Hormones
advertisement

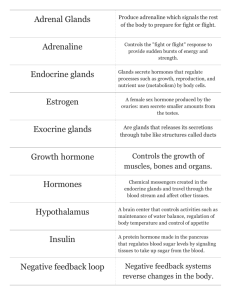
Biological Bases of Behaviour. Lecture 6: Hormones. Learning Outcomes. • By the end of this lecture you should be able to: • 1. Describe the different types of hormones and their key actions. • 2. Explain the neural control of hormone release. • 3. Describe specific hormonal disorders. • 4. Explain the term 'pheromone' and provide examples of pheromones in action. What Are Hormones? • Hormones are chemicals secreted by endocrine glands How Do Hormones Work? • Hormones travel through the blood and influence the activity of other glands and organs. • They produce short- and long-term changes in various cells and organs by acting like neurotransmitters at metabotropic receptors. • A hormone can only influence cells that have specific target receptors for that particular hormone. Types of Hormones. • Endocrine glands produce 2 major classes of hormones (and several other types as well): • 1. Protein hormones: These comprise amino acids, those that are only several amino acids in length are called peptide hormones, whereas larger ones are called polypeptide hormones. They include: • Insulin: Made in the pancreas, it increases the entry of glucose into the cells, and regulates fat storage. • Glucagons: Made in the pancreas, are responsible for increasing the conversion of stored fats to blood glucose. • Leptin: Produced by the fat cells, it informs the brain how much fat is contained in the body. Leptin in Action. When leptin levels are high appetite is decreased. When leptin levels are low appetite is increased and bodily activity is reduced. Mice who inherit 2 copies of the defective ob gene are unable to produce leptin and so overeat. Injections of leptin reduce their food intake. 2. Steroid Hormones. • These are derived from cholesterol from the diet and exert their effects in two ways: • i) They bind directly to membrane receptors. • ii) As they are fat soluble they pass through cell membranes where they attach to receptors in the cytoplasm. Here they determine gene expression. • There are several types of steroid hormones: • a) Corticoids. • Glucocorticoids (principally cortisol) are released by the adrenal glands in response to stress. • They increase the breakdown of fats and proteins into glucose to trigger escape or defense ("fight or flight"). • Mineralocorticoids (e.g. aldosterone) are also produced by the adrenal glands and reduce salt secretion in the kidneys. b) Sex Steroids. • These are released mainly by the ovaries and testes but also by the adrenal glands. They comprise: • Androgens: Testosterone is produced in large amounts in males and has masculinising and defeminising effects; maintaining male secondary sexual characteristics and promoting courtship, aggressive and sexual behaviours. • Estrogens: Estradiol is produced in large amounts in females and has feminising effects, promoting female secondary sexual characteristics, water retention, calcium metabolism, sexual behaviour and maternal behaviours. • Progesterone prepares the uterus for the implantation of a fertilised ovum and regulates the stages of pregnancy. Misunderstandings. • According to Nelson (2000), there misunderstandings surrounding hormones: are several • 1. Sex steroids are sex-specific: In fact both males and females produce androgens and estrogens though their relative concentrations differ. • 2. Individual differences in behaviour and physiology reflect differences in hormone concentration: While overall concentration is indeed important, of equal importance is the receptivity of the cells to the hormone. • A high hormone concentration will have little effect if cells lack receptivity, an excellent example of this is Androgen Insensitivity Syndrome. Control of Hormone Release. • Hormone release is controlled by two key structures in the brain: • 1. Hypothalamus: This is located at the base of the brain and consists of several interconnected nuclei. • The hypothalamic nuclei synthesise releasing hormones that either stimulate or inhibit the release of hormones from the pituitary gland. • The hypothalamus also secretes oxytocin and vasopressin which travel to the posterior pituitary gland. This then releases them into the bloodstream in response to certain neural signals. Negative Feedback in the Hypothalamus. • The hypothalamus maintains fairly constant levels of hormones because it operates a negative feedback system. E.g: excitatory Hypothalamus Thyroid Stimulating HormoneReleasing Hormone inhibitory Anterior pituitary Thyroid Stimulating Hormone Thyroid gland Thyroid hormones 2. Pituitary Gland. • This is called ‘the master gland’ as it produces at least 10 hormones which influence the other endocrine glands via the hypothalamus. • It consists of two separate regions. • The anterior pituitary and the posterior pituitary each share distinct connections with the hypothalamus. hypothalamus Blood supply Anterior pituitary GH, ACTH, TSH, FSH, LH and prolactin Posterior pituitary Vasopressin and oxytocin Anterior Pituitary Gland. • Hormones produced here are referred to as tropic as they stimulate various processes: • Luteinizing Hormone (LH): Increases production of progesterone and stimulates ovulation in females. In males it increases production of testosterone. • Follicle-Stimulating Hormone (FSH): Increases production of estrogen and maturation of the ovum (in females) and sperm (in males). • Thyroid-Stimulating Hormone (TSH): Controls secretions of the thyroid gland. • Growth Hormone (GH): Increases body growth. • Prolactin: Controls milk production in females. • Adrenocorticotropic