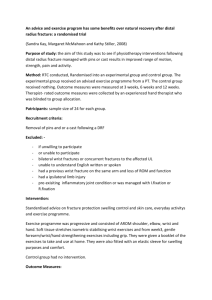
51 yo M with R Shoulder pain s/p humeral head replacement 10
advertisement

59 y/o male with ulnar sided wrist pain 59 y/o male with ulnar sided wrist pain 59 y/o male with ulnar sided wrist pain 59 y/o male with ulnar sided wrist pain 59 y/o male with ulnar sided wrist pain 59 y/o male with ulnar sided wrist pain 59 y/o male with ulnar sided wrist pain TFC Tear • • • • • • • • • • Palmer classification for triangular fibrocartilage complex abnormalities Class 1: Traumatic A - Central perforation B - Ulnar avulsion C - Distal avulsion D - Radial avulsion with or without sigmoid notch fracture Class 2: Degenerative (ulnocarpal abutment syndrome) stage A - TFCC wear B - TFCC wear with lunate and/or ulnar chondromalacia C - TFCC perforation with lunate and/or ulnar chondromalacia D - TFCC perforation with lunate and/or ulnar chondromalacia and LT ligament perforation E - TFCC perforation with lunate and/or ulnar chondromalacia, LT ligament perforation, and ulnocarpal arthritis 30 y/o female with clinical hx of left-sided trunk/thigh hypertrophy? 30 y/o female with clinical hx of left-sided trunk/thigh hypertrophy? 30 y/o female with clinical hx of left-sided trunk/thigh hypertrophy? 30 y/o female with clinical hx of left-sided trunk/thigh hypertrophy? 30 y/o female with clinical hx of left-sided trunk/thigh hypertrophy? 30 y/o female with clinical hx of left-sided trunk/thigh hypertrophy? Absent vs. Atrophic Piriformis muscle? • 1) Piriformis muscle might be absent and there might be variations in origin and insertion sites of some muscles and their relation with regional nerves of this region. Bannister L, Berry M, Collins P, Dyson M, Dussek J : Muscles of the thigh and gluteal region. In. Williams P (ed): GrayÕs Anatomy. 38 th ed. London: Churchill Livingstone, 1995 : 875-878 2) Lee CS, Tsai TL : The relation of the sciatic nerve to the piriformis muscle. Taiwan I Hsueh Hui Tsa Chih 1974; 73 : 75-80. 27 y/o male with twisting ankle injury while hiking 27 y/o male with twisting ankle injury while hiking 27 y/o male with twisting ankle injury while hiking Achilles Avulsion • Greek mythology relates that the legendary warrior Achilles was made invincible by his mother Thetis, who dipped him in the River Styx while holding him by his heel. Because his heel was never immersed, it remained his one area of vulnerability. After the fall of Troy, Achilles met his demise when he was shot in the heel by Paris, whose arrow was guided by the Greek god Apollo. This is the derivation of the term "Achilles tendon." Achilles Avulsion • However, Achilles avulsion is considered rare, usually occuring at the calc. tubercle. • Possible causes: • Traumatic dorsiflexion in maximally plantar flexed foot • Contraction of triceps surae during knee extention in a sprint • Direct blow The heel of achilles: calcaneal avulsion fracture from a gunshot wound. Cooper DE, Heckman JD Foot Ankle. 1989 Feb;9(4):204-6 34 y/o MLB pitcher with shoulder pain 34 y/o MLB pitcher with shoulder pain 34 y/o MLB pitcher with shoulder pain 34 y/o MLB pitcher with shoulder pain Thrower’s Shoulder Elbow pain 55 yr old man pre post Elbow pain 55 yr old man Bicipitoradial Bursa Cubital Bursae • • bicipitoradial bursa interosseous bursa Bicipitoradial Bursitis: MR Imaging Findings in Eight Patients and Anatomic Data from Contrast Material Opacification of Bursae Followed by Routine Radiography and MR Imaging in Cadavers1 Abdalla Y. Skaf, MD, Robert D. Boutin, MD, Robert Weiber M. Dantas, MD, Andrew W. Hooper, MD, Claus Muhle, MD, David S. Chou, MD, Nittaya