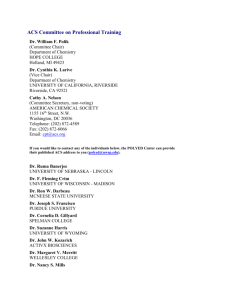
Welcome Cara Bilinsky ACCELMED Logistical Information Track Number: • Track 1 = Red travel packet • Track 2 = Blue travel packet Departure: • Departure city = city on ID Rotation: • You will rotate sessions every 25 minutes • 5-minute transition time between sessions Logistical Information (cont’d) Passport: • Refer to your passport for the program slides, faculty bios, and credit information Brochures: • 3 sessions have handouts for additional information Stations: • Please stay with your assigned travel group • After the 3 sessions, we will reconvene for the conclusion Logistical Information (cont’d) Pre/Postsurvey: • Located in the center of your travel packet • Complete the presurvey prior to the first session • After the last session, complete the postsurvey Evaluation Form: • Located in the center of your travel packet • Turn in at the registration tables as you leave Credit: • Complete the information on the Evaluation Form, and your certificate will be issued by mail Welcome and Overview Deepak L. Bhatt, MD, MPH, FACC, FAHA, FSCAI, FESC Professor of Medicine, Harvard Medical School Chief of Cardiology, VA Boston Healthcare System Director, Integrated Interventional Cardiovascular Program Brigham and Women's Hospital and VA Boston Healthcare System Senior Investigator, TIMI Study Group Boston, Massachusetts Accreditation and Funding Jointly sponsored by the Postgraduate Institute for Medicine (PIM) and ACCELMED. This activity is supported by an educational grant from Daiichi Sankyo, CO., LTD., and Lilly USA, LLC. This educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the FDA. PIM, ACCELMED, Daiichi Sankyo CO., LTD., and Lilly USA, LLC do not recommend the use of any agent outside of the labeled indications. The opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of PIM, ACCELMED, Daiichi Sankyo CO., LTD. and Lilly USA, LLC. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications, and warnings. Accreditation and Funding (cont’d) Physician Continuing Medical Education Accreditation Statement This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Postgraduate Institute for Medicine and ACCELMED. The Postgraduate Institute for Medicine is accredited by the ACCME to provide continuing medical education for physicians. Credit Designation The Postgraduate Institute for Medicine designates this live activity for a maximum of 2.0 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. Faculty Disclosures The faculty reported the following financial relationships or relationships to products or devices they or their spouse/life partner have with commercial interests related to the content of this CME activity: Name of Faculty/Presenter Deepak L. Bhatt, MD, MPH, FACC, FAHA, FSCAI, FESC Activity Chair Reported Financial Relationship Contracted Research: Amarin Corp.; AstraZeneca; Bristol-Myers Squibb Company; Eisai, Inc.; Ethicon, Inc.; Medtronic; sanofi-aventis; The Medicines Company Dominick J. Angiolillo, MD, PhD, FACC, FESC, Consulting Fees: Abbott Vascular; Accumetrics; Arena Pharmaceuticals, Inc.; FSCAI AstraZeneca; Bristol-Myers Squibb Company/sanofi-aventis; Daiichi Sankyo, CO., LTD./Lilly USA, LLC; Evolva; Medicure, Inc.; Merck & Co., Inc.; Novartis International AG; Portola Pharmaceuticals, Inc.; The Medicines Company Contracted Research: Boston Scientific; Bristol-Myers Squibb Company/sanofi-aventis; Daiichi Sankyo, CO., LTD./Lilly USA, LLC; GlaxoSmithKline; Otsuka America, Inc. Speakers’ Bureaus: Abbott Vascular; AstraZeneca; Bristol-Myers Squibb Company/sanofi-aventis; Daiichi Sankyo, CO., LTD./Lilly USA, LLC Faculty Disclosures (cont’d) Name of Faculty/Presenter Reported Financial Relationship Paul A. Gurbel, MD Consulting Fees: Accumetrics; AstraZeneca; Bayer Healthcare Pharmaceuticals; Boehringer Ingelheim GmbH; CSL Limited; Daiichi Sankyo, CO., LTD./Lilly USA, LLC; Iverson Genetics Diagnostics, Inc.; Haemonetics Corporation; Medtronic; Merck & Co., Inc.; Nanosphere, Inc.; Novartis International AG; POZEN, Inc.; sanofi-aventis Patents: Personalized antiplatelet therapy and interventional