Corporate Induction Information Booklet 2014

Corporate Induction
Information Booklet
(Interactive Version)
Important Telephone Numbers
Fire, Security and Other Emergencies 3333
Cardiac Arrest
ICT Service Desk
2222
2771
Estates Help Desk
Switchboard
2451
0
Version 24 – September 2013
1
Contents
Induction
Pages
Corporate Induction Programme including the
Introductory Session
Governance o Governance Framework o Risk Management Strategy o Mental Capacity Act and Deprivation of Liberty Safeguards o Hospital Policy and Procedure
3
4
5
9
10
11
Workforce Issues o Corporate Curriculum and Local Induction o Knowledge and Skills Framework (KSF) and Appraisal o KSF Appraisal Training o Trust Values and Behaviours
12
13
15
16
Safe Environment o Security Awareness o Equality and Diversity o Health and Safety o Medical Devices
Clinical Care o Patient Journey o Patient Safety o Infection Control o Safeguarding Vulnerable Adults o Safeguarding Children o Information Governance o Health Records Standards o Palliative Care
24
26
27
29
30
32
33
35
17
20
21
23
Learning from Experience o Incident Reporting o Complaints Policy and Procedure
38
39
Additional Information o Hospital Chaplaincy o Blood Transfusion Training Requirements
40
41 o Moving and Handling Awareness o Occupational Health Service o Workplace Mediation and Harassment Advice o Harassment Adviser Contact List
43
52
54 o Workplace Mediation Handout 56
58 o Workplace Mediators Contact List o Stress Control Workshops o Health and Wellbeing o Trade Union and Staff Side Information
59
61
63 o Fraud Awareness Guide 64
Appendices o Appendix ‘1’ - Mandatory Training Dates 2010/11 o Appendix ‘2’ - Corporate Curriculum (Mandatory and
66
67
Statutory Compliance Training Delivery)
2
Section 1
Induction
Welcome to Barnsley Hospital NHS Foundation Trust and congratulations on your appointment.
As part of your induction to the Trust, you are required to attend a Corporate
Induction programme that lasts 3 days. You will initially attend a Corporate
Induction introductory session . This session lasts 2 hours and will cover general Trust information whilst it also includes a
Director’s talk.
(To note, if you are a student on a reasonably short Trust placement e.g. 12 weeks this booklet can be accessed instead of attending the face to face
Corporate Induction introductory session.)
The rest of the 3 day programme will be a mixture of face to face mandatory and statutory training courses and e-learning. The courses are section 1 courses from the Trust’s Corporate Curriculum.
Once you have completed the Corporate Induction Programme please make use of the Workforce Information Site and the Training Requirements by
Position report (all posts are listed by position ID). This report will list all mandatory and statutory training you are required to complete for your role.
The Trust’s Corporate Curriculum document (with 4 sections) will also provide you with further information on courses that are offered by the Trust. This can be accessed from the Learning and Development Department’s homepage.
Finally, your Corporate Induction Information booklet should provide you with information to supplement what is covered in the Corporate Induction 3 day programme and your local departmental induction. Please take time to read this thoroughly and use it as an ongoing source of information during your employment with the Trust.
Thank you
Julie Fellows
Learning and Development Officer
September 2013
3
Section 2
Corporate Induction Programme
Aims and Objectives
• To allow new employees and volunteers to meet other new starters and receive a formal welcome to the Trust from a Member of the Board of Directors
• To allow new employees and volunteers to gain an overview of key corporate messages and information
• To signpost new employees and volunteers to how further and more indepth knowledge and information can be obtained via local induction and the Corporate Curriculum
Programme
08.45
09.00
09.05
09.25
10:15
10.30
Refreshments
Introduction and Housekeeping
Director’s Talk
Governance and Transformation
09:45 Workforce Issues
10.05 Safe Environment
Union Talk
Payroll and Pension
ENSURE PROMPT ATTENDANCE TO ALL TRAINING SESSIONS
4
Section 3
Governance
Governance Framework
Definitions:
Governance
Governance is defined in general terms as’ the systems and processes that exist in order to direct and control activities within an organisation.
Corporate Governance
Corporate governance is defined as, an internal system encompassing policies, processes and people, which serve the needs of the organisation and its stakeholders, by directing and controlling management activities with good business objectivity, accountability and integrity.
Clinical Governance
The most widely used definition of clinical governance is the following:
“A framework through which NHS organisations are accountable for continually improving the quality of their services and safeguarding high standards of care by creating an environment in which excellence in clinical care will flourish”.
Governance is about “Getting It Right”, every time.
