Clinical Research Professional Orientation

Clinical Research Professional Orientation
“Research Documentation"
Suzanne Swain Cabriales, MSN, OCN, CBCN, CCRP
Clinical Research Office
Samuel Oschin Comprehensive Cancer Institute
Cancer Drug Approval Process
(Friends of Cancer Research; 2013, www.focr.org)
EDIT ALL FOOTERS WITH VIEW>HEADER AND FOOTER... 2
The Economics of Drug Development
(Cancer Information &Support Network, 2013; cisncacner.org)
3
Introduction
• Clinical Trials are controlled experiments run in an uncontrolled environment
• Source documents are the ‘field notes’ establishing study conduct
The Economics of Drug Development
(Cancer Information &Support Network, 2013; cisncacner.org)
Another potential solution to the drug logjam is to run adaptive clinical trials, where the criteria for success would be adjusted as results come in.
Based on early responses, doctors might recruit different types of patients midway through a trial.
EDIT ALL FOOTERS WITH VIEW>HEADER AND FOOTER... 5
What is the purpose of Source Documentation?
Accurate Documentation Supports the
Fundamental Principle of Protecting
Subject’s Rights, Safety and Well Being
FDA Guidance: Investigator Responsibilities-protecting the rights, Safety, and Welfare of Study Subjects
• Guidance states:
“The investigator should develop a plan for the supervision and oversight of the clinical trial at the site. Supervision and oversight should be provided even for individuals who are highly qualified and experienced. A plan might include the following elements:
Routine meetings with staff to review trial progress, adverse events and update staff on any protocol changes
Routine meetings with the sponsor’s monitors
A procedure for timely correction and documentation of problems identified by study personnel
A PROCEDURE FOR ENSURING THAT SOURCE DATA ARE
ACCURATE, CONTEMPORANEOUS, AND ORIGINAL
A PROCEDURE FOR ENSURING THAT INFORMATION IN SOURCE
DOCUMENTS IS ACCURATELY CAPTURED ON THE CRF
EDIT ALL FOOTERS WITH VIEW>HEADER AND FOOTER... 7
Why is Source Documentation so Important?
21CFR Parts 16,58,71,101,170,171,190,312,511,571, and 812
• Sponsors are required to report information indicating that any person has, or may have, engaged in the falsification of data in the course of reporting study results, or in the course of proposing, designing performing, RECORDING, supervising, or reviewing studies……
• Falsification of data means creating, altering, recording or OMITTING data in such a way that the data do not represent what actually occurred..
• ..
These reporting requirements would apply to information related to studies including but not limited to, clinical investigations, nonclinical laboratory studies, and clinical studies in animals
EDIT ALL FOOTERS WITH VIEW>HEADER AND FOOTER... 8
Rule #1: Data is King
Data reported on the CRF, which are derived from source documents, should be consistent with the source documents or the discrepancies should be explained
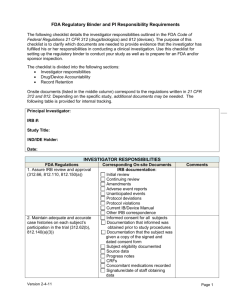
What is Clinical Trial Documentation?
Any document, form, or record where specific participants’ data is first recorded: ICH guidelines define source documents as original documents, data and records.
FDA (21 CFR 312.2 (b)) requires that the investigator prepare and maintain accurate case histories designed to record all observations and other data pertinent to the investigation on each individual treated with the investigational drug or employed as a control in the investigation”.
Clinical Trials
Clinical trials are controlled experiments conducted in uncontrolled environments
Our job is to exert quality control measures and adhere to protocol
Our job is to ensure subject safety
Our job is to ensure data integrity
Documentation of the course of events establishes the facts
Source documentation ensures that the subject’s welfare was respected
Source Documentation
Source documents include:
Inpatient and outpatient medical records
Progress notes
Consults
Nursing/Physician Assistant’s notes
Pathology
Radiology reports
Medication/radiation administration record
Surgical / procedural reports
Laboratory reports
Admission forms
Flow sheets that are initialed/signed and dated
Quality of life or other surveys
Participant/subject diaries/calendars
Documentation Standards
All research personnel must comply with applicable standards for medical documentation as determined by their institutional policy, professional Code of Ethics, and licensing authority
At a minimum, the following general standards must be followed:
1. Keep handwritten notes and signatures legible (if necessary, print name underneath the signature).
2. Sign and date all entries. Include credentials if required by the institution.
3. Make error corrections in the following manner: draw a single line through the incorrect information, initial, date, and state reason for change (if necessary).
