
No
Yes***
Am J Kidney Dis 2000
MICRO-HOPE**
Lancet 2000
GFR=glomerular filtration rate
*Reduction in the risk of end-stage renal disease (renal transplant or dialysis)
**Only 27 (8%) of the 352 patients in this study were Type 2 diabetics
***In this study there was no reduction of risk for renal dialysis for ramipril compared to placebo (p=0.70)
Slide 3
Downloaded from www.cozaar.ae
Controlling the Course of
Renal Disease with Losartan
Rationale for RENAAL (Losartan Renal Protection Study):
• Losartan significantly lowered BP comparable to other classes
of antihypertensive drugs
• Losartan demonstrated superior tolerability compared to other
classes of antihypertensive drugs (placebo-like side-effect profile)
• Losartan was a specific antagonist of angiotensin II (significant driver
of pathology in renal disease)
• Losartan had significant renoprotective effects in animal models
of renal disease
• Losartan was well tolerated and lowered BP in hypertensive patients
with renal insufficiency
BP=blood pressure
Adapted from Goa KL, Wagstaff AG Drugs 1996;51(5):820-845; Goldberg AI et al J Hypertens 1995;13(suppl 1):S77-S80;
Lafayette RA et al J Clin Invest 1992;90:766-771; Remuzzi A et al J Am Soc Nephrol 1993;4(1):40-49; Toto R et al Hypertension
1998;31:684-691.
Slide 4
Downloaded from www.cozaar.ae
Effect of Losartan on Microalbuminuria
Urinary albumin (mg/24 hr)
250
Type 2 diabetes
Type 1 diabetes
Renal transplant
Hypertension
200
211
188
173
153
150
115
100
83
92
94
57
50
21
0
15
n=29
30
22
n=12
60
37
40
39
n=10
n=194
66
55
15
n=9
n=103
n=424
n=14
n=8
n=40
Slide 5
Downloaded from www.cozaar.ae
RENAAL
Reduction of Endpoints in NIDDM with
the AII Antagonist Losartan
An investigator-initiated, multicenter, double-blind, randomized,
placebo-controlled study to evaluate the renal protective
effects of losartan in patients with Type 2
diabetes and nephropathy
1513 Patients; 250 Centers; 28 Countries
• Steering Committee
Chair
B. M. Brenner, MD
• Data and Safety Monitoring Committee
Chair
C. E. Mogensen, MD
• Clinical Endpoint Adjudication Committee
Chair
S. Haffner, MD
• Coordinating Center: Merck Research Labs
Study Director
S. Shahinfar, MD
Adapted from Brenner BM et al J Renin-Angiotens-Aldoster Syst 2000;1(4):328-334; Brenner BM et al N Engl J Med 2001;
345(12):861-869.
Slide 6
Downloaded from www.cozaar.ae
RENAAL
Primary Hypothesis
• Long-term treatment with losartan versus placebo (alone or
in combination with conventional antihypertensive therapy*)
in Type 2 diabetic patients with nephropathy will increase
the time to first event and decrease the incidence of
doubling of sCr, ESRD, or death
*Excluding ACE inhibitors and other AII antagonists
sCr=serum creatinine
Adapted from Brenner BM et al J Renin-Angiotens-Aldoster Syst 2000;1(4):328-334.
Slide 7
Downloaded from www.cozaar.ae
RENAAL
Secondary Hypothesis
• Losartan compared to placebo (alone or in combination
with conventional antihypertensive therapy*) in patients
with Type 2 diabetes and nephropathy will
– Increase the time to first event and decrease
the incidence of cardiovascular morbidity/mortality
– Reduce proteinuria
– Decrease the rate of progression of renal disease
*Excluding ACE inhibitors and other AII antagonists
Adapted from Brenner BM et al J Renin-Angiotens-Aldoster Syst 2000;1(4):328-334.
Slide 8
Downloaded from www.cozaar.ae
RENAAL
Study Design
Losartan 100 mg qd
(+CTx)
Losartan 50 mg qd
(+CTx)
Maintain conventional
antihypertensive therapy (CTx)*
Goal trough BP:
<140/<90 mmHg
n=1513
(excluding ACE inhibitors,
AII antagonists)
Placebo
(+CTx)
Losartan 100 mg qd (+CTx)
Placebo
(+CTx)
Placebo (+CTx)
6 wk
4 wk
8 wk
Mean follow-up 3.4 years
qd=once daily
*CTx=conventional therapy: Open-label calcium-channel blocker, diuretic, beta blocker, alpha blocker, or centrally acting agents.
