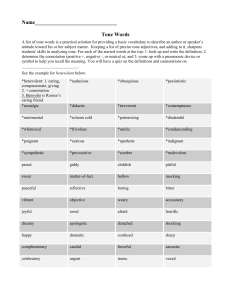
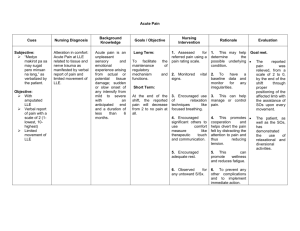
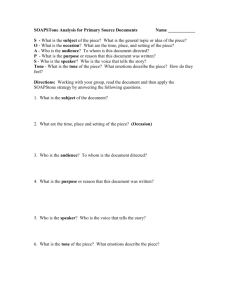
High Tone Power Therapy
advertisement

H. U. MAY High Tone Power Therapy - HiToP® Theory and Practice Porto, March 2005 Introduction Theory, part 1 "High Tone Therapy" and "High Tone Power therapy" Simultaneous modulation of frequency and amplitude and its advantages "High Tone Power Therapy" and the equipment to realise this most advanced an most modern kind of "High Tone Therapy", HiToP®, is the result of the last step of developments of middle frequency therapy. I will begin with the explanation of the reasons for the decision for the development of a new sophisticated method within the physical therapy, described as “electrical high tone frequency alternating field therapy”, abbreviated in German “Hochtontherapie”, in English “high tone therapy”, in Polish “terapia energotonowa”, that means “energy tone therapy”. The new method has been realised in Germany by gbo. The result is the equipment HiToP® (High Tone Power Therapy). High tone therapy is a purposeful new development in the field of electrotherapy. It appears with the pretension to realise all effects known and expected from the traditional low and middle frequency therapy with higher efficacy. Including ranges of frequencies never used until now and introducing the simultaneous modulation of frequency and amplitude a completely novel method of electrotherapy has been created. Important aspects of this innovative creation were to optimise the therapeutically width and to take more into account the very interesting non-stimulatory effects. Several clinical investigations published recently (2002, 2003 and 2004) in Poland confirm the expectations concerning the efficiency of high tone therapy in various injuries and/or diseases. To understand correctly and completely the position of the high tone therapy within the electrotherapy it is required to be well acquainted with some terms of the fields of physiology, related disciplines and physical therapy. However, neither all medical doctors nor all physical therapists have been sufficiently educated during their specific education's in both disciplines, or may be they have forgotten some details. Therefore I will try to repeat, to explain and to comment some of the most important terms and facts. Terms: The term “High tone therapy” This term, abbreviated from “electrical high tone frequency alternating field therapy” was proposed by medical doctors just after the introduction of the first generation of high tone therapy units High tone therapy High tone therapy is a purposeful new development in the field of electrotherapy, basing on the principles of the electric differential therapy (HANSJÜRGENS & MAY, 1990). By means of simultaneous modulation of frequency and amplitude (SimulFAM®), either a) along the threshold graph after it’s individual determination (SimulFAMi) or b) with crossing of this threshold graph with adjustable crossing angles (SimulFAMx) it is possible to generate alternatively either a) selectively non-stimulatory effects or b) non-stimulatory effects in combination with stimulatory effects. Electric differential therapy Electric differential therapy (MAY & HANSJÜRGENS, 1988; HANSJÜRGENS & MAY, 1990) can be considered as a principle to classify currents used in electrotherapy and as a principle to select the most suitable kind of current for the pathological condition or symptom just to be treated. For the selection of the best suitable current is decisive – like in pharmacology – the best relation between efficacy and tolerability, in other words: the therapeutic width. Tolerance We have to distinguish between local and systemic tolerance for currents. Local tolerance The local tolerance is correlated with or described by respectively a) the value of the (“direct”) pain threshold, b) the risk of chemical burning, c) the risk of burning by heat, d) the value of the (“indirect”) pain threshold caused by intensive muscle contraction, measured as functions of frequency and intensity, for b and c additionally as functions of time. Systemic tolerance The systemic tolerance can be defined mainly by means of the a) the value of the threshold for ventricular fibrillation or b) the value of the threshold for cardiac arrest. In cases of current applications including head and brain thresholds for undesired sensations