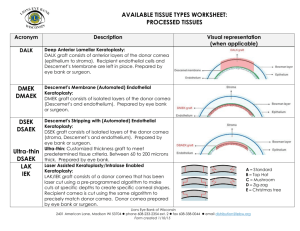
Big-Bubble Deep Anterior Lamellar Keratoplasty Dissection Plane

Big-Bubble Deep Anterior Lamellar
Keratoplasty Dissection Plane
Hamish D. McKee, MB ChB
Luciane C. D. Irion, PhD, FRCPath
Fiona M. Carley, FRCOphth
Arun K. Brahma, MD, FRCOphth
Manchester Royal Eye Hospital, United Kingdom
Corneal Transplantation
• Penetrating Keratoplasty
– Femtosecond-assisted
• Anterior Lamellar Keratoplasty
– Deep Anterior Lamellar Keratoplasty (DALK)
– Anterior Lamellar Keratoplasty (ALK)
– Femtosecond-assisted
• Endothelial Keratoplasty
– Descemet’s Stripping Automated Endothelial
Keratoplasty (DSAEK)
– Descemet’s Membrane Endothelial Keratoplasty
(DMEK)
• Keratoprosthesis
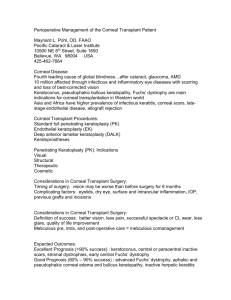
Descemet’s Membrane
8 week stage in utero endothelial cells secrete
DM continuously
A = banded DM prior to birth 3 micrometre
B = unbanded DM post-birth up to 7 micrometre
Stroma
• 80-85% of structure of cornea
• Deeper layers more strictly organised than superficial layers
• Anterior cornea is more rigid
• Posterior cornea has poor rigidity
– During stromal swelling pressure directs against
DM
– Results in Descemet’s Folds
DALK
• Video
• Several techniques for anterior lamellar removal
• big bubble technique (Anwar)
– Surgically technically challenging
– Best method of ‘baring’ Descemet’s membrane
• Sugito and Kondo hydrodelamination technique
• Melles technique of manual dissection
• Rostron’s direct dissection method
Why not do PK for everyone?
• Less invasive the procedure, the better
• Avoid removing non-diseased, healthy tissue
• Remove only the part of the cornea that is dysfunctional
• Avoid open-sky situations
Background
• Assumed that big-bubble DALK dissection plane is between stroma and Descemet membrane (DM)
Anwar M, Teichmann KD.
Big-bubble technique to bare Descemet's membrane in anterior lamellar keratoplasty.
J Cataract Refract Surg 2002;28:398-403.
• Study of 3 big-bubble posterior lamellae obtained during conversion to PK showed residual stroma on all 3
Jafarinasab MR, Rahmati-Kamel M, Kanavi MR, et al.
Dissection Plane in Deep Anterior Lamellar Keratoplasty Using the Big-Bubble Technique.
Cornea 2010 Feb 15.
Background
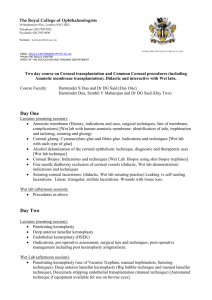
• 2 types of big bubble seen clinically
• White-margin big-bubble
– As described in original paper
Anwar M, Teichmann KD.
Big-bubble technique to bare Descemet's membrane in anterior lamellar keratoplasty.
J Cataract Refract Surg 2002;28:398-403.
• Clear-margin big-bubble
– Appears like air-bubble in AC but not mobile
– Anwar suggested may represent intra-DM cleavage plane (AAO
Subspeciality Day November 10,
2007)
Edge of mobile air bubble in AC
Aims and methods
• Donor corneas mounted on artificial anterior chamber
• Big-bubble dissection carried out
• Type of bubble noted
– White-margin
– Clear-margin
• Samples, formalin-fixed paraffin-embedded, evaluated with light microscopy using H&E and PAS stain
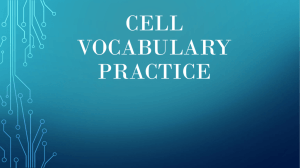
Results
• 30 white-margin big-bubbles
– All showed residual stroma
Mean 7.0 μm (range 2.6 – 17.4)
• 2 clear-margin big-bubbles
– No residual stroma seen on
Descemet membrane
• Unable to determine on light microscopy if plane between
DM and stroma or intra-DM
Stroma (S), Descemet membrane (D), endothelium (E)
Conclusion
• The big bubble technique does NOT routinely bare DM
• The white margin seen during big-bubble DALK may indicate an intrastromal cleavage plane
• True baring of DM may only occur in the less commonly seen clear-margin big-bubble
• The disregulation of lamellar fibres within the stroma of keratoconus may explain why the big bubble is a surgically difficult procedure with relatively low success
• It is important to note the type of big-bubble obtained clinically for histological or clinical research on bigbubble DALK