Lektrakul, MD, Debra J. Trudell, RA, Parviz Haghighi, MD and Donald L. Resnick, MD 1 From the Departments of Radiology (A.Y.S., R.D.B., R.W.M.D., A.W.H., C.M., D.S.C., N.L., D.J.T., D.L.R.) and Pathology (P.H.), Veterans Affairs Medical Center and University of California San Diego, 3350 La Jolla Village Dr, San Diego, CA 92161. Bicipitoradial Bursa • reduces friction between the biceps tendon and the radial tuberosity Bursitis • • • • • • Repetitive mechanical trauma Infection Inflammatory arthropathy Chemical synovitis Bone proliferation Elbow Pain Torn Biceps Tendon Cubital Bursitis Supinator muscle edema • Mass effect in the cubital tunnel may compress the branches of the radial nerve Posterior Interosseous Nerve Syndrome • Compression of the deep branch of the radial nerve • innervates multiple extensor muscles • extensor indicis proprius, extensor digiti quinti, extensor carpi ulnaris, abductor pollicis longus, extensor pollicis brevis, and extensor digitorum communis muscles 34 yo Hockey player SLAP tear with possible extension into the SGHL and MGHL 33 yo woman 33 yo woman osteopenia, cartilage loss, and erosions, subluxation Rheumatoid Arthritis Same patient OA pattern • Superolateral joint space narrowing • Marginal osteophytes • Eburnation and subchondral cystic change Why the early OA? Femoral Acetabular Impingment? Crystal deposition disorders? 19 yr old Marine with new onset difficulty performing pull-ups 19 yr old Marine with new onset difficulty performing pull-ups Suprascapular Nerve Entrapment • • • At suprascapular notch, will involve both the supra- and infraspinatus muscles At the spinoglenoid notch, involves only the infraspinatus Most common cause is a ganglion cyst from a superior labral tear 36 year old man with arm and hand numbness for one day 36 year old man with arm and hand numbness for one day • Patchy scattered foci and muscular edema • Considerations • • Parsonage Turner syndrome Quadrilateral space syndrome Post op day 1 from ventral hernia repair • Other considerations • Positioning neuropathy T2 T1-PRE POST T2 T1 PRE T1 POST SOFT TISSUE MASS: VOLAR DISTAL PHALANX • • • • • • • Ganglion cyst 50% to 70% Hemangioma/vascular malformation Giant cell tumor Glomus tumor Mucoid (epidermoid) cyst Epidermoid Nerve sheath tumor Benign tumors of fibrous tissue origin • • • • • Nodular fasciitis Neurofibroma Schwannoma Fibrous histiocytoma Fibroma/ fibromatosis Nodular fasciitis • • • Most common soft tissue lesion originating from fibrous tissue 50% arise in the upper extremity, m/c volar forearm Present as a rapidly growing mass Enzinger FM, Weiss SW. Soft tissue tumors. St Louis: Mosby, 1995. Nodular fasciitis • Histologically often misdiagnosed because of its rapid growth, increased cellularity and mitotic activity Nodular fasciitis • Thee subtypes • Subcutaneous • • Intramuscular • • Subcutanous nodule Large, deep, mimics a soft tissue malignancy Intermuscular • Irregular/ stellate appearance, mimics inflammatory lesion MR characteristics • • Variable depending on the amount of collagen, cellularity, and mucin. Subcutaneous lesions to occur in younger patients and exhibit myxoid histology and increased T2 signal. Wang et al., Nodular fasciitis: correlation of MRI findings and histopathology. Skeletal Radiol. 2002 Mar;31(3):155-61. 