Dig-Lecture3 - UMF IASI 2015
advertisement

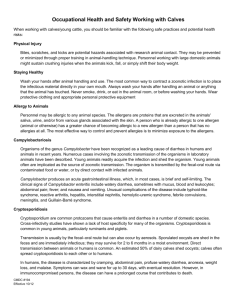
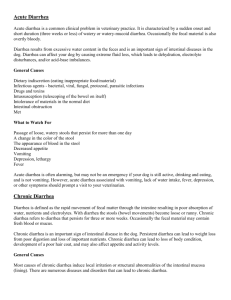
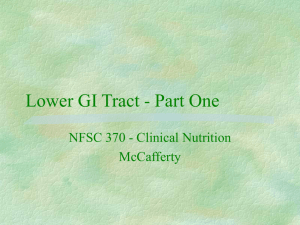
Normal histology • • Layers: Mucosa Submucosa Muscularis propria (externa) Subserosa Serosa - contains mesothelial lining, loose connective tissue • Lamina propria: contains loose connective tissue, lymphocytes, plasma cells, occasional eosinophils, macrophages, mast cells, neutrophils Mucosa • contains villi with central blood vessels, lymphatics • epithelium • lamina propria • muscularis mucosa Mucosa • Villi: contain microvilli; contain primarily columnar absorptive cells and goblet cells • Absorptive cells: have microvilli on luminal surface (brush border) and underlying mat of microfilaments (terminal web) Crypts of Lieberkuhn • lower 20% of epithelium, contain undifferentiated (immature) crypt cells, Paneth cells (have large, apical eosinophilic granules containing antimicrobial proteins), scattered goblet cells and endocrine cells • secrete ions, water, IgA, antimicrobial peptides into lumen • crypt cells take 3-8 days to migrate to surface; allows for rapid repair, but also causes these cells to be sensitive to radiation therapy and chemotherapy Submucosa • contains connective tissue, blood vessels, lymphatics, submucosal (Meissner’s) plexus Muscularis propria (externa) inner circular and outer longitudinal layer, with myenteric (Auerbach’s) plexus between these layers; plexus also contains interstitial cell of Cajal, ganglion cells, fibroblasts Auerbach’s cells • Interstitial cell of Cajal =type of interstitial cell found in the gastrointestinal tract that serves as a pacemaker which creates the basal electrical rhythm leading to peristalsis • ganglion cells=special nerve cells in the intestine that make the muscles push; congenital aganglionosis-Hirschsprung's disease • fibroblasts=produce the extracellular matrix and participate in the transport of absorbet metabolites to the blood and lymphatic apillaries Endocrine cells • similar to cells in pancreas, biliary tree, lung, thyroid, urethra • contain fine eosinophilic granules with secretory proteins • nuclei on luminal side of granules, not basal - Serotonine (enterocromafine) - Gastrine (G) - Secretine (S) - Enteroglucagon (EG) DISEASES OF THE INTESTINE Congenital anomalies • • • • • Meckel diverticulum Duplications Intestinal atrezia & stenosis Malrotation Gastroschisis & omphalocele Meckel diverticulum • During early gestation, the omphalomesenteric or vitelline duct connects the fetal yolk sac to the primitive gut. By 7 to 8 weeks of gestation, this duct is normally completely obliterated. • A Meckel diverticulum, results when this structure fails to resorb completely. Symptoms • most adults remain asymptomatic • intestinal obstruction is manifested by cramping abdominal pain, obstipation, nausea and vomiting • acute Meckel's diverticulitis is characterized by abdominal pain and tenderness typically localized below or to the left of the umbilicus; it is often accompanied by vomiting and is similar to appendicitis except for location of pain. • bleeding- typically resulting in melena rather than frank blood. Signs • voluntary guarding with mild tenderness - in the absence of strangulation, the abdomen is not tender - with infarction, the abdomen becomes tender and auscultation reveals a silent abdomen or minimal peristalsis • hyperactive, high-pitched peristalsis with rushes coinciding with cramps is typical • sometimes, dilated loops of bowel are palpable • shock and oliguria are serious signs that indicate either late simple obstruction or strangulation Diagnosis • based on symptoms • flat and upright X-rays of the abdomen (vomiting and signs of obstruction) • CT scan with oral contrast (for abdominal pain and focal tenderness) • wireless capsule • radionuclide scan - 99mTc pertechnetate scan may identify ectopic gastric mucosa and hence the diverticulum (if rectal bleeding is suspected to originate from a Meckel's diverticulum) Barium X-ray Axial contrast-enhanced CT scan shows blind-ending Meckel's diverticulum with thickened mucosal folds (arrow). Pathology confirmed ectopic gastric mucosa in Meckel's diverticulum. Giant Meckel diverticulum in a 21-year-old man who was referred for wireless capsule endoscopy because of chronic abdominal pain and anemia. Results of a small bowel follow-through study, radionuclide examination, and endoscopy of the upper and lower gastrointestinal tract were unremarkable. (a) Wireless capsule endoscopic image shows a shallow ulcer in one segment of the ileum (arrow). Other images showed ulcers in an adjacent segment and possibly in the colon. Doublecontrast barium enteroclysis was requested to determine the extent of Crohn disease. (b) Double-contrast air-barium enteroclysis image shows a large saccular dilatation (arrowheads) in a pelvic segment of the ileum. Scattered ulcerations (arrow) are seen adjacent to the point of attachment of the dilatation to a normal-appearing loop of ileum. Results of surgery confirmed the presence of a giant Meckel diverticulum with ulcerations. There was no evidence of Crohn disease. Technetium-99m pertechnetate scan in a 12-year-old boy who presented with intermittent dull abdominal pain and a mild iron deficiency anemia. On the present occasion, the pain appeared more severe and was associated with occasional vomiting; thus, the child was hospitalized. This 90-minute delayed image