Click here to Accident Injury form
advertisement

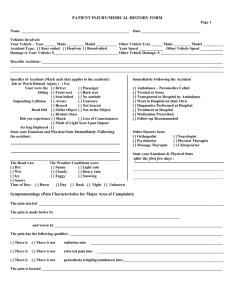
ACCIDENTAL INJURY REPORT If your clinic visit is due to an accident, please describe all events associated with it. DATE OF ACCIDENT _____________________________________ HOUR OF ACCIDENT ________________________ AM / PM TYPE OF ACCIDENT : WORK RELATED TRAFFIC OTHER WORK RELATED ACCIDENT EMPLOYER ____________________________________________ TYPE OF BUSINESS____________________________________ WAS ANY EQUIPMENT, MACHINERY AND/OR OBJECT RELATED TO ACCIDENT? WHAT KIND? ____________________ WAS ACCIDENT REPORTED TO SUPERVISOR AND/OR EMPLOYER? HAS A WOKER’S COMPENSATION CLAIM BEEN FILED? YES NO YES NO TRAFFIC ACCIDENT WHAT KIND OF VEHICLE WAS INVOLVED IN ACCIDENT? WERE YOU A DRIVER PASSENGER TRUCK CAR MOTORCYCLE OTHER PEDESTRIAN? IF A PASSENGER, PLEASE INDICATE YOUR LOCATION IN THE CAR _______________________________________________ YES NO MPH? ________________________ WAS YOUR VEHICLE MOVING WHEN THE ACCIDENT OCCURRED? DID YOUR VEHICLE HIT OTHER VEHICLE/S YES NO WHERE? ___________________________________________ DID OTHER VEHICLE/S HIT YOUR VEHICLE? YES NO WHERE? WAS ACCIDENT REPORTED TO POLICE DEPARTMENT? WERE TRAFFIC CITATIONS ISSUED? YES NO YES ___________________________________________ NO TO WHOM?_________________________________________________ WHERE DID ACCIDENT OCCUR ? ______________________________________________________________________________ DESCRIBE ACCIDENT INCLUDING CAUSE/S AND SURROUNDING CIRCUMSTANCES ______________________________ ______________________________________________________________________________________________________________ ______________________________________________________________________________________________________________ PRESENT COMPLAINT PROLONGED CAR RIDING FACE PALE LOSS OF SMELL PINS & NEEDELS IN ARMS/LEGS DIZZINESS DEPRESSION ANXIETY EYES SENSITIVE TO LIGHT NECK MOTION RESTRICTED HEAD SEEMS TOO HEAVY EXCESS PERSPIRATON SINUS TROUBLE NUMBNESS IN FINGERS, ARMS, LEGS FAINTING SWOLLEN ______ EXTREME FATIGUE EYES LOSS OF FOCUS UPPER BACK PAIN/STIFFNESS HEAD & SHOULDERS TIRED & HEAVY DIGESTIVE DISORDERS TREMORS EXTREME CHEST PAIN DOUBLE VISION NERVOUSNESS INSOMNIA NAUSEA, VOMITING FEET/HANDS MENTAL DULLNESS PALPITATION COLD SHORTNESS OF BREATH EARS BUZZING/RINGING MID BACK PAIN/STIFFNESS NEURITIS DIARRHEA TENSION LOSS OF MEMORY NECK PAIN DIFFICULTY IN EYE STRAIN LOSS OF TASTE LOW BACK PAIN/STIFFNESS FACE FLUSHED CONSTIPATION IRRITABLIT EQUILIBRIUM PROBLEMS NECK STIFFNESS PAIN BEHIND EYES DIFFICULTY IN EXCESSIVE STANDING WALKING RIDING BENDING NECK, LOW BACK PAIN & STIFFNESS UOPN RISING PAIN RADIATING INTO RIGHT ARM RIGHT LEG BOTH LEFT LEG LEFT ARM BOTH DIFFICUILTY IN EXCESSIVE LIFTING LIGHT MODERATE HEAVY REPETITIVE PAIN RADIATING INTO NECK BASE OF SKULL SHOULDER ARMS HIPS LEGS DID YOU REQUIRE POST-ACCIDENT HOSPITALIZATION YES NO IF SO, WHERE?____________________ HAVE YOU HAD SIMILAR ACCIDENTS OR INJURIES BEFORE? YES NO SYMPTOMS OTHER THAN ABOVE ______________________________________________________________________ ______________________________________________________________________________________________________ INSURANCE COMPANIES INVOLVED PARTY RESPONSIBLE FOR PAYMENT _________________________ CLAIM # _________________________________ HAVE YOU BEEN CONTACTED BY AN INSURANCE ADJUSTER OR COMPANY REPERSENTATIVE ABOUT CLAIM? ____________________________________________________ HAS YOUR ATTORNEY ADVISED YOU IN THIS CASE YES NO ATTORNEY’S NAME, ADDRESS & TELEPHONE # _________________________________________________________ PATIENT’S SIGNATURE ______________________________________________________ DATE ____________________