Hormone (ACTH): Controls secretions of the adrenal gland. Posterior Pituitary Gland. This stores oxytocin which controls uterine contractions, milk release, parental behaviours and orgasm. It also stores vasopressin (also known as antidiuretic hormone) which constricts blood vessels, raises blood pressure, and decreases urine volume. Hormones and Behaviour. • Hormones do not cause a particular behaviour to change, rather they change the likelihood that a particular behaviour will occur in an appropriate environmental context. • Certain behaviours can also influence hormone levels, e.g. testosterone levels can rise or fall depending upon whether a contest has been won or lost. • This is a ‘chicken and egg’ problem, i.e. do hormones influence behaviour by directly affecting the brain, or does behaving in a particular manner influence hormone production? • In order to decide we can use three techniques: Experiments to Test Hormone/Behaviour Relationships. • 1. If we remove the source of a particular hormone then a behaviour that is assumed to depend upon that hormone should disappear. E.g removal of testosterone by castration dramatically reduces sexual desire and aggression in many male animals. • 2. Once a behaviour has ceased following hormone removal, we can restore hormone function and see if the behaviour returns. E.g administration of testosterone to castrated adult males restores aggressive behaviours and the mating urge. • 3. If hormones and certain behaviours are related, then we should expect that alterations in the relative concentration of a hormone should produce related alterations in a behaviour. E.g aggression should be higher when circulating levels of testosterone are higher. Human Hormone Disorders. • 1. Congenital Adrenal Hyperplasia (CAH). • This is a genetic disorder producing enzyme deficiency in the adrenal glands. • The glands are unable to produce sufficient quantities of cortisol which normally inhibits the release of adrenocorticotropic hormone (ACTH) which promotes sexsteroid synthesis. • ACTH is thus produced in large amounts and the foetus is exposed to excessive amounts of androgens which have a masculinising effect. • Affected females display masculinised genitals and behaviour. Affected males may show precocious puberty. 2. Androgen-Insensitivity Syndrome (AIS). • An X-linked recessive disorder (affecting only males) in which androgen receptors in the cells do not function. • The male brain and body remain unresponsive to androgens and are feminised due to maternal estrogens. • At puberty the testes do not descend and secondary female sexual characteristics appear due to circulating estrogens. • Individuals are often reared as girls and do not discover that they are ‘male’ until they fail to menstruate at puberty. 3. Idiopathic Hypogonadotropic Hypogonadism (IHH): • This is caused by the insufficient release of gonadotropin releasing hormone from the hypothalamus. • It is sometimes referred to as ‘Kallman’s Syndrome’. • Affected males are genetically normal, but do not receive sufficient testosterone before birth. • Their genitals remain relatively unaffected due to the influence of maternal androgens, but at puberty secondary male sex characteristics fail to appear. 4. Turner’s Syndrome. • This syndrome was first described by Turner (1938). • It only affects females in which all or part of one X chromosome is deleted. • This leads to a failure in ovary development, and produces short stature and physical anomalies such as webbing of the neck. • Externally, such individuals appear female but as they fail to produce female sex hormones they remain sexually immature unless provided with hormone replacements. • They remain infertile. 4. 5- Reductase Deficiency. • This is a deficiency of the enzyme 5-reductase which normally converts testosterone into dihydrotestosterone. • As dihydrotestosterone is principally responsible for masculinising the external genitals before birth, males with this syndrome are born with ambiguous genitalia and undescended testes. • They are often mistaken for females at birth and reared as such. • However at puberty when exposed to large amounts of testosterone their body and external genitals become more masculine. Pheromones. • These are chemicals derived from sex hormones which are manufactured and released by the apocrine glands. • They are released into the environment via sweat and urine where they are detected by individuals of the same species in whom they activate specific physiological and behavioural responses. • The following effects have been noted in animals: Pheromone Effects in Animals. Lee-Boot effect: When groups of female mice are housed together their estrus cycles slow down and stop. Whitten effect: If groups of female mice are then exposed to an adult male mouse (or to the odour of his urine) they begin estrus again and their cycles become synchronised. Similar menstrual synchrony has been reported in human females sharing accommodation. Vandenburg effect: The presence of an unrelated adult male causes the acceleration of puberty in female rats. This has also been reported for human females in the presence of a stepfather. Bruce effect: When a pregnant female mouse is housed with a male mouse who is not the father the pregnancy is likely to fail and she quickly comes into estrus again. Effects of Human Pheromones. • At puberty, pheromones derived from androgens act as sexual attractants. E.g. Thorne et al., (2002) found that nonpill using females unknowingly exposed to male pheromones gave higher attractiveness ratings to photographs of males faces.