shows focal activity in the mid abdomen. The activity is more diffuse than is expected with Meckel diverticulum. At surgery, an inflamed Meckel diverticulum containing ectopic gastric mucosa was removed. The Meckel diverticulum had intussuscepted into the terminal small bowel. Differential diagnosis • • • • • • • • • appendicitis intestinal polyposis syndromes colitis intussusception colonic vascular malformations juvenile polyps necrotizing enterocolitis Crohn disease ulcerative colitis Complications • The risk for complications dramatically decreases with age, and most adults with a Meckel diverticulum remain asymptomatic. • Complications develop in approximately 2% of all adults with a Meckel diverticulum: - bleeding - intestinal obstruction - diverticulitis - perforation - carcinoma Obstruction is caused by: • intussusception of the diverticulum into adjacent bowel • volvulus around or herniation into a fibrous band • entrapment in inguinal, femoral or umbilical hernia sacs (Littré hernia) • inflammation and scarring leading to blockage around the diverticular neck and adjacent ileum Structural anomalies • • • • Volvulus Intussusception Lymphangiectasia Celiac artery compression Volvulus • abnormal twisting of the intestine around the axis of its own mesentery, resulting in obstruction of the more proximal bowel • twisting of the mesentery may involve the mesenteric vessels and so make the involved loop particularly susceptible to strangulation and gangrene, with resulting perforation, peritonitis and sepsis Symptoms • often has an abrupt onset - abdominal pain continuous, sometimes with superimposed waves of colicky pain - obstipation - nausea - vomiting - marked abdominal distention Signs • • • • • abdominal distention rebound guarding rigidity a palpable abdominal mass (occasionally) Complications • SURGICAL EMERGENCY! • • • • • strangulation of the twisted bowel loop loss of blood supply deterioration perforation fatal peritonitis when the bowel material infects the abdominal cavity Investigations • abdominal and chest X-rays may show the obstruction and abnormal air-fluid levels in the bowels • barium enema X-ray shows typical volvulus shapes • CT • white blood cell count will be higher than normal Radiological investigations • Plain abdominal radiographs taken in supine and upright positions may demonstrate distended bowel with air-fluid levels, consistent with obstruction. • Perforation may be indicated by the presence of free air. • A typical corkscrew-like appearance of the barium in the distorted duodenum and jejunum is diagnostic. • Angiography may reveal twisting of the branches of the superior mesenteric artery. X-ray Small-Bowel Obstruction (Supine) Small-Bowel Obstruction (Upright) Dysmotility • Chronic small intestine pseudoobstruction - it may be secondary to neuropathy or myopathy - abnormalities of small bowel ICCs - there is some evidence of a genetic association - it can occur in conjunction with Kawasaki disease or Parkinson's disease Dysmotility-causes Primary Secondary • Familial visceral myopathies • Mithocondrial DNA and myopathies • Familial visceral neuropathies • Congenital neuropathic motility disorders • MEN type 2B • Non-familial visceral myopathies • Idiopatic non-familial visceral neuropathies • • • • • • • • • • • • • • • • Scleroderma Dermatomyositis and polymyositis Systemic lupus erythematosus Mixed connective tissue disease Diabete mellitus Parkinson disease Neurofibromatosis Spinal cord injury Paraneoplastic visceral neuropathy Myotonic distrophy Amiloidosis Thyroid disease Hypoparathyroidism Drug-induced changes in small intestine motility Celiac disease Irradiation Clinical findings • Isolated severe small intestinal dysmotility is very unusual; small intestinal dysmotility is generally associated with dysmotility in other parts of the digestive tract. • asymptomatic • recurrent symptoms and signs of small intestinal obstruction = chronic small intestinal pseudoobstruction Symptoms • Between those two ends of the spectrum, the patient may have recurrent symptoms - postprandial cramping - periumbilical and epigastric abdominal pain - abdominal bloating - easy satiety - anorexia - weight loss - nausea - vomiting • symptoms are usually related to eating. • diarrhea can occur in patients with bacterial overgrowth and malabsorption. • in severe cases, the patients have episodes of chronic intestinal pseudoobstruction syndrome Signs • cachectic and malnourished • the abdomen may be distended and mildly tender • the bowel sounds are inactive and infrequent in patients with smooth muscle dysfunction, but they are hyperactive and high-pitched in those with myenteric plexus dysfunction • in those with chronic intestinal pseudoobstruction, during an obstructive episode, the abdominal examination findings may be indistinguishable from those of true mechanical obstruction • symptoms and signs of multiple-organ dysmotility Complications • malnutrition • bacterial overgrowth • pneumatosis cystoides intestinalis - rare condition characterized by multiple, gas-filled cysts in the wall of the small and large intestine. Pneumoperitoneum may occur. Investigations • • • • • • Blood tests Plain abdominal X-ray Enteroclysis Whole-gut transit with radiopaque markers Radioactive isotope transit by scintigraphy Small intestinal manometry Blood tests • Blood cell count: anemia and macrocytosis • Blood chemistries: malnutrition, malabsorption Plain abdominal