The Movement of Fluid Across the Plasma Membrane
advertisement

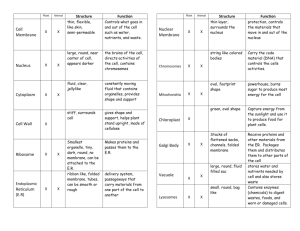
The Movement of Fluid Across the Plasma Membrane • Describe the role of aquaporins in water movement across membranes. • Define and explain osmotic and hydrostatic forces. • Calculate the osmotic pressure gradient. • Define and explain tonicity. • Discuss the effect of hypertonic, isotonic and hypotonic -solutions on cell volume. • Define non-penetrating, rapid penetrating and slow penetrating solute • Describe the effect of the administration of various IV fluids on the internal environment. The Movement of Water Across the Plasma Membrane •Water can move in and out of cells. •But the partition coefficient of water into lipids is low meaning the permeability of the membrane lipid bilayer for water is low. •Specific membrane proteins that function as water channels explain the rapid movement of water across the plasma membrane •These water channels are small integral membrane proteins known as aquaporins Water Movement NaCl 0 mOsm NaCl 100 mOsm [water] HIGH [water] LOW Aquaporin If membrane impermeable to NaCl CLINICAL CORRELATION•In the kidney, aquaporin-2 (AQP2) is abundant in the collecting duct and is the target of the hormone vasopressin, also known as antidiuretic hormone. This hormone increases water transport in the collecting duct by stimulating the insertion of AQP2 proteins into the apical plasma membrane. Several studies have shown that AQP2 has a critical role in inherited and acquired disorders of water reabsorption by the kidney. • For example, nephrogenic diabetes insipidus is a condition in which the kidney loses its ability to reabsorb water properly, resulting in excessive loss of water and excretion of a large volume of very dilute urine (polyuria). Although inherited forms of diabetes insipidus are relatively rare, it can develop in patients receiving chronic lithium therapy for psychiatric disorders, giving rise to the term lithium-induced polyuria. • Both of these conditions are associated with a decrease in the number of AQP2 proteins in the collecting ducts of the kidney. Osmosis - Osmosis is the flow of water across a semipermeable membrane from a solution with low solute concentration to a solution with high solute concentration. • The driving force for the movement of water across the plasma membrane is the difference in water concentration between the two sides of the membrane. • For historical reasons, this driving force is not called the chemical gradient of water but the difference in osmotic pressure. • The osmotic pressure of a solution is defined as the pressure necessary to stop the net movement of water across a selectively permeable membrane that separates the solution from pure water. The Movement of Water Across the Plasma Membrane Is Driven by Differences in Osmotic Pressure •Osmotic pressure of a solution is defined as the pressure necessary to stop the net movement of water across a selectively permeable membrane •When a membrane separates two solutions of different osmotic pressure, water will move from – the solution with low osmotic pressure (high water and low solute concentrations) to the solution of high osmotic pressure (low water and high solute concentrations). The osmotic pressure of a solution can be calculated by - Van't Hoffs law, which states that osmotic pressure depends on the concentration of osmotically active particles. The concentration of particles is converted to pressure according to the following equation: where: osmotic pressure (mm Hg or atm) g = number of particles in solution 7T = R = gas constant (0.082 L-atm/mol-K) σ = Reflection coefficient (varies from 0 to 1) T = absolute temperature (K) C = concentration (mol/L) Reflection coefficient (σ) • is a number between zero and one that describes the ease with which a solute permeates a membrane. • a. If the reflection coefficient is 1, the solute is impermeable. Therefore, it is retained in the original solution, it creates an osmotic pressure, and it causes water flow. Serum albumin (a large solute) has a reflection coefficient of nearly one. • b. If the reflection coefficient is 0, the solute is completely permeable. Therefore, it will not exert any osmotic effect, and it will not cause water flow. Urea (a small solute) has a reflection coefficient