and/or generalised epileptic seizures are important. In cases of treatments of the trunk with high current intensities above the motor threshold the thresholds of the muscles responsible for respiration are important. Effects The electric differential therapy distinguishes between stimulatory and non-stimulatory effects. Stimulatory effects Stimulatory effects are caused by generation of action potentials in excitable structures (nerves, muscles, receptors). The frequency of the triggered action potentials ranges between > 0 and – for very short periods – 1000 Hz, defined in physiology and physical medicine as the “low frequency range. The application of stimulatory effects can be realised either according the functional imitation principle or according the functional fatiguing principle, depending on the values of the frequencies of stimulation in relation to the fatiguing frequency of the just stimulated excitable structure. Important frequencies for therapeutically desired special effects, basing on well known physiological investigations regarding the discharge behaviour of excitable structures - usable as border line frequencies between the functional imitation principle and the functional fatiguing principle Efferent nerve fibres Sympathetic nerve fibres Lipolysis 3 Hz This frequency of 3 Hz is not a border line frequency between imitation and fatiguing frequencies. The lipolytic effect of a stimulation of sympathetic nerve fibres innervating fatty tissue is decreased in case of using higher frequencies than 3 Hz because of the simultaneously increasing vasoconstriction (ROSELL, 1966). Vasoconstriction 10 Hz Motor nerve fibres 20 Hz Afferent nerve fibres 100 Hz, however, not valid for all groups of afferent fibres Instructions regarding the meaning of the principles of functional imitation and functional fatiguing related to the stimulation of the mentioned groups of nerve fibres The principle of imitation can be used therapeutically for all of the mentioned groups, the principle of fatiguing mainly for sympathetic fibres, in few cases for motor nerves as well. To avoid undesired fatiguing effects during the initial phase of a treatment in cases of applications of various (low) modulation frequencies, please start every time with the lowest frequency! Stimulation of sympathetic nerve fibres: Frequencies up to 3 Hz: Frequencies up to 10 Hz: Frequencies for example > 10 Hz, 100 Hz: activation of the lipolysis within the innervated area mainly vasoconstriction increasing with frequency reduced lipolysis caused by vasoconstriction and product-inhibition vasodilatation after initial vasoconstriction Stimulation of motor nerve fibres: Frequencies up to 20 Hz: Muscle exercise, re-education, strengthening with individually designed and adjusted periods consisting in phases of stimulation interrupted by pauses. 20 Hz is the physiological tetanising frequency, i. e. the maximum discharge frequency in the efferent neurones of the motor units during voluntarily initiated maximum isometric contraction (HENNEMAN 1957; HENNEMAN et al. 1965; SOMJEN et al 1965; MILNER-BROWN et al. 1973; FREUND, BÜDINGEN & DIETZ 1975; BÜDINGEN & FREUND 1976) Frequencies > 20 Hz: muscle relaxation caused by fatiguing stimulation Stimulation of afferent (somato-sensory) nerve fibres: This group of nerve fibres is not homogeneous. Therefore a frequency limit valid for all fibres does not exist. Furthermore, there is no indication for purposeful fatiguing stimulation of this group of fibres. Nevertheless, 100 Hz can be accepted as the most useful frequency to cause central pain relief according the imitation principle by means of counter-irritation. Non-stimulatory effects These effects are defined as effects caused independently from the generation of action potentials. Non-stimulatory effects at the physical and chemical levels of efficacy Such effects are for instance movements of freely movable charged particles, ions as carriers of the electrical currents, of water molecules (dipoles) and of charges fixed in molecules as constituents of the tissue. Results of these primary effects are facilitation and acceleration of diffusion, that means equilibration of concentration differences, and the enhancement of the ability of water to act as an solvent. End of Introduction, Theory , Part 1 Practice, part 1 Practice, part 1, High Tone Power Therapy - HiToP® A. The 2 modes of application