4. Never obliterate entries that require correction.
5. Never destroy original documents if they require error correction
Documentation Standards Continued
6. Keep subject records secure yet accessible
7. Do not alter past-dated notes, chart notes/progress notes (e.g., by writing alongside or adding to prior entries)
8. Only use dark ink.
9. Never use whiteout
10. Never use pencils
11. Hospital records used to substantiate data must meet institutional policy and are not held to GCP standards as are research records
12. Records should be maintained chronologically
US FDA Guidance- ALCOA
ALCOA documentation- adapted by the World
Health Organization
A – Attributable, you can tell who wrote the note
L – LEGIBLE- including signatures
C – Contemporaneous – REAL TIME DATA COLLECTION
O – Original – first place the data is captured (shouldn’t be on a sticky note)
A – Accurate – consistent and real representation of the facts
Additionally
Enduring – long-lasting and durable
Available and accessible, complete, consistent
Credible – based on real and reliable facts
Purpose of Source Documents
Provide original documents, “raw” data and records
Document existence of the subject
Substantiate compliance with the protocol and integrity of the study data
Serve as audit trail = recreate the progression of clinical trial
Rule #2: Please do not make up the data
If it was not documented in the patient’s medical record, it was not done or never happened!!!!!
Documentation Don’ts
Don’t leave any space between the last entry and your signature
Do not chart in advance
Backdate, tamper with ,erase, or add to previously written notes
Skip lines between entries
Do no use slang
Do not use medical terms unless their meaning in known
Do not chart for anyone else
Do not use correction fluid
Do not spell words incorrectly
Research Documentation Elements
Informed consent process
Verification of Eligibility
Past medical history – obtain primary source
Prior therapies- obtain primary source
Concomitant Medications – start/stop dates, indication, dosage, frequency
Protocol related visits, procedures, exams
Results of study required scans/tests (e.g. RECIST)
Study drug administration
Subject medication diaries
Adverse events/Serious adverse events
Unscheduled visits
Off treatment; why, date, investigator decision and signature
Off Study: date and reason
Follow up
Medical Record vs. Research Record
Medical Record
The collection of information concerning a patient and his or her health care.
Each medical record shall contain sufficient, accurate information to identify the patient, support the diagnosis, justify the treatment, document the course and results, and promote continuity of care among health care providers. The information may be from any source and in any format, including, but not limited to print medium, audio/visual recording, and/or electronic display.
Also known as the “Legal Medical Record” or “LMR” in that it serves as the documentation of the healthcare services provided to a patient by a hospital, clinic, physician or provider.
Research Record (aka: “Shadow Chart”)
Typically refers to copies of a subjects’ medical record that is maintained by study staff.
Contains all clinical information related to the subjects’ care during the research protocol and additional research records that may not be filed in the subjects’ medical record.
The documents contained within these files are NOT considered original source documents, as they are copies. Monitors and FDA auditors may require the original documents or certified copies during site visits or inspections.
FDA Audits
FDA conducts both announced and unannounced inspections of clinical investigator sites, typically under the following circumstances:
to verify the accuracy and reliability of data that has been submitted to the agency ; as a result of a complaint to the agency about the conduct of the study at a particular investigational site;
in response to sponsor concerns; upon termination of the clinical site;
during ongoing clinical trials to provide real-time assessment of the investigator’s conduct of the trial and protection of human subjects; at the request of an FDA review division; and
related to certain classes of investigational products that FDA has identified as products of special interest in its current work plan (i.e., targeted inspections based on current public health concerns).
FDA Audits continued
whether authority to conduct aspects of the study was delegated, and if so, how the conduct of the study was supervised by the clinical investigator ;
where specific aspects of the investigation were performed;
how the study data were obtained and where the study data were recorded ; accountability for the investigational product, including shipping records and disposition of unused investigational product; whether the clinical investigator disclosed information regarding his financial interests to the sponsor and/or interests of any subinvestigator(s), spouse(s) and dependent children;
the monitor’s communications with the clinical investigator; the monitor’s evaluations of the progress of the investigation; and
corrective actions in response to previous FDA inspections, if any, and regulatory correspondence or sponsor and/or monitor correspondence
FDA Audits continued
During an inspection at the site of a clinical investigator, the FDA investigator typically verifies compliance with the regulations governing the use of investigational products and human subject protections at 21 CFR parts 50, 56,
312, and/or 812, by inspecting records and talking to individuals involved in the conduct of the study to ascertain:
who performed various aspects of the protocol for the study (e.g., who verified inclusion and exclusion criteria, who obtained informed consent, who collected adverse event data);
whether the IRB approved the protocol, informed consent form, and any amendments to the protocol prior to implementation;
whether the clinical investigator and study staff adhered to the sponsor’s protocol and investigational plan and whether protocol deviations were documented and reported appropriately ; whether informed consent documents were signed by the subject or the subjects’ legally- authorized representative prior to entry in the study (i.e., performance of any study- related procedures);
Informed Consent and Eligibility Verification
Informed consent process
Note stating that the process occurred and that the subject received a signed copy
Verification of eligibility
Note stating that subject meets all inclusion criteria and has no exclusionary criteria
All results for labs, pathology and any other procedures that are required to confirm eligibility should be in the appropriate section of the medical record (paper or electronic)
Past medical hx/prior therapies
Summary from initial H & P, or more recent one
Outside records that confirm prior cancer therapies, pathology reports, etc. are to be placed in the medical record
Concomitant Medications
All con meds that the patient has been taking, generally for 30 days prior to enrolling, need to be in the medical record including:
Dates taken – both when started and when stopped or dosage changed
Month and Year is acceptable for con meds taken before enrollment to study
Day, month, year is to be noted once patient has begun treatment on study
Reason/indication
Some meds are given for indications not approved by the FDA, so you can’t assume that the patient is taking them for the condition indicated in the package insert. This is referred to as off label use.