of close to zero and it is, therefore, an ineffective osmole Osmolarity refers to osmotic pressure generated by the dissolved solute molecules in 1L of solvent. It depends strictly on the number of particles in solution (not the number of molecules, since some molecules (e.g. NaCl) dissociate into ions when in solution). Osmolarity is therefore, the number of particles per liter of solution and is expressed in osmol/L or OsM or in the case of dilute solutions as milliosmol/L. Ex- A solution of 1 M CaC12 has a higher osmotic pressure than a solution of 1 M KCl because the concentration of particles is higher. The higher the osmotic pressure of a solution, the greater the water flow into it. Units of concentration • mOsm (milliosmolar) or mOsm/L = an index of the concentration of particles per liter of solution • mM (millimolar) or mM/L = an index of the concentration of molecules dissolved per liter of solution • isotonic solutions = 300 mOsm = 150 mM NaCl (one NaCl molecule yields two particles in solution) • 300 mOsm = 300 mM glucose Osmolality and Tonicity • A solution’s osmolality is determined by the total concentration of all the solutes present. • In contrast, the solution’s tonicity is determined by the concentrations of only those solutes that do not enter(“penetrate”) the cell Osmolarity • Two solutions having the same effective osmotic pressure are isotonic because no water flows across a semipermeable membrane separating them. • If two solutions separated by a semipermeable membrane have different effective osmotic pressures, the solution with the higher effective osmotic pressure is hypertonic and the solution with the lower effective osmotic pressure is hypotonic. • Water flows from the hypotonic to the hypertonic solution. RBC hypotonic solution Rules for predicting tonicity If the cell has a higher concentration of non-penetrating solutes than the solution, there will be net movement of water into the cell. The cell swells, and by definition that solution is hypotonic. SWELL RBC isotonic solution NO VOLUME CHANGE RBC hypertonic solution SHRINK Tonicity Tonicity describes the volume change of a cell placed in a solution Problems involving a non penetrating solute • Predict the changes in cell volume (increase, decrease, no change) when a normal RBC previously equilibrated in isotonic saline is placed in the following solutions. • Assume the fluid volume of the external solution is large, and thus, as water moves in or out of the cell, there is no significant change in the concentration of beaker solutes . 1. 200 mOsm NaCl 2. 400 mOsm NaCl 3. 150 mM NaCl 4. 300 mM NaCl Effect of substances that rapidly penetrate cell membranes • The presence of a substance, such as urea, ,5% dextrose that penetrates the cell membrane quickly does not affect the osmotic movement of water. • If the total concentration of non penetrating solutes is <300 mOsm, the RBC will swell; if it is >300 mOsm,the RBC will shrink. Problems involving a rapidly penetrating solute • Predict the changes in cell volume (increase, decrease, no change) when a normal RBC previously equilibrated in isotonic saline is placed in the following solutions: 1. 200 mOsm NaCl and 200 mOsm urea 2. 300 mOsm urea only 3. 500 mOsm urea only Effect of substances that slowly penetrate cell membranes • Some substances( glycerol) penetrate cell membranes but do so slowly. • Thus, they initially have an osmotic effect like sodium chloride but no osmotic effect at equilibrium. • Problem involving a slowly penetrating solute Q.Predict the changes in cell volume (increase, decrease, no change) when a normal RBC previously equilibrated in isotonic saline is then placed in the following solution. Determine the initial effect versus the longterm effect. • 200 mOsm NaCl and 200 mOsm glycerol (a slowly penetrating substance) The Clinical Relevance of Understanding Tonicity The importance of understanding this well is to make sure that you understand the basis and rationale for intravenous fluid therapy. Several IV fluids exist e.g. 0.9% saline(normal saline) 5% dextrose in normal saline 5% dextrose in water half normal saline 5% dextrose in half normal saline. (Dextrose is glucose). How does the clinician decide which fluid to use? Well, it depends on what the objectives are – replacement of blood volume or rehydration of cells in dehydrated individuals. Discussion on IV solutions First thing to do is to look at the relative osmolarity and tonicity of the solution to the extracellular (and intracellular) fluid. Then take into account what effect this will have on the volumes of the two fluid compartments. 