NREPP
advertisement

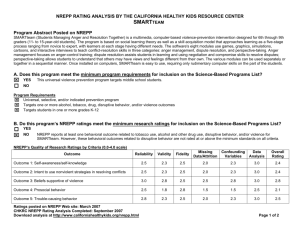
Identifying and Implementing Evidence-Based Mental Health and Substance Abuse Services September 16, 2005 Kevin D. Hennessy, Ph.D. Science to Service Coordinator Substance Abuse & Mental Health Services Administration U.S. Department of Health & Human Services “A Life in the Community For Everyone” “Building Resilience & Facilitating Recovery” A Cross-Cutting Principle: Science to Services/Evidence-Based Practices How do we translate research into practice? How do we connect services to science? An old and well-defined problem Few research innovations are implemented successfully in typical health care settings Many widely used interventions have little if any research support Most in treatment don’t receive evidence-based interventions Many reports exist documenting the problem and recommending actions Bridging the Gap Between Research and Practice: Forging Partnerships with Community-Based Drug and Alcohol Treatment (Institute of Medicine Report) – 1998 Mental Health: A Report of the Surgeon General – 2000 Achieving the Promise: Transforming Mental Health Care in America (The President’s New Freedom Mental Health Commission) – 2003 Knowledge to practice gap remains at 15-20 years Original research 18% Negative results variable Dickersin, 1987 Submission 46% Koren, 1989 Negative results 0.5 year Kumar, 1992 0.6 year Kumar, 1992 Acceptance Publication 35% Lack of numbers Balas, 1995 0.3 year Poyer, 1982 Expert opinion Bibliographic databases 50% Poynard, 1985 Inconsistent indexing 17:14 6. 0 - 13.0 years Antman, 1992 Reviews, guidelines, textbook 9.3 years Implementation It takes 17 years to turn 14 per cent of original research to the benefit of patient care SAMHSA Activities for Reducing the Knowledge – Practice Gap Identify evidence-based practices (NREPP) Develop guides, manuals and other materials Evidence-Based Practice Implementation Resource Kits Disseminate materials and provide trainings through regional centers Centers for the Application of Prevention Technology (CAPTs) Addiction Technology Transfer Centers (ATTCs) Center for Mental Health Services Technical Assistance Centers Create interagency and private-public partnerships National Registry of Evidence-based Programs and Practices (NREPP) Purpose: A voluntary rating and classification system for mental health and substance abuse prevention and treatment interventions. Goal: NREPP will become a leading national resource for science-based information on substance abuse and mental health prevention and treatment interventions. NREPP Timeline 1998…Started with a focus on substance abuse prevention as the National Registry of Effective Prevention Programs 1998-2003…reviewed and rated over 1,100 substance abuse prevention programs information on over 150 Model, Effective, and Promising Programs on web site (www.modelprograms.samhsa.gov) 2004…initial expansion of system to include substance abuse treatment, mental health promotion, and mental health treatment programs NREPP Current Status Formal public comment process by SAMHSA this summer Notice in August 26th Federal Register Available through SAMHSA web site – access through “Quick Picks” on SAMHSA’s home page (www.samhsa.gov) Written comments due no later than October 25th U.S. Mail – SAMHSA, c/o NREPP Notice, 1 Choke Cherry Road, Rockville, MD 20877 Electronic Mail – nreppcomments@samhsa.hhs.gov Posting of recently completed reviews (using older NREPP system) by Fall 2005 No new reviews until 2006 New NREPP Website will be launched in 2006: www.nationalregistry.samhsa.gov NREPP: Comprehensive & Transparent Comprehensive Scientists independently evaluate and classify outcomes for programs/practices based on statistical significance, replications and 16 evidence quality criteria Program impact and practical significance will be reported through effect sizes For status programs, additional information on implementation, training, quality tools, staffing, costs, etc. will be provided NREPP: Comprehensive and Transparent Transparent Review results will be posted on the new NREPP website By 2006 Web site will feature: Outcomes searchable database Links to educational materials on review criteria Self-assessment tool for candidate programs Links to technical assistance centers and supports NREPP: Draft Rating Criteria Two Types of Criteria Evidence Rating Criteria “Utility Descriptors” NREPP: Evidence Rating Criteria 16 evidence rating criteria applied to each program outcome (0 to 4 scale). Include: Theory-driven selection of measures & analytic methods Reliability Validity Intervention and comparison fidelity Assurances to participants Standardized Data Collection Selection bias Attrition and missing data Analysis meets data assumptions NREPP: “Utility Descriptors” Look beyond scientific evidence and ensure that programs are able to be implemented. Assessments also made of the following: Implementation Quality Monitoring Unintended or Adverse Events Population Coverage Cultural Relevance Staffing Cost NREPP: Questions to the Public From the August 26th Federal Register Notice (FRN) Is proposed system objective, transparent, efficient, and scientifically defensible? How might SAMHSA engage stakeholders in determining