of the HiToP therapy 1. Whole body treatment 2. Regional (topical) treatments, mostly (a-e) with SimulFAMi, only for stimulation of nerves and muscles with SimulFAMX (f-g) a. Shoulders b. Vertebral column and abdominal region c. Hip d. Knee e. Ankle f. Peripheral stimulation of sympathetic fibres causing vasoconstriction (upper arm) g. Stimulation of muscles (M. quadriceps femoris, M. triceps brachii, calf-muscles, abdominal muscles) The recommended whole body treatment carried out besides the topic application has not only general effects upon the mood and the general condition of the patient; moreover, the superposition of the alternating electric fields of the general treatment and the topical treatment causes periodical changes of the directions of the vectors of the local electric fields responsible for the electrochemical shaking effect. This kind of interference is used for the support of non-stimulatory effects and not for the generation of stimulatory effects, realised in traditional interferential current units, invented by NEMEC. HiToP® allows the use of more than two electrodes per channel. The purpose is to compensate the different sensitivities of different body regions or to concentrate the effects in particular areas respectively. Moreover, it is possible to treat two different body regions in the same time using only one channel B. The 2 modes of SimulFAM 1. SimulFAMi - without stimulation of nerves and/or muscles (ca. 80 % of the applications in practice) 2. SimulFAMX - for stimulation of nerves and/or muscles (ca. 20 % of the applications in practice) Only apparently complicated at the latest convincing experiencing the feeling: The variability of the "slope" of SimulFAMX and the advantage of "paradoxical stimulation" SimulFAMX and its stimulatory frequencies The choice of the most suitable frequency 0.3 Hz for activation of the muscle pump (for instance for the prevention of venous thrombosis and for the treatment of edema) 3 Hz 10 Hz for lipolysis for vasoconstriction (for example after in juries and for the reduction of edema) 20 Hz 100 Hz for tetanising stimulation of muscles for central pain relief by means of counterirritation - only one of the 5 pain relieving effects available in HiToP® The modulation of frequency happens between two corner frequencies, 212 Hz and 215 Hz. The duration of one period of the “slow” threshold-adapted modulation of frequency and amplitude, SimulFAMi, is 144 s (2 min 24 s). Frequency and amplitude will be changed all the time stepwise periodically in the same direction, either both upstairs or both downstairs. The frequency of the “fast” simultaneous modulation of frequency and amplitude (SimulFAMx) can be varied between 0,1 Hz and 200 Hz. In this case frequency and amplitude can be changed periodically quickly either in the opposite direction or in the same direction (upstairs or downstairs). Opposite changes lead to more or less brusque stimulation, corresponding changes lead to softer stimulation (paradoxical stimulation). End of practice, part 1 Pictures illustrating the theoretical background of high tone power therapy presented after the first part of practice when the participants of the seminar have acquired the first practical experience with HiToP® Threshold current mA (eff) Threshold graph of the current sensation Threshold curve Frequency in Hz Intensity Intensität Threshold Curve lle e hw c S Horizontal stimulation. Vertical stimulation. Threshold threshould Sensation curve as a function beim Menschen of frequency in Abhängigkeit der frequency Frequency Frequenz Intensität Threshold Curve ® SimulFAM i lle e hw c S SimulFAM i fmin fmax Frequenz Intensität Threshold Curve ® SimulFAM i lle e hw c S SimulFAM i fmin fmax Frequenz Intensität Threshold Curve ® SimulFAM i lle e hw c S SimulFAM i fmin fmax Frequenz Intensität Threshold Curve ® SimulFAM i lle e hw c S SimulFAM i fmin fmax Frequenz Intensität Threshold Curve ® SimulFAM i lle e hw c S SimulFAM i fmin fmax Frequenz Intensität Threshold Curve ® SimulFAM i lle e hw c S SimulFAM i fmin fmax Frequenz Intensität Threshold Curve ® SimulFAM i lle e hw c S SimulFAM i fmin fmax Frequenz Intensität Threshold Curve ® SimulFAM i lle e hw c S SimulFAM i fmin fmax Frequenz Intensität Threshold Curve ® SimulFAM i lle e hw c S SimulFAM i fmin fmax Frequenz Intensität Threshold Curve ® SimulFAM i lle e hw c S SimulFAM i fmin fmax Frequenz