The main elements of Governance are:
Comprehensive up to date policies and procedures that are fully embedded within the organisation – All Trust policies are developed in accordance with NHS Litigation Authority (NHSLA) guidelines and can all be accesses through the Trusts policy warehouse portal link on intranet home page or by following this link http://sv sharepoint/systems/pt/default.aspx
Clinical audit - highlights deficits in adherence with clinical policies and procedures and identify action to improve practice
Internal and External Auditors – The Trust employs both an internal and external body of auditors in order to monitor the Trusts adherence to its control systems, audits are conducted across a number of areas annually. Clear Audit assessments and improvement recommendations are provided which support assurance to the Board of Directors that the
Trust Systematic processes are being delivered as intended
5
Staff development - ensures staff have the skills and competencies to deliver the organisational objectives and meet the needs of patients and service commissioners
Effective Risk Management - recognising potential issues, assessing the risk to the organisation, developing controls and mitigation to manage the identified risk
Clear processes for organisational learning through o Analysis of incidents o External inspections o Health and Safety issues o National Patient Safety Agency Data o Clinical Audit o Divisional Governance Meetings
R&D/innovation - improve practice, continually innovate / keep up to date
Stakeholder Involvement o Patient/carer involvement - empowers and gives patients/carers ownership o Clinical Quality / contract review with Commissioners
Efficient and Effective use of Resources New ways of working - best use of resources, modernisation and ability to embrace change to meet service needs
Compliance with Standards and Regulatory Frameworks
Information Governance- meeting the NHS Information Risk
Management guidelines
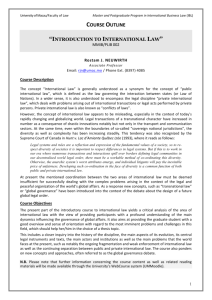
See Governance Mind Map fig 3.1
6
3.1 Governance Mind Map
Operational Practices
Policy and Document
Management Arrangements
Assurance Framework
Assurance Committee Structures
(NCGRC, AC, FC, CGC)
Risk Management
Processes
Governance
Assurance
Risk Registers
Patient Safety
Trust Board
Governors
Regulation & Compliance
CGC
NHSLA
Monitor-
Compliance framework / Code of Governance
Nice
Quality Accounts
IG tool Kit
CQuINs
NPSA
Board Assurance Framework
(Business Objectives Risk Mitigation plan)
Governance Documents
Standing financial Instructions
Schemes of Delegation
Standing Orders
Processes
.
Data Security
Data Quality
Information Governance
Records Management
7
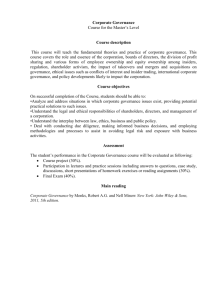
Assurance is provided through to the Governing Council and the Board of
Directors, through a number of Board committees and down to divisions and departments. The major committees are highlighted in the following diagram:-
GOVERNING COUNCIL
BOARD OF DIRECTORS
Audit
Committee
Finance
Committee
Performance Board
Investment
Board
Workforce
Board
Divisional Governance Groups
Non Clinical
Governance &
Risk
Committee
Clinical
Governance
Committee
Executive Team
Quality Safety
Improvement &
Effectiveness Board
RATS
Governance
Assurance
Patient Experience
Board
Corporate Working Groups
Infection Prevention and Control, Strategic Risk,
Safeguarding Children, Safeguarding Adults, Medical Devices
Committee, Falls Steering Group, Radiation Safety
Committee, Clinical Guidelines and Policy Group, Medicines
Management, Nursing Procedures, VTE Prophylaxis Steering
Group, Resuscitation Committee, Organ Donation
Committee, Information Governance Group, Complaints
Review Group, PPI delivery Group, Outpatient Patient Forum,
LNC, Joint Partnership Forum, Equality and Diversity
Steering Group, Health and Safety Committee, Change
Advisory Group, Medical Gas Committee, Decontamination
Strategy Group, Sustainability/Carbon Reduction Group,
Emergency Planning and Business Continuity, Medical and
Surgical Equipment Committee
8
Risk Management Strategy
Risk Management is the reduction in harm to an organisation by identifying and, as far as possible, eliminating risk.
Non-clinical risks include threats to business objectives, finance and threats to the hospital reputation, information governance, as well as staff safety and health & safety matters.
Clinical risks include threats to the safety of our patients, quality of care, and service or business interruption.
Each Division or Department regularly analyses Incidents, Complaints, Claims and Coroner’s Inquests and other sources of risk to assess and manage any emerging themes or problems.
There are four strategy areas that support the process of risk management these are:
Training programmes within the Corporate Curriculum
Policy and Procedures for risk
Committee Structures
Performance Management
Management Arrangements
The Board of Directors has overall responsibility for corporate governance, including risk management. The Board has adopted a framework to its governance arrangements that operates through Board Committees, specifically:
Clinical Governance Committee
Non-Clinical Governance Committee
In addition to these there are other Board Committees dealing with:
Finance
Audit
Performance
Within each Division or Directorate a local Risk or Governance Committee will be held, usually monthly, where risk issues will be considered. Depending on your grade you may be involved directly, but all staff are encouraged to contribute to highlighting problems through the local managers or supervisors or by using the incident reporting system.