Adapted from Brenner BM et al J Renin-Angiotens-Aldoster Syst 2000;1(4):328-334.
Slide 9
Downloaded from www.cozaar.ae
RENAAL
Inclusion/Exclusion Criteria
Inclusion criteria
Exclusion criteria
Type 2 diabetes
Type 1 diabetes
Age 31–70 years
Known non-diabetic renal
disease or renal artery stenosis
Proteinuria:
urine albumin:cr >300 mg/g
or 24-hr protein >500 mg
sCr:
1.3–3.0 mg/dl,
115–265 µmol/L*
Recent history of MI, CABG,
PTCA, CVA, TIA
History of HF
HbA1c >12%
CABG=coronary artery bypass graft; PTCA=percutaneous transluminal coronary angioplasty; CVA=cerebral vascular accident;
TIA=transient ischemic attacks
*Lower limit 1.5 mg/dl (133 µmol/L) in male patients >60 kg
Adapted from Brenner BM et al J Renin-Angiotens-Aldoster Syst 2000;1(4):328-334.
Slide 10
Downloaded from www.cozaar.ae
RENAAL
Enrollment by Region
N=1513
Asia
17%
North America
46%
Europe
19%
Latin America
18%
Adapted from Brenner BM et al J Renin-Angiotens-Aldoster Syst 2000;1(4):328-334.
Slide 11
Downloaded from www.cozaar.ae
RENAAL
Baseline Characteristics
Age, years
Male, %
Female, %
Race, %
Asian
Black
Caucasian
Hispanic
Other
Systolic BP, mmHg
Diastolic BP, mmHg
BMI, kg/m2
Losartan (+CTx)
(n=751)
Placebo (+CTx)
(n=762)
60
62
38
60
65
35
16
17
48
19
2
152
82
30
18
14
50
18
1
153
82
29
Adapted from Brenner BM et al J Renin-Angiotens-Aldoster Syst 2000;1(4):328-334.
Slide 12
Downloaded from www.cozaar.ae
RENAAL
Primary Composite Endpoint and Components
Composite
and components
Losartan (+CTx)
(n=751)
n (%)
Placebo (+CTx)
(n=762)
n (%)
p Value
% Risk
reduction
95% CI
DsCr, ESRD, Death
327 (43.5)
359 (47.1)
0.02
16
(2, 28)
DsCr
162 (21.6)
198 (26.0)
0.006
25
(8, 39)
ESRD
147 (19.6)
194 (25.5)
0.002
28
(11, 42)
Death
158 (21.0)
155 (20.3)
0.88
–2
(–27, 19)
ESRD or death
255 (34.0)
300 (39.4)
0.01
20
(5, 32)
DsCr=doubling of serum creatinine; CI=confidence interval
Adapted from Brenner BM et al N Engl J Med 2001;345(12):861-869.
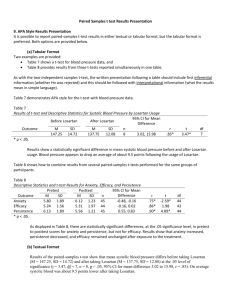
Slide 13
ESRD
% with event
30
20
10
RR: 28%
p=0.002
Doubling of sCr
30
0
0
12
24
36
48
Months
20
Placebo (+CTx) 762
Losartan (+CTx) 751
10
RR: 25%
p=0.006
50
0
0
12
24
36
48
Months
Placebo (+CTx) 762
Losartan (+CTx) 751
689
692
554
583
295
329
36
52
% with event
% with event
RENAAL
Primary Components
715
714
610
625
347
375
42
69
ESRD or Death
40
30
20
10
RR: 20%
p=0.010
0
sCr=serum creatinine; RR=risk reduction
Adapted from Brenner BM et al N Engl J Med 2001;345(12):861-869.
0
12
24
36
48
Months
Placebo (+CTx) 762
Losartan (+CTx) 751
715
714
610
625
347
375
42
69
Slide 14
Downloaded from www.cozaar.ae
RENAAL
Primary Composite Endpoint
Doubling of sCr / ESRD / Death
ITT analysis
% with event
50
40
40
30
30
20
20
RR: 16%
p=0.02
10
Per-protocol analysis
50
RR: 22%
p=0.008
10
0
0
0
Placebo (+CTx) 762
Losartan (+CTx) 751
12
689
692
24
Months
554
583
36
48
0
12
295
329
36
52
760
746
584
612
24
Months
431
479
36
48
214
263
24
36
Adapted from Brenner BM et al N Engl J Med 2001;345(12):861-869; Brenner B. Presented at 16th Annual Meeting of the American
Society of Hypertension, San Francisco, CA, USA, May 16–19, 2001.