X-ray • during exacerbations, show multiple air-fluid levels and dilation of the small intestine Enteroclysis Spot radiograph of small intestine from enteroclysis shows marked dilation of the mid small intestine. The luminal diameter is 9 cm (double arrow). Despite the marked luminal dilation, the valvulae conniventes are tightly packed. The folds are smooth and of normal caliber Scleroderma (Small Bowel) Differential diagnosis between chronic intestinal pseudoobstruction and mechanical obstruction • Partial small bowel obstruction from adhesions, tumors, intussusception or stricture can mimic chronic intestinal pseudoobstruction. • Enteroclysis or careful small bowel radiography with fluoroscopy is probably the most helpful way to differentiate chronic intestinal pseudoobstruction from mechanical obstruction. • In most cases, exploratory laparoscopy may be necessary to rule out an obstructing lesion. Infections Acute • Common bacteria • Viral pathogens • Traveller’s diarrhea Chronic • Whipple disease • Tropical sprue • Tuberculosis • Mycotic infections Pathophysiology Host factors Microbial factors • Normal intestinal flora • Control mechanisms • Intestinal immunity • number of organisms • enterotoxins • adherence to gut mucosa • invasion of enterocytes Clinical manifestations • • • • • • • • Diarrhea Nausea and vomiting Loss of appetite Fever Headaches Abnormal flatulence Abdominal pain Bloody stools (dysentery - suggesting infection by amoeba, Campylobacter, Salmonella, Shigella or some pathogenic strains of Escherichia coli) Diagnosis • diagnosing gastroenteritis is mainly an exclusion procedure • in rare cases when the symptoms are not enough to diagnose gastroenteritis, several tests may be performed in order to rule out other gastrointestinal disorders. - rectal examinations - complete blood count - electrolytes - kidney function tests • when the symptoms are conclusive, no tests apart from the stool tests are required Diarrhea - the most common manifestation of intestinal tract infections • Young children and the elderly are at greatest risk for more severe disease and complications. • The presence of underlying medical conditions, especially those that compromise immunity, greatly enhances the risk of acquiring an infection and its ultimate severity. • Poor sanitation, inadequate water supplies and increasing globalization of food transport systems all predispose to the development of large epidemics of food- and water-borne outbreaks of gastrointestinal disease. • Seasonal or cyclic weather variations also influence the epidemiology of diarrhoeal disease and food poisoning. Is just a little case of diarrhea… • Second leading causes of all death worldwide • Most common cause of morbidity and mortality in children worldwide • Accounts for 9% of hospitalizations in children <5 years old in the United States • You will likely suffer from diarrhea in the near future! Definition • >3 feces/day, > 200 g/day • acute/chronic • Physiology: – in gastrointestinal tract 9-10 l fluids (2l ingestion, the rest secretions); – Na - co-transport with Cl and glucose in small bowel and biliary salts in terminal ileum; cotransport with H - HCO3; K absorbed with H or Ca. – parasimpatic is stimulating the peristalsis and electrolyte secretion; simpatic nerves are doing the opposite. – enteric nervous system Figure 4.1 - Water fluxes through the intestine ©Copyright Science Press Internet Services Functional design of small intestine Acute diarrhea - definition • Stool weight in excess of 200 g/day • 3 or more loose or watery stools/day • Alteration in normal bowel movement characterized by decreased consistency and increased frequency • Less than 14 days in duration Etiology • Viral: 70-80% of infectious diarrhea in developed countries • Bacterial: 10-20% of infectious diarrhea but responsible for most cases of severe diarrhea • Protozoars: less than 10% Epidemiology • 1.2-1.9 episodes per person annually in the general population • 2.4 episodes per child <3 years old annually • 5 episodes per year for children <3 years old and in daycare • Seasonal peak in the winter Viral Diarrhea • Rotavirus • Norovirus (Norwalk-like) • Enteric Adenovirus • Astrovirus Rotavirus • Leading cause of hospitalization for diarrhea in children • Most prevalent during winter season • Fecal-oral transmission: viral shedding can persist for 21 days • Acute onset of fever followed by watery diarrhea (10-20 BM/day) and can persist for up to a week Mechanism Norovirus • Most common cause of diarrheal outbreaks/epidemics • Multiple modes of fecal-oral transmission • Acute onset of nausea and vomiting, watery diarrhea with abdominal cramps and can persist for 1-3 days Enteric adenovirus • Primarily affects children < 4 years old • Fecal-oral transmission • Clinical picture similar to rotavirus (fever and watery diarrhea) Astrovirus • Primarily affects children < 4 years old and immunocompromised • Seasonal peak in the winter • Fecal-oral transmission: viral shedding can occur for several weeks • Fever, nausea and vomiting, abdominal pain and diarrhea lasting up to a week Symptoms of viral enteritis • low grade fever • nausea • vomiting • abdominal cramps • watery diarrhea lasting up to 1 week • Viral shedding can occur for weeks after symptoms resolve Bacterial diarrhea • Campylobacter • Salmonella • Shigella • Enterohemorrhagic Escherichia coli Campylobacter • Most common bacterial pathogen • Transmitted through ingestion