Intensität Threshold Curve ® SimulFAM i lle e hw c S SimulFAM i fmin fmax Frequenz Threshold Curve ® SimulFAM i Intensity SimulFAM i fmin fmax Frequency Threshold Curve ® SimulFAM i Intensity 3 octaves in 72 steps of 1/4 tones SimulFAM i 1 second each fmin fmax Frequency X Intensität ® SimulFAM SimulFAM X fmin fmax Frequency X Intensität ® SimulFAM lle e hw c S SimulFAM X fmin fmax Frequenz X Intensität ® SimulFAM lle e hw c S SimulFAM X fmin fmax Frequenz X Intensität ® SimulFAM lle e hw c S SimulFAM X fmin fmax Frequenz X Intensität ® SimulFAM lle e hw c S SimulFAM X fmin fmax Frequenz X Intensität ® SimulFAM lle e hw c S SimulFAM X fmin fmax Frequenz X Intensität ® SimulFAM lle e hw c S SimulFAM X fmin fmax Frequenz X Intensität ® SimulFAM lle e hw c S SimulFAM X fmin fmax Frequenz X Intensität ® SimulFAM lle e hw c S SimulFAM X fmin fmax Frequenz X Intensität ® SimulFAM lle e hw c S SimulFAM X fmin fmax Frequenz X Intensität ® SimulFAM lle e hw c S SimulFAM X fmin fmax Frequenz X Intensität ® SimulFAM lle e hw c S SimulFAM X fmin fmax Frequenz X Intensität ® SimulFAM lle e hw c S SimulFAM X fmin fmax Frequenz X Intensität ® SimulFAM lle e hw c S SimulFAM X fmin fmax Frequenz X Intensität ® SimulFAM lle e hw c S SimulFAM X fmin fmax Frequenz lle e hw c S Intensität Advantages of ® SimulFAM fmin fmax X Frequenz lle e hw c S Intensität Advantages of ® SimulFAM fmin fmax X Frequenz lle e hw c S Intensität Advantages of ® SimulFAM fmin fmax X Frequenz lle e hw c S Intensität Advantages of ® SimulFAM X Balanced relation between the phases above threshold and below threshold fmin fmax Frequenz lle e hw c S Intensität Advantages of ® SimulFAM X Sensitive patient fmin fmax Frequenz lle e hw c S Intensität Advantages of ® SimulFAM fmin fmax X Frequenz lle e hw c S Intensität Advantages of ® SimulFAM X Now Ifmax can be adjusted via the modification knob as x% of Ifmin. Ifmax fmin fmax Frequenz lle e hw c S Intensität Advantages of ® SimulFAM X Now Ifmax can be adjusted via the modification knob as x% of Ifmin. fmin fmax Frequenz Intensität “Paradoxical” Stimulation via ® lle e SimulFAM X Schw Now Ifmax can be adjusted via the modification knob as x% of Ifmin. fmin fmax Frequenz Intensität “Paradoxical” Stimulation via ® lle e SimulFAM X Schw Now Ifmax can be adjusted via the modification knob as x% of Ifmin until the patient has the maximum comfort fmin fmax Frequenz End of the presentation of pictures Theory, part 2 Theory, part 2 History of High Tone Power Therapy - HiToP® The purpose of this new development The effects in the tissue The effects in the healthy body The use of HiToP® in medicine Year of publication or introduction or start of the development respectively, inventors and terms of the introduced currents and methods 1935 KOEPPEN: (Hoch-)"Tonfrequenzströme", (high) tone frequency currents 1944 GILDEMEISTER: "Mittelfrequenzströme", middle frequency currents 1948 NEMEC: Interferenzströme, interferential currents, using amplitude modulation (AM) caused by interference of two unmodulated middle frequency currents between 4000 and 4100 Hz 1988 MAY & HANSJÜRGENS: Electric differential therapy 1995 HANSJÜRGENS & MAY: 1st generation of high tone therapy equipment, using frequency modulation (FM) for "horizontal stimulation" within 1 1/2 octaves up to 12300 Hz 2000 MAY: 2nd generation of high tone therapy equipment: High Tone Power Therapy, HiToP®, using simultaneous modulation of frequency and amplitude, SimulFAM®, within 3 octaves between 4096 Hz and 32768 Hz, realised by gbo in Rimbach, Germany The term "Tonfrequenzströme", "tone frequency currents", was created by KOEPPEN 1935 in his scientific publication "Tonfrequenzströme in der Medizin", "Tone frequency currents in medicine", and he still described important advantages and special interesting effects appearing and rising with increasing frequencies into the high tone frequency range. Therefore, it is legitimate and more precise to use the term "High tone frequency currents" instead of "tone frequency currents", because of the absence of the special advantages within the lower tone frequency range. KOEPPENS investigations concerning the high tone frequency currents did not lead to any creations of equipment for electrotherapy. GILDEMEISTER and his pupil SCHWARZ were physiologists. GILDEMEISTER created the term "middle frequency currents" in his last paper, published 1944 after his death 1943. SCHWARZ published many papers concerning the physiological properties of the middle frequency currents within the 40th and 50th of the 20th century. Without the knowledge of the publications of KOEPPEN, GILDEMEISTER & SCHWARZ interferential current as the first therapeutic application of middle frequency currents was introduced by NEMEC after the second world war. The next step was the differentiation of the therapeutic application of middle frequency currents by the creation of the method of "Electric Differential Therapy" (MAY & HANSJÜRGENS) to distinguish between stimulatory and non-stimulatory effects related to "low frequency effects" and "middle frequency effects": Unmodulated middle frequency currents can be used for nonstimulatory effects, and middle frequency currents modulated in there amplitude within the low frequency range can be used for stimulation of nerves and muscles; however, they contain additional non-stimulatory effects. In the first generation of high tone frequency treatment units, developed by MAY, HANSJÜRGENS & FORSTER within the middle of the last decade of the last century, the next (3rd) important step into the direction of increase of efficacy and significant reduction or even complete elimination of discomfort was realised by the introduction of frequency modulation (FM) - instead of amplitude modulation (AM). "High Tone Therapy" is the abbreviation for "Electrical High Tone Frequency Alternating Field Therapy". As mentioned above, the first important step to reduce the discomfort and the risks of electrotherapy, furthermore to increase the efficacy of electrical currents used for therapeutic purposes was the introduction of middle frequency currents as the so called "interferential current" by the inventor Hans NEMEC in the middle of the last century. KÖCHERT and NEMEC founded the company NEMECTRON, and the first generations of interferential current treatment units, named Nemectrodyn®, were more successful, and the interferential current was more comfortable for the patients than the other currents (Galvanic current and low frequency currents) used in electrotherapy. The aim of the development of the HiToP® High Tone Power Therapy The aim of this development was, to intensify and to combine already known effects of the especially well tolerable currents, the so called middle frequency currents. Moreover, the equipment should indicate not only the current intensity (amperage) in mA as a singular quantitative parameter of the applied electricity: Now additionally will be indicated the voltage in V, the power in mW, the impedance in W and the sum of the applied electrical energy in mWh. Until now no other electrotherapy equipment offers such completeness of indication of important electric parameters. Non-stimulatory effects at the biochemical level of efficacy Increase of the probability of “meetings” and contacts between enzymes and substrates Enzymes are biocatalysts. The mediated biochemical reactions are in all cases electrical events too, facilitated by means of alternating electrical fields. Conformation changes of signal molecules as a reason for the activation of the adenylatcyclase In several papers changes of the intracellular formation of cAMP (cyclic Adenosinemonophosphate, one of the most important second messengers) caused by middle frequency currents have been published (KORENSTEIN 1984; BRIGHTON & TOWNSEND 1986; NOSZVAY-NAGY 1988-1994). Beneficial influences upon the trophism of the tissues, anti-asthmatic, generally activating and antidepressive effects - within the therapeutic level of efficacy – could be explained by this electro-biochemical effect. Non-stimulatory effects at the neurophysiological level of efficacy Intensities of unmodulated middle frequency currents distinctly above the threshold cause in nerves and muscles partial depolarisation, in nerves correlated with a block, in muscles additionally with a physiological contracture. Below of these relatively high intensities a range of intensities exists which is characterised by some particularities: Non-stimulatory effects at the therapeutic level of efficacy 1. Pain relief a. symptomatic, immediate, transient via distribution and thinning of mediators of pain and inflammation via blocking of afferent fibres involved in coding of pain information b. causal, longer lasting by facilitation and/or activation of metabolic processes, acceleration and