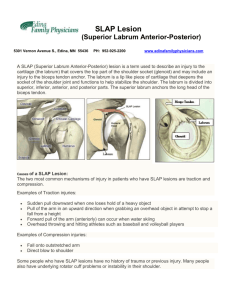
Labral Tears - Manchester University
advertisement

Brett Gemlick, MD SportONE Review Shoulder Anatomy Describe types of labral injuries Review Surgical Techniques Discuss post operative rehabilitation Return to play Clavicle • 1st bone to ossify, last to fuse (25 y) • SC joint only true joint connecting UE to axial skeleton Scapula • GH: greatest ROM of all joints golf ball on a tee, not ball in socket • Provides site for 17 muscle attach. • Acromion: shape and non-fusion predispose for problems Proximal Humerus • RC attachments • Bicipital groove Rotator Cuff (RC) • Supraspinatus, Infraspinatus, Subscapularis, & Teres Minor • Function: movement & center H.head in glenoid Long Head of Biceps (LHB) • Superior/anterior stability Labrum • Meniscus of GH joint Laxity=symptomatic, passive of humeral head ; no pain translation Ex: generalized ligament laxity, hx of chronic ankle sprains Congenital :“I’m very bendy” Some able to sublux/dislocate without injury Instability=pathologic condition w/excessive translation of humeral head on glenoid fossa; pain and/or discomfort Traumatic/Sports related injuries Static: ligaments & tendons • Labrum “meniscus of shoulder” Cross-sectional anatomy, microvascularity, and attachments similar to knee meniscus (Cooper 1992) • capsule and ligaments • RC passive tension • neg. intra-articluar pressure (vacuum) Dynamic: muscle contraction RC and LHB contraction Scapular retractors Trauma - dislocations of shoulder may cause isolated or extensive labral injury (Mazzocca 2011) • Anterior labral tear or Bankart lesions • Posterior labral tears or reverse Bankhart lesion • Superior Labrum Anterior and Posterior (SLAP) tears Overhead throwing/hitting athletes • Long head of biceps anchor at superior labrum applies traction during overhead throwing, especially during cocking and deceleration phase (Yeh 2007) • “peel-back mechanism” during cocking phase • Typically SLAP tears www.ptsmi.org Global Laxity • Repeated shoulder subluxations with increased capsular laxity may result in blunting or tearing of labrum www.rpocenter.co m Bruce Springsteen “Born in the USA” History • Important Details / HPI Pain description (location, provocative actions, etc) Acute vs. chronic, frequency With c/o instability: subluxation v. dislocation self-reduced v. trip to ER for closed reduction with conscious sedation Direction of subluxation mechanism of injury temporary numbness/tingling hand dominance Mechanical symptoms: clicking, catching, etc. O’Brien’s Test – SLAP tears or AC injury Apprehension/Relocation – Anterior instability/labral injury Load and Shift – Anterior/Posterior instability Sulcus Sign – Inferior instability Janke test – posterior instability Note: MDI patients will likely have multiple positive tests O’Brien’s Test Apprehension Test Load and Shift Test Sulcus Sign Plain films: AP, outlet, grashey, & AXILLARY! • Cannot truly diagnose dislocation or prove reduction without axillary view • Bony Bankart or Hill Sachs lesions MRI Arthrogram • Labrum and capsule damage seen better w/ dye • Bony edema from osseous injury seen that might not show on plain film Labral Tears MRI arthrogram: 89% sensitive, 91% specific, and 90% accurate (Bencardino 2000) Non-contrast MRI vs MRI Arthrogram (Sheridan 2014) Non-contrast MRI: accuracy 85%, sensitivity 36%, PPV 13% MRI Arthrogram: accuracy 69%, sensitivity 80%, PPV 29% Bankart Tear injury to the labrum at the point of the IGHL (90%) and MGHL (10%) from the glenoid rim (Solomon) Hill Sachs Lesion compression fracture at the posterolateral margin of the humeral head Increased capsular volume Irreversible stretching RC Tears seen typically in dislocation patients over age 40 www.orthoinfo.aaos.org www.crawfordsportsmedicine.com SLAP type Description Treatment I Frayed labrum without detachment Debridement II Labrum & biceps anchor detached from superior glenoid rim Repair III Bucket-handle tear of superior labrum wihtout detachement of biceps anchor Debridement IV Bucket-handle tear extending into and splitting biceps Repair V SLAP II that extends into anterior labrum Repair VI SLAP II combined with parrot-beak type flap tear Repair and debride flap VII SLAP II extending into MGHL origin Repair VIII SLAP II extending posteriorly Repair IX Circumferential tear off glenoid repair Radiologyassistant.nl Anterior Labral Tear www.bacsianh.com Posterior Labral Tear appliedradiology.com Hill Sachs Lesion Anterior Labroligamentous Periosteal Sleeve Avusion (ALPSA lesion) • Associated with anterior shoulder dislocation Radiopedia.org/cases/alpsa-lesion The cymbal company Zildjian which was founded in Constantinople in 1623. Source: American Heritage of Invention & Technology, Winter 2000 Select superior labral tears • Long Head of Biceps Tenodesis or Tenotomy Depends on extent of tear and age of patient Most Labral Tears • Arthrosciopic Labral repair Use of suture anchors or knots to fixate labrum back to glenoid rim • Often performed in conjunction with capsulorrhaphy if capsule is stretched/weakened SURGICAL FINDINGS: 1. Anomalous long head of biceps tendon with no normal tendon in the intraarticular portion of the joint. There was what appeared to be an anomalous long head of biceps tendon running medial to the normal entrance into the joint, and it went superficial to the joint capsule and headed posteriorly. There was a band of tissue that appeared to be the middle glenohumeral ligament attached to the superior labrum. 