cardiology Contracted Research: AstraZeneca; CSL Limited; Daiichi Sankyo, CO., LTD./Lilly USA, LLC; Duke Clinical Research Institute; Haemoscope; Harvard; Medtronic; National Institutes of Health; POZEN, Inc.; sanofi-aventis Speakers’ Bureaus: Daiichi Sankyo, CO., LTD./Lilly USA, LLC; Iverson Genetics Diagnostics, Inc.; Merck & Co., Inc.; Nanosphere, Inc.; sanofi-aventis Gilles Montalescot, MD, PhD Consulting Fees: Abbott Vascular; AstraZeneca; Bayer Healthcare Pharmaceuticals; Biotronik; Boehringer Ingelheim GmbH; Daiichi Sankyo, CO., LTD.; GlaxoSmithKline; Lilly USA, LLC; Iroko Pharmaceuticals, LLC; The Menarini Group; MSD India; Nanosphere, Inc.; Novartis International AG; Pfizer, Inc.; Portola Pharmaceuticals, Inc.; Roche Diagnostics; sanofi-aventis; The Medicines Company Contracted Research: AstraZeneca; Biotronik; Bristol-Myers Squibb Company; Boston Scientific; Brahms; Daiichi Sankyo, CO., LTD; GlaxoSmithKline; Lilly USA, LLC; Medtronic; Nanosphere, Inc.; Pfizer, Inc.; Roche Diagnostics; sanofi-aventis; Spartan Bioscience, Inc.; Stago; STENTYS SA Faculty Disclosures (cont’d) Name of Faculty/Presenter Reported Financial Relationship E. Magnus Ohman, MD, FRCPI, FESC, FACC, FSCAI Consulting Fees: AstraZeneca; Boehringer Ingelheim GmbH; Bristol-Myers Squibb Company; Gilead Sciences, Inc.; Janssen Global Services, LLC.; LipoScience, Inc.; Merck & Co., Inc.; POZEN, Inc.; Roche Diagnostics; sanofiaventis; The Medicines Company; WebMD Contracted Research: Daiichi Sankyo, CO., LTD./Lilly USA, LLC P. Gabriel Steg, MD Consulting Fees: Amarin Corp.; Astellas; AstraZeneca; Bayer Healthcare Pharmaceuticals; Boehringer Ingelheim GmbH; Bristol-Myers Squibb Company/sanofi-aventis; Daiichi Sankyo, CO., LTD./Lilly USA, LLC; GlaxoSmithKline; Iroko Pharmaceuticals, LLC; Medtronic; MSD India; Novartis International AG; Otsuka America, Inc.; Pfizer, Inc.; Roche Diagnostics; sanofiaventis; Servier; The Medicines Company Contracted Research: NYU School of Medicine; sanofi-aventis; Servier Ownership Interest: Aterovax Learning Objectives After completing this activity, the participant should be better able to: 1. Incorporate antiplatelet therapies at an optimal dose to maximize benefit and minimize adverse events in the treatment of patients with ACS 2. Evaluate the role of genetic testing and potential drug-drug interactions on the choice of antiplatelet therapy 3. Appraise the current evidence on platelet function testing in choosing or altering antiplatelet therapy appropriately in patients Agenda Please join us in your assigned track. 2000 1500 1000 500 0 ACS MI UA Incidence Rate (# of cases/100,000 person-yr) Number of Hospitalizations (x 1000) Trend in Hospitalizations for ACS, MI, and UA Age- and Sex-adjusted Incidence Rates of AMI, 1999-2008 300 250 ][ ][ ][ ][ 200 150 100 50 ][ ][ ][ ][ ][ ][ ][ ][ ][ ][ ][ ][ ][ ][ ][ ][ ][ MI ][ ][ ][ ][ NSTEMI STEMI ][ ][ ][ ][ ][ 0 ACS = acute coronary syndromes. AMI = acute myocardial infarction. MI = myocardial infarction. NSTEMI = non-ST elevation myocardial infarction. STEMI = ST elevation myocardial infarction. UA = unstable angina. Error bars represent 95% confidence intervals. Based on ICD-9 Code Data from Kaiser Permanente Northern California Patient Database. American Heart Association. Heart Disease and Stroke Statistics – 2005 Update. Available at: http://www.americanheart.org/downloadable/heart/1105390918119HDSStats2005Update.pdf. Thom T, et al. Circulation. 2006;113:e85-e151. Rosamond W, et al. Circulation. 2007;115:e69-e171. Rosamond W, et al. Circulation. 2008;117:e25-e146. Lloyd-Jones D, et al. Circulation. 2009;119:e21-e181. Lloyd-Jones D, et al. Circulation. 2010;121:e46e215. Roger VL, et al. Circulation. 2011;123:e18-e209. Roger VL, et al. Circulation. 2011;123:e18-e209. Yeh RW, et al. N Engl J Med. 2010;362:2155-2165. PCI is Inherently Thrombogenic vWF, Tissue Factor Thrombin Generation • Indirect thrombin inhibitors: – Unfractionated heparin – LMWH • Direct thrombin inhibitors: – Bivalirudin Collagen Exposed Platelet Activation • Aspirin • P2Y12 inhibitors • GP IIb/IIIa inhibitor GP = glycoprotein. LMWH = low-molecular weight heparin. PCI = percutaneous coronary intervention. vWF = von Willebrand factor. Antiplatelet Agents ADP = adenosine diphosphate. PAR = protease-activated receptor. TxA2 = thromboxane A2. Desai NR, Bhatt DL. JACC Cardiovasc Interv. 2010;3:571-583. Clinically Relevant Dilemmas that We Face in Managing Patients with ACS • Optimal Dose of Oral Antiplatelet Therapies: – What is the optimal dose of aspirin for patients with ACS? – Is there an optimal dose of clopidogrel in ACS and should that vary in patients after PCI? – What is the optimal management strategy for medically managed patients? – What is optimal dose of prasugrel, especially in patients <60 kg and older patients >75 years of age to decrease bleeding risk? – Does the dose of aspirin play a role in patients treated with ticagrelor? Clinically Relevant Dilemmas that We Face in Managing Patients with ACS (cont’d) • Role of Platelet Function Testing in Choosing/altering Antiplatelet Therapies: – It has been well established that there is more variability in response to clopidogrel than with the more potent agents prasugrel and ticagrelor – Recent evidence indicates that on-treatment platelet aggregation predicts future risk of stent thrombosis or MACE – Recent evidence also shows that increasing the loading or maintenance dose of clopidogrel in hyporesponders improves platelet response – Is there evidence to support routine platelet function testing? MACE = major adverse cardiovascular event. Clinically Relevant Dilemmas that We Face in Managing Patients with ACS (cont’d) • Genetic Testing – It has been well established that a family of cytochrome P450 enzymes metabolizes clopidogrel to its active form – Recent evidence shows that patients who are treated with clopidogrel and are carriers of loss-of-function CYP2C19 polymorphism have an increased CV risk that led to an FDA warning – Are there other polymorphisms besides CYP2C19 that need to be tested? – Is there evidence that warrants routine genetic testing? CV = Cardiovascular. FDA = US Food and Drug Administration. Clinically Relevant Dilemmas that We Face in Managing Patients with ACS (cont’d) • Potential Drug-drug Interaction: – Ex vivo evidence using platelet function testing has shown that PPIs decrease the efficacy of clopidogrel – Registry analysis has shown that use of PPIs in patients on clopidogrel increases their risk of future events – Retrospective analyses of randomized trials has failed to show that PPIs adversely affect the efficacy of clopidogrel – A randomized prospective trial has shown that PPIs do not adversely affect the efficacy of clopidogrel. The result has also shown that PPI use provides better GI protection – Should PPIs be used routinely in patients on clopidogrel or on more potent antiplatelet agents? GI = gastrointestinal. PPI = proton pump inhibitor. Conclusions: Optimal Dose of Antiplatelet Agents • Evidence shows that low-dose aspirin seems to be as efficacious as high-dose aspirin, with lower risk of GI bleeding and no difference in major bleeding in PCI as well as non-PCI patients with ACS • Evidence shows that high-dose clopidogrel is not beneficial in all patients with ACS. However, it seems to be more efficacious in lowering the risk of CV death/MI/stroke in patient with ACS undergoing PCI, although the bleeding risk is also increased • Prasugrel does not have a role in medical management of ACS, though it does in patients with ACS undergoing PCI; when used, 5 mg should be considered in the underweight and the elderly • Patients with ACS managed invasively or medically on ticagrelor should receive low-dose aspirin Conclusions: Platelet Function Testing, Genetic Testing, and PPI Interaction • Current guidelines do not recommend routine platelet function testing • Current guidelines do not recommend routine genetic testing • Current guidelines do not recommend routine use of PPIs; however, use of PPIs in patients with high risk of GI bleeding is advised Thank You! Pease turn in your survey and evaluation as you depart.
 0
0
advertisement





Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users