69 y.o. male with possible fracture of 1st proximal Axial T1 FS nd phalanx and gout of 2 digit. Axial T1 FS/Gd Axial T2 FS Axial T1 69 y.o. male with possible fracture of 1st proximal phalanx and gout of 2nd digit. Cor T2 FS Cor T1 FS/Gd 69 y.o. male with possible fracture of 1st proximal phalanx and gout of 2nd digit. Sag T1 69 y.o. male with possible fracture of 1st proximal phalanx and gout of 2nd digit. Sag T1 69 y.o. male with possible fracture of 1st proximal phalanx and gout of 2nd digit. Sag T1 69 y.o. male with possible fracture of 1st proximal phalanx and gout of 2nd digit. Sag T1 FS/Gd 69 y.o. male with possible fracture of 1st proximal phalanx and gout of 2nd digit. Sag T1 FS/Gd 69 y.o. male with possible fracture of 1st proximal phalanx and gout of 2nd digit. Sag T1 FS/Gd Gout • MRI of Tophi • • • Low on T1WI On T2WI usually variable but contain lowsignal regions High signal on post Gd Yu et al, MR imaging of tophaceous gout. AJR Am J Roentgenol. 1997 Feb;168(2):523-7. Weishaupt et al, MR imaging of inflammatory joint diseases of the foot and ankle. Skeletal Radiol. 1999 Dec;28(12):663-9. 20 yo minor league baseball player with history of aspergillus Axial T1 Recurrent pain and swelling in the hand and infection 1 yr ago. wrist. Axial T1FS/Gd 20 yo minor league baseball player with history of aspergillus infection 1 yr ago. Recurrent pain and swelling in the hand and wrist. Axial T2 FS 20 yo minor league baseball player with history of aspergillus infection 1 yr ago. Recurrent pain and swelling in the hand and wrist. 20 yo minor league baseball player with history of aspergillus infection 1 yr ago. Recurrent pain and swelling in the hand and wrist. 20 yo minor league baseball player with history of aspergillus infection 1 yr ago. Recurrent pain and swelling in the hand and wrist. 20 yo minor league baseball player with history of aspergillus infection 1 yr ago. Recurrent pain and swelling in the hand and wrist. 20 yo minor league baseball player with history of aspergillus infection 1 yr ago. Recurrent pain and swelling in the hand and wrist. Chronic Infection and Synovial Hypertrophy • D.Dx. • • Fungus TB ( Mycobacterium marinum) Mycobacterium Infection Recurrent Mycobacterium marinum tenosynovitis of the wrist mimicking extraarticular synovial chondromatosis on MR images. Lee EY, Rubin DA, Brown DM. Skeletal Radiol. 2004 Jul;33(7):405-8. Epub 2004 May 04. Tenosynovitis caused by atypical mycobacterial infections may produce rice bodies within affected tendon sheaths. …. the flexor tendons within the carpal tunnel in which the rice bodies were mistaken for synovial chondromatosis on MR images Horseshoe Abscess Diagnosis of Bone and Joint Disorders, Resnick Hand – Pathways of infection, pg 2399 21yo F with hand pain. History of bilateral THA and TKA. 21yo F with hand pain. History of bilateral THA and TKA. 21yo F with hand pain. History of bilateral THA and TKA. 21yo F with hand pain. History of bilateral THA and TKA. 21yo F with hand pain. History of bilateral THA and TKA. 21yo F with hand pain. History of bilateral THA and TKA. Juvenile Chronic Arthritis Portrait of a Youth Botticelli, 1483 Juvenile –onset adult type RA • • • • • Female >10yrs Polyarticular Possible subQ nodules and vasculitis Seropostive for RA Diagnosis of Bone and Joint Disorders, 3rd ed. D Resnick, editor. W.B. Saunders Co., Philadelphia, 1995. Juvenile –onset adult type RA • • • • • • • MCP and IP joints of hand Wrist Knee MTP and IP joints of foot Cervical spine Hip Shoulder Juvenile –onset adult type RA • • • • • • • • • Soft tissue swelling Osteoporosis Periostitis Erosions, especially in the absence of joint space loss Possible joint space loss Atlanto Axial Subluxation Epiphyseal compression fractures Joint Subluxation Growth disturbances 73 y.o F with wrist pain and stiffness 73 y.o F with wrist pain and stiffness 73 y.o F with wrist