Slide 15
Downloaded from www.cozaar.ae
RENAAL
Time to ESRD from Doubling of sCr
% with event
80
60
40
20
RR: 30%
p=0.013
0
0
6
12
18
24
Months
Placebo (+CTx) 198
Losartan (+CTx) 162
111
104
48
43
11
19
4
3
Adapted from Brenner B. Presented at 16th Annual Meeting of the American Society of Hypertension, San Francisco, CA, USA,
May 16–19, 2001.
Slide 16
Downloaded from www.cozaar.ae
RENAAL
BP (mmHg)
Systolic/diastolic
Losartan (+CTx)
Placebo (+CTx)
Mean arterial pressure
Losartan (+CTx)
Placebo (+CTx)
Pulse pressure
Losartan (+CTx)
Placebo (+CTx)
Baseline
Year 1
Year 2
Study End
152/82
153/82
146/78
150/80
143/77
144/77
140/74
142/74
105.5
106.0
100.9
103.1
99.1
99.7
95.9
96.8
69.4
70.8
67.8
69.8
66.2
67.1
66.7
67.4
Adapted from Brenner BM et al N Engl J Med 2001;345(12):861-869; Brenner B. Presented at 16th Annual Meeting of
the American Society of Hypertension, San Francisco, CA, USA, May 16–19, 2001.
Slide 17
Downloaded from www.cozaar.ae
RENAAL
Risk Reduction for Primary Composite Endpoint and
Components After Adjusting for Mean Arterial Pressure
DsCr/ESRD/Death
RR p Value
Unadjusted
Adjusted
16%
15%
0.02
0.03
ESRD
RR p Value
28%
26%
0.002
0.007
ESRD/Death
RR
p Value
20%
19%
0.01
0.016
Adapted from Brenner B. Presented at 16th Annual Meeting of the American Society of Hypertension, San Francisco, CA, USA,
May 16–19, 2001.
Slide 18
Downloaded from www.cozaar.ae
RENAAL
Dose of Losartan
• The daily dose of losartan ranged from 50–100 mg
Losartan*
n=751
%
100 mg qd
*Patients
71
who took the dose more than 50% of the time.
Adapted from Brenner B. Presented at 16th Annual Meeting of the American Society of Hypertension, San Francisco, CA, USA,
May 16–19, 2001.
Slide 19
Downloaded from www.cozaar.ae
RENAAL
Concurrent Antihypertensive Medications
Losartan
(n=751)
Placebo
(n=762)
Calcium-channel blocker, %
Dihydropyridine, %
77.9
60.7
81.1
63.9
Diuretic, %
83.8
84.0
Alpha blocker, %
40.2
45.7
Beta blocker, %
34.1
36.7
Centrally acting agents ,%
18.0
21.7
Therapeutic Class
Adapted from Brenner BM et al N Engl J Med 2001;345(12):861-869.
Slide 20
Downloaded from www.cozaar.ae
RENAAL
Secondary Composite Endpoint
and Components
Composite
and components
Losartan (+CTx)
(n=751)
n (%)
CV morbidity/mortality
Placebo (+CTx)
(n=762)
n (%)
p Value
% Risk
reduction
95% CI
247 (32.9)
268 (35.2)
0.255
10
(–8, 24)
CV death
90 (12.0)
79 (10.4)
0.455
–12
(–52, 17)
HF
89 (11.9)
127 (16.7)
0.005
32
(11, 48)
MI
50 (6.7)
68 (8.9)
0.079
28
(–4, 50)
Unstable angina
42 (5.6)
41 (5.4)
0.881
–3
(–59, 33)
Stroke
47 (6.3)
50 (6.6)
0.787
5
(–41, 36)
Revascularization
69 (9.2)
60 (7.9)
0.331
–19
(–68, 16)
CV=cardiovascular
Adapted from Brenner BM et al N Engl J Med 2001;345(12):861-869.