abbreviation of healing processes c. indirect by anti-oedematous effects via reversible physiological contractures of the smooth muscles of the vessels including lymphatic vessels 2. Acceleration and abbreviation of healing processes, which are not accompanied by pain (s. 1 b) 3. Local anti-oedematous effects (explained under 1 c) and diuretic effects As I partially still mentioned above, the most important fundamental facts for the purposeful development of the high tone therapy equipment are originated from the publications of the physiologists Martin GILDEMEISTER (Straßburg, Leipzig), Friedrich SCHWARZ (Leipzig, Posen, Jena), Oscar A. M. WYSS (Zürich), and of a pioneer of physical medicine, Siegfried KOEPPEN (Halle, Wolfsburg), furthermore from the electrotoxicological investigations of GEDDES and co-workers (1969). KOEPPEN already 1935 introduced the term “Tonfrequenzströme”, English “tone frequency currents”, GILDEMEISTER 1944 the term “Mittelfrequenzströme”, English “middle frequency currents", defined as alternating currents with frequencies between ca. 1000 Hz and 100 kHz . 1. The principle of apolar “stimulation” is valid: Using two electrodes (of the same size) under both electrodes are generated the same effects at the same time. Anodic or cathodic effects do not exist. 2. The law of “Alles oder nichts” (everything or nothing) is not valid. With repetitions of tests of the thresholds the values increase. 3. There are no relations between the single phases of the middle frequency current and the begin of the triggered action potentials. 4. Around the threshold single action potentials are triggered irregularly, but this kind of ongoing activity disappears after a while 5. Intensities above the threshold trigger a “transient excitatory activity”, abbreviated “tea”: immediately after the start of the establishment of the alternating electrical field the firing rate has it’s highest values, followed by decreasing discharge frequencies. “Tea” is correlated at the psychophysical level of efficacy with a fading tingling sensation. “Tea” leads to fatigue of the involved excitable structures. Monographs of WYSS (1975) and of his pupil SENN (1980) contain comprehensive descriptions of the history and the peculiarities of the middle frequency currents. However, the descriptions of the pain relieving effects of unmodulated and modulated middle frequency currents are incomplete. The possibilities to use either the blocking or pseudoblocking effects of unmodulated middle frequency currents or the counter-irritation principle (GAMMON & STARR 1941), caused by the low frequency effects of modulated middle frequency currents have not been mentioned. On the other hand, just the pain relieving effect by means of unmodulated middle frequency currents can be easily explained by the results of neurophysiological investigations of WYSS and his pupils, for instance the “reversible reactive partial depolarisation”, with other words the “plateau effect” (KUMAZAWA & WYSS 1966). These results, gained by means of intracellular recordings, could be confirmed later by extracellular recordings (BOWMAN 1981). The cited publications reveal 1.) that the local and systemic tolerability of alternating currents above 50 Hz is increasing with increasing frequencies and accordingly the possibility of incoupling of electric power into the body is increasing too with increasing frequencies – without any local discomfort and without any risks for the heart, 2.) that these currents, named “(high) tone frequency currents” or “middle frequency currents” have particular advantageous qualities in comparison to the traditional low frequency currents and direct current. The frequency-correlated increase of the threshold of afferent fibres of the sensory nervous system is also valid for the motor fibres innervating the striated muscles (DALZIEL, 1941-1973), and we can assume for the sympathetic fibres responsible for the smooth muscles of the vasculature as well. As I still mentioned above, originally, interferential therapy was introduced by Hans NEMEC (1947/1950-1960) with the aim to make the stimulating (stimulatory) effects of traditional electrotherapy more comfortable: two unmodulated middle frequency currents with slightly different frequencies should be superimposed within the tissue to generate interferential beats, a special kind of amplitude modulation. The low frequency of beat