of contaminated food or by direct contact with fecal material • diarrhea (+/- blood), abdominal cramps (can be severe), malaise, fever • Usually self-limited and does not require antibiotics Salmonella • Most common in children <4 years old and a peak in the first few months of life • Transmitted via ingestion of contaminated food and contact with infected animals • fever, diarrhea and abdominal cramping • Antimicrobial therapy can prolong fecal shedding Mechanism Shigella • Fecal-oral transmission • fever, abdominal cramps, tenesmus, and mucoid stools with or without blood • Can lead to serious complications • Antimicrobial treatment shortens duration of illness and limits fecal shedding Mechanism E. Coli O157:H7 • Transmission via contaminated food and water • bloody diarrhea, severe abdominal pain, and sometimes fever • Can lead to serious complications • Antibiotics have no proven benefit and may increase the risk of complications Symptoms of bacterial enteritis • Can affect all age groups • Fecal-oral transmission, often through contaminated food • bloody diarrhea, severe cramping and malaise • Antibiotic treatment not always necessary History and Physical Exam • 3 main goals – Estimate the level of dehydration – Identify likely causes on the basis of history and clinical findings – Determine if additional studies and/or medications are necessary History • Onset, frequency, quantity, and character of diarrhea • Associated symptoms: nausea, vomiting, fever, abdominal pain, tenesmus, malaise • Recent oral intake • Signs and symptoms of dehydration Tenesmus • Tenesmus is the feeling that you constantly need to pass stools, even though your bowels are already empty. • It may involve straining, pain, and cramping. • Usually occurs with inflammatory diseases of the bowels. • It can also occur with motility disorders. Malaise • Malaise is a generalized feeling of discomfort, illness or lack of well-being. • Malaise is a symptom that can occur with almost any significant health condition. • It may start slowly or quickly, depending on the type of disease. • Fatigue occurs with malaise in many common diseases. Mailaise can be accompanied by a feeling of not having enough energy to accomplish usual activities. Physical Exam • Vitals, vitals, vitals! • Abdominal exam • Presence of occult blood • Signs of dehydration Dehydration • particularly dangerous in children, older adults and people with weakened immune systems • must be treated promptly to avoid serious health problems, such as organ damage, shock or coma • • • • thirst less frequent urination than usual dark-colored urine dry skin, does not flatten back to normal right away after being gently pinched and released • fatigue • dizziness • light-headedness Laboratory evaluation • Unnecessary for patients who present within 1 day from onset of diarrhea • Warning signs/symptoms: bloody diarrhea, high fever, severe abd pain, dehydration or comorbid condition • Fecal leukocytes followed by bacterial culture, ova & parasites, viral antigens • CBC, chemistries TRAVELER’S DIARRHEA • substantial risk (~40%) for diarrheal disease • To some degree, the specific agents that cause traveler’s diarrhea vary by geographic region and season. • Giardia and Cryptosporidium appear to be common causes of diarrheal disease in visitors to Russia • Aeromonas spp appear to be very common causes of traveler’s diarrhea in visitors to Thailand • toxigenic E coli is somewhat more frequently encountered during the warmer summer months • Campylobacter jejuni appears to occur more frequently in the winter months Clinical features • Traveler’s diarrhea usually occurs within the first 14 days of travel. • It can also occur within a week or more after return from a foreign country. • The diarrhea is usually characterized as watery, with the passage of three to ten bowel movements a day for 2 to 5 days. • Abdominal cramps and pain often accompany the illness. • Fewer patients experience fever, chills, vomiting and dysentery-like symptoms. • Fewer than 10% of patients have an illness that lasts longer than a week and about 2% of patients have illness lasting a month or more Diagnosis • Rarely is diagnosis required or available in the setting of acute watery traveler’s diarrhea. • For cases of dysentery, a diagnosis, if available, is more useful. • Given that traveler’s diarrhea occurs in the traveling patient, it is almost always reasonable to initiate treatment without an etiologic diagnosis. • Stool examination for parasites is warranted only in cases of prolonged illness. Chronic diarrhea - definition • >3 weeks duration • usually means three or more loose stools per day • average fecal daily weight in normal person is 100-200grams/day Approach to patient • Patient should be questioned about the onset, duration, pattern, aggravates (especially diet), relieving factors and stool characteristics • Presence or absence of fecal incontinence, fever, weight loss, pain, certain exposurestravel, medications, contacts with diarrhea should be noted Approach to patient • On physical exam, check for thyroid mass, wheezing on lung exam, heart murmurs, edema, hepatomegaly, abdominal mass, LAD, perianal fistula or anal sphincter laxity. • If diagnosis is still unclear after initial encounter, further testing is required • secretory vs. osmotic diarrhea vs. malabsorption vs. inflammatory Tests • Stool culture - a sample of stool is analyzed in a laboratory to check for