2. Three hundred sixty degree labral tear. Good labral tissue. 3. Normal glenoid and humeral head articular surface. 4. Normal intraarticular subscapularis tendon. 5. Ninety percent full-thickness articular-sided supraspinatus tear just posterior to the bicipital grove 10 mm in AP dimension. 6. Normal posterior cuff. PROCEDURE PERFORMED: 1. Right shoulder arthroscopy with arthroscopic superior labral repair. 2. Arthroscopic anterior labral repair. 3. Arthroscopic posterior labral repair. 4. Arthroscopic rotator cuff repair. Anterior Bony Bankhart Posterior Bony Bankhart Arthroscopic Remplissage • French for “to fill in” • Infraspinatus used to “fill” large Hills-Sachs lesion in conjunction with anterior Bankhart (Merolla 2014) Boileau 2012 Algorithm for surgical treatment of anterior shoulder instability that has failed conservativ e treatment jaaos.org Shoulder immobilizer x 6 weeks • keeps arm at side with forearm across body • Ultra-Sling immobilizer (Gunslinger) for posterior labrum/capsule to protect repair Begin outpatient PT within few days of surgery • PROM only for 6 weeks • At 6 weeks, may DC immobillizer and begin AROM with PT with 5 lb limit • ROM limitation dependent upon location of repair • If capsulorrhaphy, will hold PT start for 2 weeks SLAP Program may vary between PT departments and/or therapists, but goals same: • Early PROM • Structured rehabilitation • Return to sport 80-90% athletes return to throwing and contact sports (uwhealth.org) 72.5% MLB pitchers returned to competition at a mean of 13.1 months with no significant change in performance (Ricchetti (2010) 68% elite pitchers returned to play at mean of 12 months; 22% never returned to MLB (Harris 2013) Immobilizer for 6 weeks May shower on post-op day 3 and change dressing. No ointments or creams. Do not immerse in water until staples are removed. Physical Therapy 0-3 Weeks • Immobilizer at all times; active hand , active wrist, passive gentle active elbow exercises started immediately • Codman exercises, PROM 0-90 degrees of flexion and abduction; external rotation in adduction to neutral; avoid extension of arm behind body for 4 wks • No external rotation in abduction because of peel-back mechanism • Immobilizer when not doing PROM regimen 3-6 Weeks • Continue sling and start progressive PROM to full as tolerated in all planes • Begin passive posterior capsular and internal rotation stretching • Begin passive and manual scapulothoracic mobility program • Begin external rotation in abduction • Allow use of operative extremity for light activities of daily living 6-16 Weeks • Continue all stretching and flexibility programs as above ROM should be full • Begin progressive strengthening of rotator cuff, scapular stabilizers and deltoid • At 8-12 weeks biceps resistance and sports/work specific exercises instituted with goal of normal function at 4 months For Throwing Athlete • Begin interval throwing program on level surface • Continue stretching and strengthening regimen with particular emphasis on posterior capusular stretching 6 Months • Begin throwing from mound 7 Months • Allow full velocity throwing from mound • Continue strengthening and posterior capsular stretching indefinitely Who was the last Division 1 college football team to finish the regular season unbeaten, untied, AND unscored upon? The University of Tennessee 1939 Solomon,D, et al. “Extensive Labral Tears – Pathology and Surgical Treatment”. Shoulder Instability: A Comprehensive Approach. 36: 426-34.\ Weber, S. DeLee & Drez’s Orthopaedic Sports Medicine. 49: 54349. Yeh, ML. “Stress Distribution in the Superior Labrum During Throwing Motion.” The American Journal of Sports Medicine. March 2005. 33: 395-401. Burkhart SS. :The Peel-Back Mechanism: its role in producing and extending posterior type II SLAP lesions and its effect on SLAP repair and rehabilitation.” Arthoscopy. 1998; 14: 637-40. Mazzocca, A..et al. “Traumatic Shoulder Instability Involving Anterior, Inferior, and Posterior Labral Injury: A Prospective Clinical Evaluation of Arthroscopic Repair of 270 º Labral Tears.” Am J Sports Med August 2011. vol 39. 8: 1687-96. Cooper, DE et al. “Anatomy, histology, and vascularity of the glenoid labrum – An anatomical Study.” J Bone Joint Surg Am, 1992 Jan; 74 (1): 46-52. Nam, E. and S. Snyder. “Clinical Sports Medicine Update. The Diagnosis and Treatment of Superior Labrum, Anterior and Posterior (SLAP) Lesions”. Am J Sports Med. Sept 2003; 5: 798-810. Ricchetti et al. “Glenoid labral repair in Major League Baseball pitchers”. Int J Sports Med. 2010 Apr; 31(4): 265-70. Harris et al. “Return to sport following shoulder surgery in the elite pitcher: a systematic review”. Sports Health. 2013 Jul; 5(4): 367-76. Bencardino JT, Beltran J, Rosenberg ZS, et al: Superior labrum anterior-posterior lesions: Diagnosis with MR arthrography of the shoulder. Radiology 214:267 –271,2000 Solomon and Devine. “SLAP Tears: Pearls and Pitfalls in Diagnosis and Management”. Sports Medicine Update Jan/Feb 2011. p2-6. Merolla & Porcellini. “Infranspinatus strenght assessment and ultrasound evaluation of posterior capsulotenodesis after arthroscopic hill-sachs remplissage in traumatic anterior glneohumeral instability: a retrosecptive controlled study protocol”. Transl Med UniSa. April 2014. 24:; 9: 27-9. Boileau et al. “Anatomical and Functional Results After Arthroscopic Hill-Sachs Remplissage”. J Bone Joint Surg Am, 2012 April 04; 94 (7): 618-626.