priority review areas? How best to use statistical significance and measures of effect size in NREPP? Beneficial to use multiple categories of effectiveness? Approach to assessing and presenting cultural relevance? NREPP: Questions to the Public From the August 26th Federal Register Notice (FRN) - continued Approach to re-reviewing existing NREPP programs? Types of technical assistance needed to promote adoption of NREPP interventions? How best to involve consumers, families, and other non-scientists in NREPP? What, if any, guidance on use of NREPP interventions within block grants? How best to promote other sources – e.g., clinical judgement, consumer values, etc – in decisions regarding selection, delivery and financing of services? Panel to annually review NREPP operational and technical suggestions? NREPP’s Reach Influences SAMHSA discretionary and block grant investments Serves as a resource for states and communities seeking to implement evidence-based Mental Health & Substance Abuse prevention and treatment services Provides an important tool for both public and private purchasers in selection of effective services Publications and Materials on Best Practices in Mental Health and Substance Abuse Prevention & Treatment What type of Products? • • • • • • Training Manuals Evidence-based Implementation Resource Kits (CMHS) Interactive Web-based Technical Support (Prevention Platform) Treatment Improvement Protocols (TIPs) Quick Reference Cards & Pocket-size Guides Fact Sheets, Brochures, Reports, and Periodicals Publications and Materials on Best Practices in Mental Health and Substance Abuse Prevention & Treatment Who Uses the Products? Program Administrators & Staff Clinicians Policymakers Consumers Where to Find the Products: For SA Treatment go to www.kap.samhsa.gov For SA Prevention go to www.prevention.samhsa.gov For Mental Health go to www.mentalhealth.samhsa.gov Evidence-Based Practice Implementation Resource Kits Focus on six practices Assertive community treatment Family psychoeducation Supported employment Integrated dual disorders treatment Illness management and recovery skills Standardized pharmacological treatment Two Phases I – Development (Fall 2000 – Summer 2002) II – Pilot-Testing (Summer 2002 – Summer 2005) More information is available through SAMHSA’s web site (www.samhsa.gov) under “Mental Health System Transformation” Evidence-Based Practice Implementation Resource Kits Kits have targeted and distinct components for: Consumers Family and Other Supports Practitioners and Clinical Supervisors Mental Health Program Leaders Public Mental Health Authorities/Administrators Kits include: Research summaries Information sheets for all stakeholders Tip sheets for program leaders and administrators Program manuals/workbooks for practitioners Introductory and training/demonstration videos Fidelity assessment tools and cultural competence statements Outcome measures Materials, Trainings & Technical Assistance for Prevention Centers for the Application of Prevention Technology www.captus.org Purpose: Assist States and Communities in the application of evidence-based substance abuse prevention programs, practices, and policies Goal: To increase the impact of prevention Materials, Trainings & Technical Assistance for Treatment SAMHSA’s Addiction Technology Transfer Centers www.nattc.org Purpose: To transmit the latest knowledge, skills and attitudes of professional addiction treatment practice Goal: To enhance clinical practice Center for Mental Health Services Research, Training and TA Centers Currently 55 Centers provide a range of services – many are free but charges may apply for some: Technical assistance Information and referrals On-site consultation Training Library services Publications Other resources More information is available through SAMHSA’s web site: www.mentalhealth.samhsa.gov/links/ Promoting Interagency Partnerships Collaborations with National Institutes of Health to jointly fund state planning grants facilitating implementation of evidence-based practices – RFA-MH-03-007 – State Implementation of EvidenceBased Practices: Bridging Science and Service (with NIMH) – RFA-MH-05-004 – State Implementation of EvidenceBased Practices II: Bridging Science and Service (with NIMH) – RFA-DA-05-002 – Enhancing State Capacity to Foster Adoption of Science-Based Practices (with NIDA) Creating Public – Private Partnerships Partnership between: SAMHSA’s Center for Substance Abuse Treatment (CSAT) Robert Wood Johnson Foundation (RWJF) Goals of improving organizational processes to facilitate client access and retention in addictions treatment. Initial successes include: Reduced Waiting Times by 31% (n=24) Reduced No-Shows by 22% (n=13) Increased Admissions by 25% (n=19) Increased Treatment Continuation Rates by 33% (n=8) More info available through web site – www.niatx.org Advancing Science to Service Efforts and Reducing the Knowledge – Practice Gap Focus on elements of health care redesign detailed in Crossing the Quality Chasm (Institute of Medicine, 2001) – Apply evidence to health care delivery – Align payment policies with quality improvement – Prepare the workforce – Use information technology In Conclusion “The future is here. It’s just not widely distributed yet.”