bacteria, parasites, or other signs of disease and infection. • Blood tests - can be helpful in ruling out certain diseases. • Fasting tests - to find out if a food intolerance or allergy is causing the diarrhea, the doctor may ask a person to avoid foods with lactose, carbohydrates, wheat, or other ingredients to see whether the diarrhea responds to a change in diet. Complications • • • • Dehydration Malnutrition Electrolytes (minerals) deficiencies Finally, there may be irritation of the anus due to the frequent passage of watery stool containing irritating substances Malabsorptive diarrhea • Malabsorption suspected in patients with weight loss, greasy stools, glossitis, anemia and hypoalbumenima • If malabsorption suspected, a 72 hr stool specimen should be sent for fecal fat determination, if + =>suspect malabsorption • Causes of malabsorption include pancreatic insufficiency (confirmed by CT/pancreatic function tests) and disease of small intestine--Whipple’s disease, tropical sprue, intestinal lymphoma (small bowel biopsies by EGD) Malabsorptive Diarrhea-Mucosal Malabsorbtion • Celiac sprue - hypersensitivity to gluten • Tropical sprue - infectious disease of unknown origin, seen in Indian subcontinent, Asia, West Indies, North & South America, central and southern Africa, and Central America Mucosal Malabsorptive • Whipple’s ->infection form Treponemawhippelii. • Diagnosed by + biopsy for PAS macrophages • Associated symptoms include hypersomnolescence, arthralgias, fever, hypotension and LAD Intraluminal Malabsorbtion • Most commonly results from pancreatic exocrine insufficiency when >90% of pancreatic secretory function is lost • ethanol abuse • cystic fibrosis • pancreatic duct obstruction Secretory vs Osmotic • check stool osmotic gap • 290-2x[Na stool + K stool] • If < 50, diarrhea falls under secretory category TYPICAL FEATURES OF SECRETORY DIARRHEA TABLE 4-5. TYPICAL FEATURES OF SECRETORY DIARRHEA Voluminous, watery stools Little or no fecal osmotic gap, stool pH near 7.0 Usually persists during fasting Usually no pus, blood, or excess fat in stools Secretory Diarrhea • Characterized by watery, large-volume fecal outputs that are typically painless and persist with fasting - one may do a 24 hr stool quant. -should exceed one liter and not decrease with fasting • Usually stool pH is neutral and fecal fat test is negative TABLE 4-6. M ECHANISMS AND CAUS ES OF S ECRETORY DI ARRHEA Reduction in mucosal surface area Postresection diarrhea Short-bowel syndrome Extensive mucosal disease and Inflammation Viral gastroenteritis Celiac disease Whipple`s disease Crohn`s disease Lymphoma Absence of ion transport mechanism Congenital chloridorrhea Bacterial toxins Cholera Enterotoxigenic Escherichia coli Shigella Staphylococcus Clostridium perfringens Luminal secretagogues Bile acids Fatty acids, hydroxy-fatty acids Phenolphthalein, ricinoleic acid, bisacodyl Circulating secretagogues Gastrin (Zollinger-Ellison syndrome) Vasoactive intestinal polypeptide (VIPoma, ganglioneuroma, neuroblas toma, pheochromocytoma) Calcitonin, prostaglandins (medullary carcinoma of the thyroid) Somatostatin (somatostatinoma) Glucagon (glucagonoma) Serotonin, kinins (carcinoid tumor) Thyro xine (hyperthyroidism) Histamine (mastocytosis) Secretory diarrhea - investigations • If secretory diarrhea confirmed, recommend checking serum should be sent for: • Gastrin (gastrinoma), VIP(VIPOMA), glucagon (glucogonoma), serotonin (carcinoid), calcitonin, histamine, and prostaglandins • -if overproduction of one of these mediators is documented abdominal CT scan is recommended Carcinoid Syndrome and Secretory Diarrhea • Carcinod present with watery diarrhea, flushing, skin changes, bronchospasm and cardiac murmurs which are all symptoms caused by secretion of serotonin, histamine, catecholamines, kinins and prostaglandins by the tumor masses • 1/3 pts with carcinoid present with diarrhea alone Sectretory diarrhea – differential diagnosis • Other conditions to consider include: • Diseases like Crohn’s ileitis or resection of <100cm of terminal ileum (dihydroxy bile acids may escape absorption and stimulate colonic secretion) Osmotic Diarrhea • Most common cause is lactase deficiency • Magnesium ingestion or factitious laxative abuse • Intraluminal maldigestion is also seen in cirrhotics and bile duct obstruction-there is impaired delivery of bile salts to small intestine, leads to poor micelle formation with ingested fats CHRONIC DIARRHEA -Investigation• Blood tests: ESR; hemo leucograme (anemia, inflammation); proteinograme (hyposerinemia) • Rectosigmoidoscopy, Colonoscopy with/without biopsy/ UGI endoscopy ( differential diagnosis ) • Rx: small bowel/barium enema • Chronic diarrhea: Abdominal X-Ray, US/ CT Celiac disease • Coeliac disease is an inflammatory disorder of the small intestine induced by the prolamins of certain cereals, namely the gliadins of wheat, hordeins of barley and secalins of rye. • The inflammation is associated with loss of villous height and crypt hypertrophy and leads to malabsorption. (a) Dissecting microscopic appearance of a normal jejunal biopsy. (b) Dissecting microscopic appearance of coeliac disease. Pathogenesis • There are two clear facts about the etiopathogenesis of coeliac disease. 1. The first is that fractions of gliadin, the alcoholsoluble component of gluten, are the toxic dietary constituent, together with similar fractions of rye and barley prolamins. 