Dosage/Amount with unit of measure (i.e., mg, tab)
Frequency
Protocol Visit Records
All protocol related visits, procedures, exams, etc. need to be noted in the medical record that they occurred:
Document occurrence, results, who conducted and any follow- up.
Some of the information may be on the final report.
Protocol-specific info (i.e., PKs drawn, biopsy obtained)
If a scheduled visit is missed, this also needs to be noted including the reason and then any follow-up that needs to occur (i.e., Day 8 labs missed by patient and arrangements made to be drawn on Day 10 instead)
End of Treatment
When subject is taken off active treatment, a note needs to be written including why and the date
The date is the date when the MD/ Investigator decides that no further therapy will be given
This may be the same as the date of a scan or the last dose of drug, but not always
Patient Correspondence
Telephone Calls
Document reason for call (adverse event, general question, test result, etc.)
Document outcome of call (how adverse event to be treated, etc.)
111
End of Study
Off Study
Off-treatment note:
Document reason off-treatment, including date
Document any follow-up that needs to occur
Document return of drugs, if applicable
Note any ongoing AEs and continue to follow if related to study
Follow-up note:
Review and document all protocol-specific activities that occur in the follow-up period. This may include survival alone or in combination with: adverse events (new and/or unresolved), concomitant meds, tests/procedures conducted, disease/response and/or research labs
Off-study note:
Document reason off-study, including date
FDA Warning Letter
You failed to maintain adequate and accurate case histories that record all observations and other data pertinent to the investigation on each individual administered the investigational drug or employed as a control in the investigation [21 CFR
312.62(b)].
a. The Cycle 3 (11/22/08) Case Report Form (CRF) for Subject 4065381 documented the adverse event of Nail Change, yet no evidence was available in the source documents to support the event’s occurrence.
b. All three study subjects had Case Report Forms (CRFs) in which the doses of (b)(4) bolus and (b)(4) infusion values were transposed. The value for (b)(4) infusion dose was incorrectly recorded in the (b)(4) bolus dose box, and the value for (b)(4) bolus was incorrectly recorded in the (b)(4) infusion.
Furthermore, the (b)(4) bolus, which was recorded in the infusion box, was incorrectly converted from milligrams to grams. We also note that the dosing for (b)(4), as noted in the source documents, is inconsistent with what was reported in the CRFs for the subjects and cycles, as noted in the table below.
Failing to maintain adequate and accurate case histories compromises the interpretation and validity of the clinical investigational endpoints.
FDA Warning Letter continued
An investigator is required to prepare and maintain adequate and accurate case histories that record all observations and other data pertinent to the investigation on each individual administered the investigational drug or employed as a control in the investigation.
a. According to the protocol, after reviewing a subject’s international normalized ratio (INR) value, the investigator was to make the final dosing decision. You failed to maintain adequate and accurate case histories that recorded your dosing decisions for the drugs administered during the course of this investigation. Examples of this failure include, but are not limited to, the following:
The only documentation of dosing decisions for subjects was the unsigned “face sheets” filled out by the study coordinator. Our review of the face sheets for Subjects 03461, 07600,
12285, 14055, 16496, 16666, 20418, and 20544 found no documentation that you ordered the study drug dose to be maintained, withheld, or adjusted, or that you confirmed that the drug dosing decisions recorded by the study coordinator were in line with your orders .
Both you and the study coordinator stated that your site’s process for relaying dosage information was as follows: The study coordinator would communicate blinded INR results to you, either verbally or via text messages, and you would tell the study coordinator to maintain, withhold, or adjust the current dose. The study coordinator would then issue dosing instructions and order drug supplies as needed, according to your verbal orders. Our investigation found that these unsigned face sheets served as the only documentation of the dosing decisions for subjects. As a result, there was no way to confirm that the drug dosing decisions recorded by the study coordinator were in line with your orders.
FDA Warning Statement
Failure to maintain adequate and accurate case histories compromises the interpretation and validity of the investigational endpoints.
Conclusion
“Ultimately, the source document should speak for itself. It should narrate the medical journey of the patient as it happened, to an independent observer, an auditor, or an inspector and thus form a strong foundation for a good clinical research.”
Bargaje, 2011
References
1. Bargaje, C. (2011). Good documentation practice in clinical research. Perspectives in Clinical Research, Apr-Jun; 2(2): 59-
63.
2. Documentation 101: Center for Cancer Research, NCI
3. Klimaszewski, et al, (2008). Manual for Clinical Trials Nursing,
2nd Ed.
4. 45CFR46, Subpart D
5. 21CFR50,56
6. FDA Guidance, FDA guidance for IRS and Investigators
7. FDA Guidance, E6 Good Clinical Practice
8. Kord, D., Ehringhous, S. (2006) Principles for Strengthening the integrity of Clinical Research. Public Library of Science clinTrial 1(1).