generation or amplitude modulation respectively determines the frequency of the neuronal responses, that means the frequency of action potentials. Therefore, the differences between the two middle frequencies have to be within the low frequency range, that means mostly between > 0 Hz and 100 Hz. In comparison to the interferential therapy and later introduced other modifications of middle frequency therapy for the development of high tone therapy (MAY, 2002) higher frequencies and greater frequency ranges are included: Interferential therapy mostly is using middle frequencies around 4000 Hz, in some equipment moderately higher frequencies but below 10000 Hz. However, the newest version of high tone therapy equipment, more exactly “high tone power therapy” equipment, HiToP®, are able to generate frequencies up to 215 Hz (32768 Hz), and between 212 Hz (4096 Hz) and 215 Hz 73 different frequencies are available. In comparison to NEMEC’s interferential therapy the highest frequency in HiToP® equipment is more than eight times higher, and the range of frequency modulation is more than 286 times higher: 28672 Hz in comparison to 100 Hz. In comparison to the interferential therapy and later introduced other modifications of middle frequency therapy for the development of high tone therapy (MAY, 2002) higher frequencies and greater frequency ranges are included: Interferential therapy mostly is using middle frequencies around 4000 Hz, in some equipment moderately higher frequencies but below 10000 Hz. However, the newest version of high tone therapy equipment, more exactly “high tone power therapy” equipment, HiToP®, are able to generate frequencies up to 215 Hz (32768 Hz), and between 212 Hz (4096 Hz) and 215 Hz 73 different frequencies are available. In comparison to NEMEC’s interferential therapy the highest frequency in HiToP® equipment is more than eight times higher, and the range of frequency modulation is more than 286 times higher: 28672 Hz in comparison to 100 Hz. For therapeutic purposes mostly the mentioned 73 frequencies in logarithmic steps between 212 Hz and 215 Hz are used. The factor is 2-24 corresponding a little bit less than 1,03. Because of the great distance between the lower and the upper corner frequency linear steps were not suitable. The “distances” between the neighbouring frequencies of tones in our music are defined too as logarithmic steps. The factor for the elevation in half tone steps is 2-12. The decision for the term “high tone frequency therapy”, abbreviated “high tone therapy”, derived from relations to tones or music respectively, resulted from the following considerations: 1.) The term “high tone frequency” is more concrete than “middle frequency”. The high tone frequency range (~ 1000 20 000 Hz) covers the low middle frequency range. 2.) The frequencies of the first generation of equipment varied in the high tone frequency range only. The new generation, HiToP®, includes even frequencies of the ultrasound range. Nevertheless, the introduced term has not been changed besides in Poland; there the term “energy tone therapy” is preferred. Both terms are ingenious: “high” characterises the means, namely the high tone frequencies as the agens for the possibility for an easier application of more energy, “energy” this purpose itself. 3.) The distances between the frequency steps correspond to distances of quarter tone steps in music. 4.) By means of frequency scanning the probability of resonance phenomena within structures of the treated tissue should be increased. Resonance plays an important part in music too. 5.) The new term should emphasise the great difference to traditional middle frequency units. 6.) It is possible and useful to explain the modes of action of HiToP® by an loud-speaker. It facilitates the understanding of the physical realisation of the various “programs”, SimulFAMi and the variations of SimulFAMx using modulation frequencies between 0.1 and 200 Hz. The demonstration of hearing emphasises the relation to tones and the absence of similarity to a “current” as a great river.” Main differences between traditional electrotherapy and high tone power therapy (HiToP®) 1. Main differences in comparison to direct current (DC) and low frequency currents with DC-components: HiToP is without any risks of DC as chemical burning caused by electrolysis. Vasodilatation and acceleration of reabsorption of topically applied substances in the treatment area, known as DC-iontophoresis, can be achieved by HiToP too, but by other mechanisms: vasodilatation via fatiguing stimulatory effects upon sympathetic fibres, and the acceleration of resorption via an electrochemical shaking effect resulting in facilitation of diffusion. 