2. The second is that there is a genetic susceptibility to gluten intolerance because of the close association with the HLA haplotype B8DR3-DQ2 in northern Europeans and with B8DR5/7-DQ2 in southern Europeans. Clinical findings • Coeliac disease in infants classically presents soon after weaning at the point that cereals are introduced. • In adults, the most common presentations are anaemia and variable abdominal symptoms of discomfort, bloating, excess wind and an altered bowel habit (diarrhea). Mouth ulcers are also frequent and can be the presenting symptom. Diagnosis • The crucial test to establish the diagnosis is a small-intestinal biopsy. • Several serological tests have been developed as screening tests - antibodies to gliadin (IgA or IgG isotype) - IgA antibodies to reticulin - IgA antibodies to endomysium Diagnosis • Assessment of malabsorption • Full blood count (hemoglobin level may be low, folate deficiency, vitamine B12 - concentrations • are only low in patients with extensive involvement of the small intestine and so are usually normal) • Biochemistry – hypokalaemia, hypomagnesiemia, hypocalcaemia, serum albumin is often low, as is the concentration of zinc; faecal fat excretion • Immunological tests • Radiology • Small-intestinal biopsy Small intestinal biopsy • This has traditionally been taken from the duodenal–jejunal junction (the ligament of Treitz) using a Crosby capsule. • a distal duodenal biopsy taken at endoscopy is being used increasingly to make the diagnosis and comparative studies with a true jejunal biopsy have justified its use. Differential diagnosis • • • • • Giardia common-variable hypogammaglobulinaemia Lymphoma Crohn's disease small-intestinal diseases such (radiation, enteritis, amyloid, Whipple's disease) • Dermatitis herpetiformis is commonly associated with an abnormal mucosal biopsy Associated diseases • There is an increased prevalence of autoimmune diseases in patients with coeliac disease: • diabetes • thyroid disease • Addison's disease • fibrosing alveolitis • systemic lupus erythematosus • polyarteritis Short bowell syndrome • Large resections of the small bowel may cause multiple nutritional and other medical abnormalities, now commonly termed the 'short bowel syndrome'. • thrombosis or embolus • multiple surgical resections of the small bowel in patients with Crohn's disease (regional ileitis) Clinical findings • Intractable (cholerheic) diarrhoea • Steatorrhoea • Consequential metabolic abnormalities including vitamin B 12 deficiency • Many patients undergoing resections will be malnourished preoperatively and energy consumption increases in the immediate postoperative period. • If not appropriately managed, long-term proteinenergy malnutrition, as well as life-threatening mineral and vitamin deficiencies develop. Adaptation • The residual bowel undergoes mucosal hyperplasia and its capacity to absorb fluids and nutrients increases over a period of weeks or months. • The molecular events that underly these changes are unclear but may include circulating trophic factors and growth factors present in pancreatic juice or secreted into the intestinal lumen. CONSTIPATION 1. 2. 3. 4. 5. Definition Pathogenesis Risk factors Diagnosis and differential diagnosis Treatment approaches Definition: usually refers to persistent, difficult, infrequent or seemingly incomplete defecation The patient’s view: The following perceptions, • Need for straining (52%) •Hard pellet-like stools (44%) •Inability to defecate when desired (34%) •Infrequent defecation (33%) The clinical view: ROME-CRITERIA (at least 2 in any 12week period); •< 3 bowel movements (BM) per week •Hard stools in > 25% of BM’s •Sense of incomplete evacuation in >25% of BM’s •Excessive straining in >25% of BM’s •The necessity of digital manipulation 2. Causes •Extrinsic •Inadequate dietary fiber, fluid •Ignoring urge to defecate •Structural •Colorectal: neoplasm,stricture,ischemia,volvulus,diverticular disease •Anorectal: inflammation, prolapse, rectocele,fissure, stricture •Systemic •Hypokalemia •Hypercalcemia •Hyperparathyroidism •Hypothyroidism •Diabetes mellitus •Addison’s disease •Pregnancy •Uremia •Neurological •CNS: Parkinson's disease, Multiple sclerosis, trauma, ischemia, tumor •Sacral nerves: trauma, tumor •Autonomic neuropathy •Aganglionosis ( Hirschsprung’s disease ) •Drugs •Analgesics •Anticholinergics •Anticonvulsants •Antihistamines •Antihypertensive •Chemotherapeutic agents •Diuretics •Metal ions •Uncertain Pathophysiology Irritable bowel syndrome, Slow transit constipation (STC) 3. Risk factors Risk situations, groups and factors: •Infants and children •People older than 55 yrs •Recent abdominal or perianal/pelvic surgery •Late pregnancy •Limited mobility •Inadequate diet (fluid or fiber) •Medications especially in the elderly •Laxative abuse •Terminal care patients •Travel •History of chronic constipation 4. Diagnosis and differential diagnosis •History taking •Physical examination •Diagnostic techniques •History taking •Check for age of onset ( sudden or long term) •Check for ROME- II criteria •Check for neurological disorders •Check for psychiatric conditions •Check for family history of constipation? •Physical examination •Palpation of abdomen ( tumour ) •Percussion ( check for gases) •Rectal palpation •Consistency/impaction •Presence of non-fecal masses or abnormalities (tumors, hemorrhoid, fissures) •Presence of blood •Sphincter tone Major alarm symptoms especially in patients >50yrs •New onset constipation •Anemia •Weight loss •Anal blood loss •Positive occult blood test •Sudden changes in defecation pattern and appearance of stool •Diagnostic techniques •Stool analysis •Weighing 3 days; < 100g avg means constipation •Abdominal x-rays •Radiological or endoscopic investigation •Colon tumour, stenosis •Abdominal echography • Tumour mass •Anorectal function tests •Manometry •Electromyography •Rectal mucosal biopsy •Colonic transit time (radiopaque marker) Barium proctography in a healthy subject (A) Barium proctography in a healthy subject (B) Barium proctography in a healthy subject (C) Barium proctography in a healthy subject (D) DEFECOGRAFIA - Distal bowel in Hirschsprung`s disease ©Copyright Science Press Internet Services There is fecal material in the right and left colon (arrows). MALABSORPTION MALABSORPTION – definition Clinical term that encompasses defects occurring during the digestion and absorption of food nutrients by the gastrointestinal tract. • The digestion or absorption of a single nutrient component may be impaired, as in lactose intolerance in lactase deficiency. • When a diffuse disorder such as celiac disease affects the intestine, the absorption of almost all elements is impaired. Pathophysiology: 3 major phases of digestion and absorption of food materials. • Luminal phase: dietary fats, proteins, and carbohydrates are hydrolyzed and solubilized by secreted digestive enzymes and bile. • Mucosal phase: relies on the integrity of the brush-border membrane of intestinal epithelial cells to transport digested products from the lumen into the cells. • Post absorptive phase: reassembled lipids and other key nutrients are transported via lymphatic and portal circulation from epithelial cells to other parts of the body. Pathophysiology of bacterial overgrowth ©Copyright Science Press Internet Services Pathophysiology of lactase deficiency ©Copyright Science Press Internet Services Symptoms • Diarrhea – Diarrhea is the most common symptomatic complaint. – Diarrhea frequently is watery, reflecting the osmotic load received by the intestine. – Bacterial action producing hydroxy fatty acids from undigested fat also can increase net fluid secretion from the intestine, further worsening the diarrhea. • Steatorrhea – Steatorrhea is the result of fat malabsorption. – The hallmark of steatorrhea is the passage of pale, bulky, and malodorous stools. – Such stools often float on top of the toilet water and are difficult to flush. Also, patients find floating oil droplets in the toilet following defecation. Symptoms • Weight loss and fatigue – Weight loss is common and may be pronounced; however, patients may compensate by increasing their caloric consumption, masking weight loss from malabsorption. – The chance of weight loss increases in diffuse diseases involving the intestine, such as celiac disease and Whipple disease. • Flatulence and abdominal distension – Bacterial fermentation of unabsorbed food substances releases gaseous products, such as hydrogen and methane, causing flatulence. – Flatulence often causes uncomfortable abdominal distention and cramps. Symptoms • Edema – Hypoalbuminemia from chronic protein malabsorption or from loss of protein into the intestinal lumen causes peripheral edema. – Extensive obstruction of the lymphatic system, as seen in intestinal lymphangiectasia, can cause protein loss. – With severe protein depletion, ascites may develop. • Anemia – Depending on the cause, anemia resulting from malabsorption can be either microcytic (iron deficiency) or macrocytic (vitamin B-12 deficiency). – Iron deficiency anemia often is a manifestation of celiac disease. – Ileal involvement in Crohn disease or ileal resection can cause megaloblastic anemia due to vitamin B-12 deficiency. • Bleeding disorders – Bleeding usually is a consequence of vitamin K malabsorption and subsequent hypoprothrombinemia. – Ecchymosis usually is the manifesting symptom, although occasionally, melena and hematuria occur. Symptoms • Metabolic defects of bones – Vitamin D deficiency can cause bone disorders such as osteopenia or osteomalacia. – Bone pain and pathological fractures may be observed. – Malabsorption of calcium can lead to secondary hyperparathyroidism. • Neurological manifestations – Electrolyte disturbances such as hypocalcemia and hypomagnesemia can lead to tetany, manifesting as the Trousseau sign and the Chvostek sign. – Vitamin malabsorption can cause generalized motor weakness (pantothenic acid, vitamin D) or peripheral neuropathy (thiamine), a sense of loss for vibration and position (cobalamin), night blindness (vitamin A), and seizures (biotin). Physical findings • General – Patients may have orthostatic hypotension. – Fatigue – Signs of weight loss, muscle wasting, or both may be present. – Patients may have signs of loss of subcutaneous fat. • Abdominal examination – The abdomen may be distended, and bowel sounds may be hyperactive. – Ascites may be present in severe hypoproteinemia. • Dermatological manifestations – Pale skin may reveal anemia. – Ecchymosis due to vitamin K deficiency may be present. – Dermatitis herpetiformis, erythema nodosum, and pyoderma gangrenosum may be present. – Pellagra, alopecia, or seborrheic dermatitis • Neurological examination – Motor weakness, peripheral neuropathy, or ataxia may be present. – The Chvostek or Trousseau sign may be evident due to hypocalcemia or hypomagnesemia. • Cheilosis, glossitis, or