Slide 21
Downloaded from www.cozaar.ae
RENAAL
First Hospitalization for Heart Failure
% with event
20
15
10
5
Risk reduction: 32%
p=0.005
0
0
12
24
36
48
375
388
53
74
Months
Placebo (+CTx) 762
Losartan (+CTx)751
685
701
616
637
Adapted from Brenner BM et al N Engl J Med 2001;345(12):861-869.
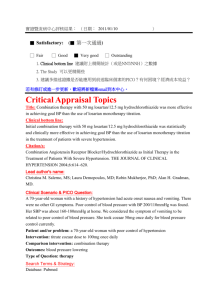
Slide 22
Downloaded from www.cozaar.ae
RENAAL
Change from Baseline in Proteinuria
Median % change
40
20
0
–20
–40
35% Overall reduction
p<0.001
–60
0
12
24
36
48
390
438
130
167
Months
Placebo (+CTx) 762
Losartan (+CTx)751
632
661
529
558
Proteinuria measured as the urine albumin:creatinine ratio from a first morning void.
Adapted from Brenner BM et al N Engl J Med 2001;345(12):861-869.
Slide 23
Downloaded from www.cozaar.ae
RENAAL
Rate of Progression of Renal Disease
(median 1/sCr slope)
p=0.01
18% reduction
–0.08
dl/mg/yr
–0.06
–0.069
–0.056
–0.04
–0.02
0
Losartan (+CTx)
Placebo (+CTx)
Adapted from Brenner BM et al N Engl J Med 2001;345(12):861-869.
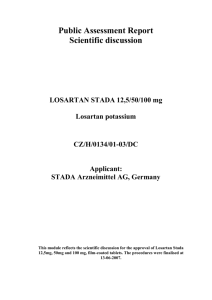
Slide 24
Downloaded from www.cozaar.ae
RENAAL
Most Common Clinical and Laboratory Adverse
Experiences Leading to Discontinuation of Study Therapy
6
Percentage
6
4
Losartan (+CTx)
Placebo (+CTx)
3
3
2
2
2
2
1
1
1
1
1
1
1
0.4
0
Heart
failure
ESRD
MI
Clinical
Stroke
Worsening
renal
insufficiency
sCr
Hyperkalemia
Laboratory
Adapted from Brenner B. Presented at 16th Annual Meeting of the American Society of Hypertension, San Francisco, CA, USA,
May 16–19, 2001.
Slide 25
Downloaded from www.cozaar.ae
Public Health and Economic Implications
of RENAAL (US)
• For diabetic patients at risk over a 3.5-year period, it is
estimated that
– Addition of losartan to the treatment regimens of 100 patients
with Type 2 diabetes and nephropathy would be expected to
lead to a reduction of 6.3 cases of ESRD
– In RENAAL, losartan reduced ESRD days by 31%
• Reduction in days with ESRD saves $5144 (p=0.003) per treated
patient at 3.5 years and $7058 (p=0.002) per patient over 4 years
• After accounting for costs of losartan, reduction in ESRD resulted
in net savings of $3522 per patient over 3.5 years (95% CI:
$143–$6900) and $5298 (95% CI: $954–$9643) per patient
over 4 years
Costs are reported in 2001 US dollars.
Adapted from Herman WH et al Diabetes Care 2003;26(3):683-687.
Slide 26
Downloaded from www.cozaar.ae
Public Health and Economic Implications
of RENAAL (EU)
• Extrapolating the addition of losartan to the treatment regimen
of patients with Type 2 diabetes and proteinuria in the EU
– 44,092 cases of ESRD averted (95% CI: 11,898–76,286)
after 3.5 years
– 64,383 years with ESRD averted (95% CI: 20,886–107,879)
after 3.5 years
– Reduction in ESRD-related costs of €2.6 billion after 3.5 years,
increasing to €3.6 billion after 4 years
Costs based on ESRD costs in Germany in 1999.
Adapted from Gerth WC et al Kidney Int 2002;62(suppl 82) S68-S72.
Slide 27
Downloaded from www.cozaar.ae
RENAAL
Summary (I)
• In patients with Type 2 diabetes and nephropathy
– Losartan delayed onset of the primary composite
endpoint (DsCr/ESRD/Death) and delayed
progression to ESRD
– Losartan reduced proteinuria and the rate of decline
in renal function (assessed by the reciprocal of
sCr concentration)
– Losartan reduced the incidence of first hospitalization
for heart failure
– These benefits were largely independent of BP
Adapted from Brenner BM et al N Engl J Med 2001;345(12):861-869.