2. Main differences in comparison to low frequency currents: HiToP has important advantages: Great superiority concerning local and systemic tolerance, very much greater spectrum of effects by additional sophisticated utilisation of non-stimulatory effects. 3. Main differences in comparison to traditional middle frequency equipment: The most important difference or advantage respectively is basing on the ability of HiToP to generate very much (up to circa 50 times) more power without any discomfort or systemic risks for the patient in comparison to traditional middle frequency equipment. HiToP offers 5000 mW as maximum output per channel; this limit of the output is prescribed by law. Additional advantageous differences: The greater frequency range increases the probability of resonance. SimulFAMx, used for stimulation of nerves including motor and sympathetic fibres, can be adjusted as more brusque (“combined” or “parallel” stimulation) or softer (“paradoxical” stimulation) according the slope of the graph representing the simultaneous modulation of frequency and amplitude. SimulFAMi can be used to minimise or avoid stimulatory effects The spectrum of indications - unbelievable large on the first view: 1. Pain (5 pain-relieving effects are available in HiToP®) 2. Chronic inflammations 3. Degenerative diseases, for example osteoarthritis 4. Diseases of nerves and muscles, for example symptoms resulting from central and peripheral pathological affection of the nervous system as spasticity in cases of cerebral palsy or multiple sclerosis 5. Edema 6. Mental-emotional disturbances 7. Functional disorders of the abdominal organs (Constipation, meteorism, dyskinesias, symptoms of CROHN's disease and colitis 8. Bronchial asthma 9. Itch 10. Sleeplessness 11. Functional arrhythmia of the heart 12. Metabolic disturbances and resulting diseases as for instance diabetic polyneuropathy The 5 pain-relieving effects of HiToP®: 1. The electrochemical shaking effect - present in all kinds of application 2. The real blocking effect - caused by unmodulated alternating fields distinctly above the sensation threshold 3. The pseudoblock - caused by unmodulated alternating fields 4. Counter-irritation - SimulFAMX 100 Hz 5. Indirect pain relief by edema reduction - SimulFAMX 10 Hz Furthermore, HiToP® can be used for the following aims of treatment: 1. Acceleration of healing processes 2. Rehabilitation in cases of peripheral or central neuronal lesions or after immobilisation 3. Prevention of venous thrombosis by means of calf muscle stimulation 4. Mobilisation of geriatric patients after long time of bed rest Scientific explanations of the manifold effects in question and answer _______ Contraindications: Pacemaker Acute bacterial infections (local or systemic) End of theory, part 2 Practice, part 2 Practice, part 2 Big tac, bimanual gliding transcutaneous application of currents using HiToP® as especially comfortable electrical massage, for the enhancement of the efficacy during the manual lymphdrainage, for the detection of trigger points, for the treatment of BELL's palsy, for the manual-digital stimulation of acupuncture points, for the massage of reflex-zones of hands and feet End of practice, part 2 Results of the study of RHADES and SCHNEIDER concerning low back pain 18 patients had been treated. The range of motion could be improved by 5.3° ( statistically significant. 4.7°), The distance of the fingers to the ground could be diminished by 3.7 cm ( 4.0) cm, (significant). Pain relief after the end of the treatment series in 8 patients (44%), later additionally in 3 patients (16.6%), together circa 60%. Degree of pain relief: Statistically high significant improvement from 6.25 ( 3.44 ( 1.82) (NAS-Score). 1.73) to Judgement of the efficiency 40% 30% 20% 10% 0% very good good doctor moderate bad patients Fig.1 Judgement of the efficiency Low back pain caused by problems of the lumbar part of the vertebral column Mean value (°) 130 120 110 100 90 80 70 1st treatment last treatment bowing follow-up examination range of motion Fig. 2 Effects upon bowing and range of motion