aphthous ulcers of the mouth • Peripheral edema TABLE 5-33. SELECTED SYMPTOMS AND SIGNS OF NUTRIENT DEFICIENCIES Symptoms or sign Possible nutrient deficiency Weakness, weight loss, muscle Protein, calorie wasting Pallor Folate, iron, vitamin B12 Follicular hyperkeratosis Vitamin A, vitamin C Perifollicular petechiae Vitamin C Protein, calorie, niacin, riboflavin, zinc, Dermatitis vitamin A, essential fatty acids Bruising, purpura Easily plucked, alopecia Vitamin C, vitamin K Corkscrew hairs, coiled hair Protein, zinc, biotin Night blindness, keratomalacia, photophobia Conjunctival inflammation Glossitis Bleeding or receding gums, mouth ulcers Decreased taste Burning or sore mouth and tongue Angular stomatitis or cheilosis Tetany Paresthesias Loss of reflexes, wrist drop, foot drop, loss of vibratory and position sense Dementia, disorientation Ophthalmoplegia Depression Vitamin C, vitamin A Vitamin A Vitamin A, riboflavin Riboflavin, niacin, folate, vitamin B12, protein Vitamin A, vitamin C, vitamin K, folate Zinc, vitamin A Vitamin B12, vitamin C, niacin, folate, iron Riboflavin, niacin, pyridoxine, iron Calcium, magnesium Thiamine, pyridoxine Vitamin B12, vitamin E Niacin, vitamin B12 Vitamin E, thiamine Biotin, folate, vitamin B12 TABLE 5-1. CLASSIFICATION OF DISEASES THAT CAUSE INTESTINAL MALABSORPTION Premucosal Mucosal Postmucosal Pancreatic insufficiency Celiac sprue Congenital lymphangiectasia Hepatobiliary disease Tropical sprue Secondary lymphangiectasia Bacterial overgrowth Whipple`s disease Rapid intestinal transit Eosinophilic enteritis Gastrectomy Brush border enzyme deficiency Lymphoma Short-bowel syndrome Prolonged malnutrition Radiation enteritis Parasitic infection Mesenteric ischemia Massive small-bowel resection can cause significant malabsorption TABLE 5-16. PREDI CTED NUTRITIONAL OUTCOME IN PATIENTS WHO HAVE HAD MASSIVE INTESTI NAL RESECTION Remaining Jejunal length, cm 0-50 51-100 101-150 151-200 >200 ©Copyright Science Press Internet Services Colon Nutritional outcome - TPN + TPN - IVFM/TPN + Modified oral diet - Regular or modified oral diet + Regular diet - Modified oral diet + Regular diet - or + Regular diet Differentials: • Zollinger-Ellison Syndrome Other Problems to be Considered: – Amino acid deficiencies (cystinuria) – Cystic fibrosis – Hartnup disease – Tropical jejunitis – Whipple disease Workup : TABLE 5-32. INITIAL EVALUATION OF PATIENT WITH POSSIBLE MALABSORPTION History and Physical Examination Initial blood tests Follow-up laboratory tests Complete blood count Serum iron Prothrombin time Serum folate Standard electrolytes Serum vitamin B12 Calcium Serum vitamin A Magnesium Plasma 25-hydroxy vitamin D Blood urea nitrogen Urinary oxalate excretion Creatinine Stool for Sudan stain Alkaline phosphatase Stool for ova and parasites Cholesterol Total protein and albumin Imaging studies – Small bowel barium studies. – CT-scan of the abdomen. – Endoscopic retrograde cholangiopancreatogram – Plain abdominal X-ray film. – Endoscopy Endoscopy Upper endoscopy with small bowel mucosal biopsy • Establishing a definitive diagnosis of malabsorption of the mucosal phase often can be achieved by histological examination of biopsied mucosal specimens obtained during routine upper endoscopy. • Examples of conditions that can be diagnosed this way include celiac sprue, giardiasis, Crohn disease, Whipple disease, amyloidosis, abetalipoproteinemia, and lymphoma. Endoscopic image of scalloping seen in celiac disease and other mucosal disorders including giardiasis Other studies – Tests of fat malabsorption. – D-xylose test. – Test of carbohydrate absorption. – Test of bile salt absorption. – Schilling test. URINARY D-XYLOSE TEST • The urinary D-xylose test for carbohydrate absorption provides an assessment of proximal small-intestinal mucosal function. D-Xylose, a pentose, is absorbed almost exclusively in the proximal small intestine. • The D-xylose test is usually performed by giving 25 g Dxylose and collecting urine for 5 h. • An abnormal test (4.5 g excretion) primarily reflects the presence of duodenal/jejunal mucosal disease. • The D-xylose test can also be abnormal in patients with blind loop syndrome (as a consequence primarily of abnormal intestinal mucosa) and, as a false-positive study, in patients with large collections of fluid in a third space (i.e., ascites, pleural fluid). The Schilling test • Is performed by administering 58Co-labeled cobalamin and collecting urine for 24 h and is dependent on normal renal and bladder function. • Urinary excretion of cobalamin will reflect cobalamin absorption provided that intrahepatic binding sites for cobalamin are fully occupied. • To ensure saturation of hepatic cobalamin binding sites so that all absorbed radiolabeled cobalamin will be excreted in urine, 1 mg cobalamin is administered intramuscularly 1 h following ingestion of the radiolabeled cobalamin. • The Schilling test may be abnormal (usually defined as 10% excretion in 24 h) in pernicious anemia, chronic pancreatitis, blind loop syndrome and ileal disease. Histologic Findings Depending on the cause, the histologic features of malabsorption vary. – A frequently encountered histologic finding is villous atrophy, which is seen in celiac disease, tropical sprue, viral gastroenteritis, bacterial overgrowth, inflammatory bowel disease, immunodeficiency syndromes, lymphoma and radiation enteritis. Caption: Small intestine. Fluorescence confocal light