pain and stiffness Rheumatiod Arthritis vs Psoraisis Interesting Wrist Case • • Dorsal Midcarpal Instability Carpal Instability Non Dissociative (CIND) UCSD Bone Conference June 3, 2005 Jeremy Kuniyoshi 57 yo M with increasing thigh mass X 2-3 months Further Hx: Infected hematoma post cath many yrs ago On anticoag for prosthetic valves (INR 1.6) 57 yo M with increasing thigh mass X 2-3 months 57 yo M with increasing thigh mass X 2-3 months 17964259.jpg COR T1 SAG STIR AX PD FS 17964259.jpg T1 POST T1 FS POST T1 FS POST AX T1 POST 57 yo M with increasing thigh mass X 2-3 months Surgical Pathology Report: Fibrous Capsule with areas of granulation tissue, multinucleated giant cells, areas of necrosis, and hemorrhage with clot c/w pseudoaneurysm Popliteal vascular malformation simulating a soft tissue sarcoma Wambeek N, Munk PL, O'Connell JX, Lee MJ, Masri BA. Skeletal Radiol 1999;28(9):532-5. Fig. 1A–C MRI of the left knee. A Coronal inversion recovery (TR 2000 / TE 18 / TI 150) image shows a large ovoid mass within the popliteal fossa, which is predominantly of high signal intensity. There is no edema in the adjacent muscles. B Sagittal gradient echo (TR 500/TE 16/flip angle 30°) image shows multiple low-signal foci within the mass consistent with calcifications. Note also the mass merging with the massively dilated popliteal vein behind the distal femur (arrows). The uniform high signal within the dilated vein is typical of slow venous flow. C Axial T2-weighted (TR 2000/TE 80) image shows intimate relationship of the mass to the popliteal artery and vein (arrow), interposed between the mass and the tibial plateau, although no direct communication could be identified Fig. 2A, B Digital subtraction angiogram of the left leg. A Arterial phase oblique image of the popliteal artery demonstrates a direct communication between the lumen of the artery and the mass (arrow), consistent with a pseudoaneurysm. B Late venous phase image shows large slow-flow venous channels (arrowheads) within the mass, draining into the enlarged popliteal vein (arrows) 51 yo M with R Shoulder pain s/p humeral head replacement 10-28-03 4-25-04 HHR Converted to TSA 51 yo M with R Shoulder pain s/p humeral head replacement 5-12-04 Glenoid component well located 6-23-04 Glenoid component dislocated 51 yo M with R Shoulder pain s/p humeral head replacement 6-2-05 Total Shoulder Arthroplasty: Glenoid Component - indications are controversial; - this needs to be performed prior to insertion of the humeral component; - increased glenoid loosening rates from eccentric loading & excessive glenoid wear can be expected with w/ rotator cuff arthropathy Glenoid loosening: - radiolucencies around the glenoid component will eventually be seen in 60% of patients; - some authors note that in many cases radiographs may fail to show loosening because the radiographic beam is not perpendicular to the bone-component interface; From: http://www.wheelessonline.com/ortho/total_shoulder_arthroplasty_glenoid_component Conversion of painful hemiarthroplasty to total shoulder arthroplasty: Long-term results Raymond M. Carroll, MD, Rolando Izquierdo, MD, Michael Vazquez, MD, Theodore A. Blaine, MD, William N. Levine, MD, and Louis U. Bigliani, MD, New York, NY “revision of a failed HHR to a TSA is a salvage procedure whose results are inferior to those of primary TSA…” From: J Shoulder Elbow Surg Nov/Dec 2004 27yo man with palpable nodules in foot 27yo man with palpable nodules in foot 27yo man with palpable nodules in foot 27yo man with palpable nodules in foot 27yo man with palpable nodules in foot