Slide 28
Downloaded from www.cozaar.ae
RENAAL
Summary (II)
• In patients with Type 2 diabetes and nephropathy
– Losartan and placebo, added to CTx, showed no
significant difference in all-cause mortality, MI,
stroke, revascularization, hospitalizations for
unstable angina, and death due to CV disease
– Losartan was generally well tolerated in this
patient population
Adapted from Brenner BM et al N Engl J Med 2001;345(12):861-869.
Slide 29
Downloaded from www.cozaar.ae
RENAAL
Conclusions
• Losartan conferred significant benefits on renal
outcomes in Type 2 diabetic patients with nephropathy
• Losartan therapy resulted in a significant reduction
in first hospitalizations for heart failure
• These benefits of losartan were independent of
achieved BP control
• Losartan was generally well tolerated
Adapted from Brenner BM et al N Engl J Med 2001;345(12):861-869.
Slide 30
Downloaded from www.cozaar.ae
RENAAL
Losartan Renal Protection Study
• RENAAL results show that losartan + CTx
– Provided excellent tolerability
– Provided proven renal protection and cardioprotective
benefit
28% risk reduction in ESRD
32% risk reduction in incidence of first hospitalization
for heart failure
35% reduction in proteinuria
• Analysis of the public health implications of RENAAL
suggested potential of losartan for substantial healthcare
savings
Adapted from Brenner BM et al N Engl J Med 2001;345(12):861-869; Herman WH et al Diabetes Care 2003;26(3):683-687;
Gerth WC et al Kidney Int 2002;62(suppl 82):S68-S72.
Slide 31
Downloaded from www.cozaar.ae
Why Is RENAAL Relevant to the
Treatment of Hypertension?
• High BP causes increased risk for cardiac, renal and
cerebrovascular events (MI, HF, ESRD, stroke)
• RENAAL provided strong evidence of a need to block
the pathological effects of angiotensin II beyond BP
• RENAAL demonstrated that specific AII blockade with
losartan in hypertensive patients with Type 2 diabetes
and nephropathy helps control the course of disease and
delays ESRD
• RENAAL demonstrated that losartan provides renal
protection and a cardioprotective benefit
Adapted from Whelton PK et al J Hypertens 1992;10(suppl 7):S77-S84; MacMahon S et al Lancet 1990;335:765-774; Kannel WB
JAMA 1996;274(24):1571-1576; Klag MJ et al N Engl J Med 1996;334:13-18; Brenner BM et al N Engl J Med 2001;345(12):
861-869.
Slide 32
Downloaded from www.cozaar.ae
Losartan Endpoint Trials
ELITE II—The losartan heart failure survival study
No significant difference was observed between treatment with losartan
or captopril on all-cause mortality in HF patients, but losartan was
significantly better tolerated
RENAAL—The losartan renal protection study
Losartan provided renal protection and a cardioprotective benefit
with excellent tolerability
LIFE—The losartan hypertension survival study
Losartan provided protection against stroke and new-onset diabetes
OPTIMAAL—The losartan post-MI survival study
Losartan provided cardiovascular benefits comparable to captopril
ELITE=Evaluation of Losartan in the Elderly; LIFE=Losartan Intervention For Endpoint reduction; OPTIMAAL=Optimal Trial in
Myocardial Infarction with the Angiotensin II Antagonist Losartan
Adapted from Pitt B et al Lancet 2000;355:1582-1587; Brenner BM et al N Engl J Med 2001;345(12):861-869; Dahlöf B et al
Lancet 2002;359:995-1003; Dickstein K et al Lancet 09/01/02; available at http://image.thelancet.com/extras/02art6111web.pdf.
Slide 33
Downloaded from www.cozaar.ae
References
Please refer to notes page.
Slide 34
Downloaded from www.cozaar.ae
References (cont’d)
Please refer to notes page.
Slide 35
Downloaded from www.cozaar.ae
References (cont’d)
Please refer to notes page.
Slide 36
Downloaded from www.cozaar.ae
Before prescribing, please consult
the manufacturers’ prescribing information.
Merck does not recommend the use of any product
in any different manner than as described
in the prescribing information.
Copyright © 2003-2004 Merck & Co., Inc., Whitehouse Station, NJ, USA.
All rights reserved.
5-05 CZR 2001-W-6747-SS
Printed in USA
VISIT US ON THE WORLD WIDE WEB AT http://www.merck.com
Slide 37