1. 0.9% saline. This has the same osmolarity as the intracellular fluid. The saline is NaCl so the two particles Na and Cl are considered to be non-penetrating. Therefore this solution is isoosmotic and isotonic. Because it is isotonic it will not change the tonicity of the extracellular fluid and so the extracellular fluid will remain isotonic to the intracellular fluid. Therefore NO FLUID MOVEMENT INTO THE CELLS. This solution would be suitable for replacing blood (extracellular fluid). 2. 5% Dextrose in normal saline. 5% dextrose is iso-osmotic to the intracellular fluid, so is normal saline. Therefore you must take into account both of these when working out the overall osmolarity. This solution has twice the osmolarity of the intracellular fluid. Therefore it is HYPEROSMOTIC. Dextrose is penetrating , so makes no contribution to the tonicity of the solution. Saline is non-penetrating it does make a contribution. Therefore the solution is ISOTONIC. Infusion of this solution into the veins would not change the tonicity of the extracellular fluid so NO NET FLUID MOVEMENT INTO THE CELLS. Notice the NET. Rapid infusion of this solution will lead initially to some water movement out of the cells which will be reversed as the dextrose moves into the cells. This solution would be suitable for replacing blood. 3. 5% Dextrose in water. 5% dextrose is iso-osmotic to the intracellular fluid. Water is, of course, hypo-osmotic (0 mosm)(it has no particles). This solution therefore is iso-osmotic to the intracellular fluid. Water has no tonicity and dextrose is penetrating . This solution has no tonicity so is HYPOTONIC to the intracellular fluid. Infusion of this solution will make the extracellular fluid hypotonic to the intracellular fluid so some of the infused fluid will enter the cell. THERE IS THEREFORE FLUID MOVEMENT INTO THE CELLS. This solution would be suitable for rehydrating cells. 4. Half normal saline. This is 0.45% saline, so has half the number of particles as normal saline so it is hypo-osmotic to the intracellular fluid. The particles are non-penetrating but again you have half the number of particles. This solution is therefore HYPOTONIC to the intracellular fluid. Infusion of this solution will make the extracellular fluid hypotonic to the intracellular fluid so some of the infused fluid will enter the cell. THERE IS THEREFORE FLUID MOVEMENT INTO THE CELLS. This solution would be suitable for rehydrating cells. 5. 5% Dextrose in half normal saline. 5% dextrose is iso-osmotic to the intracellular fluid, half normal saline is hypo-osmotic. However if you have them together in a solution the result is hyperosmotic to the intracellular fluid. Only the saline is nonpenetrating , therefore the solution is HYPOTONIC to the intracellular fluid. Infusion of this fluid will decrease the tonicity of the extracellular fluid. THERE IS THEREFORE FLUID MOVEMENT INTO THE CELLS. This solution would be suitable for rehydrating cells. In order to replenish the fluid and electrolyte loss in diarrhoea, a person is given ORS. Of the following composition of ORS, which of the following along with Na is more important for replenishing Na loss? a. K b. Cl c. Glucose d. Citrate Oral Rehydration Therapy Is Driven by Solute Transport Oral administration of rehydration solutions has dramatically reduced the mortality resulting from cholera and other diseases that involve excessive losses of water and solutes from the gastrointestinal tract. The main ingredients of rehydration solutions are glucose, NaCl, and water. The glucose and Na+ ions are reabsorbed by SGLT1 and other transporters in the epithelial cells lining the lumen of the small intestine . Deposition of these solutes on the basolateral side of the epithelial cells increases the osmolarity in that region compared with the intestinal lumen and drives the osmotic absorption of water. Absorption of glucose, and the obligatory increases in absorption of NaCl and water, helps to compensate for excessive diarrheal losses of salt and water.