For new managers likely to be involved in risk management within divisions the following dedicated training is available along with other courses within the
Curriculum:
Risk Awareness for Senior Managers
Investigation of Incidents and Claims, including Root Cause Analysis
9
Mental Capacity Act and Deprivation of Liberty Safeguards
Introduction
The Mental Capacity Act partially came into force in April 2007 and will be fully implemented by October 2007. It sets out the legal framework for making decisions on behalf of adults aged 16 years or over who lack capacity to act or make decisions for themselves. The Act affects families and carers, health and social care staff and legal, banking and advice sectors.
The Deprivation of Liberty Safeguards came into force on April 1 st 2009. The safeguards provide support for individuals whom as a result of the Mental
Capacity Act may have their freedom of movement and other human rights restricted.
What the Act Does Relevant to Health and Social Care
The
Act provides a framework for assessing a person’s mental capacity and for determining their best interests if they lack capacity to make a decision. It introduces safeguards and limitations for staff when they are working with someone who lacks the capacity to consent to receiving care or treatment.
In some circumstances Independent Mental Capacity Advocates (IMCA) will be appointed to represent people who lack capacity to make important decisions and have no other person to act as their advocate.
Key Messages
It should be assumed that an adult has the full capacity to make decisions unless it is established that this is not the case.
Individuals should be given appropriate help and support to enable them, where possible, to make their own decisions.
An individual’s participation in any decision making process regarding their mental capacity should be maximised as far as possible.
Those assisting and supporting people who lack capacity should not be overly restrictive or controlling and should always try to find an appropriate balance between a person’s right to autonomy and self determination, whilst ensuring that individuals are safeguarded and protected from harm.
Further Information
Further information in the form of Practice Guidance, can be found on the Trust intranet on the useful documents page.
10
Hospital Policy and Procedure
Trust policies are available on the Trust intranet site:
Trust Policy Warehouse - accessed from the A to Z intranet directory under ‘ Policy Warehouse’ or click on the icon at the top of the Trust’s intranet home page
Clinical Policy and Procedure - accessed from the Nursing Procedures intranet pages
Infection Control Policy and Procedure - accessed from the Infection
Control intranet pages
Be aware of local procedure that relates to your own role and responsibilities
11
Section 4
Workforce Issues
Corporate Curriculum
The Trust has developed a Corporate Curriculum to meet the mandatory and statutory training requirements for staff working in the organisation.
The Corporate Curriculum is aligned to the requirements of the NHS inspection regime and external legislation and in particular the NHS Litigation
Authority and Health Care Standards.
Corporate Curriculum
The Corporate Curriculum outlines the category of staff required to undertake a particular development course and the frequency of attendance. The full document (with 4 sections) is accessible on-line from the Learning and
Development Department ’s intranet homepage.
Dates of mandatory training weeks (offering section 1 courses from the
Corporate Curriculum) are listed in Appendix 1 whilst Appendix 2 lists all mandatory and statutory training being offered during these weeks.
For information, a range of training courses can be booked by contacting the
Education Centre ’s Admin Team on extension 2553 . These can also be booked online through the Learning and Development Department’s intranet page. If the course you are interested in is not booked by the Learning and
Development Department the Admin Team will be able to direct you to the correct person.
Local Induction Checklist
To enable a comprehensive introduction to the organisation to be successful, the management of local induction is the responsibility of your immediate line manager.
To ensure a structured approach to local induction, the local induction checklist must be completed within the timescales set for each section and returned to the Learning and Development Department within 2 weeks of commencement within post for permanent employees and within 1 week for temporary employees.
Please note a copy of the induction checklist (for permanent and temporary employees) will be forwarded to all new starters with the new starter pack sent out by the HR Department. Line managers will also receive a copy of the checklist from the HR Department.
12
To note all checklists can be downloaded from the Learning and Development intranet pages under Local Induction.
Simplified Knowledge and Skills Framework (KSF) and
Appraisal
The KSF is an NHS wide framework that can be used consistently across the service to support: o personal development in post o career development o service development
Each role under Agenda for Change has a generic KSF Outline with core dimensions. However, if you are a health care worker up to 3 Health and
Wellbeing specific dimensions will be selected for you by your line manager.
You will be monitored against these.
Overall, the meeting of dimensions and objectives/standards are used to support the KSF Appraisal process and for development and pay progression.
For further information and advice about any aspect of the Knowledge and
Skills Framework, please contact the Learning and Development Department or access downloadable information from the L&D intranet pages.
KSF Appraisal
After induction:
KSF Appraisal takes over
Must take place annually although 1 to 1 (supervision) should be undertaken regularly
Manager to give explanation as to their own role
There are different arrangements for Medical Staff (Doctors and Dentists) and Directors
Information and documentation is available on the Learning and
Development intranet pages
Roles and Responsibilities
Your role:
To complete the KSF Familiarisation workbook (available from the
Learning and Development intranet site under Appraisal Home Page and
KSF Familiarisation Training for Employees)
To participate fully in your appraisal meeting by: o Preparing thoroughly o Contributing to setting targets/objectives, based on the Trust targets/objectives, business plans at corporate and team level and your role o Identifying personal development objectives
13
o Providing upward feedback on support given o To follow up actions agreed at review meetings
Your line manager:
To ensure that you have an annual appraisal (undertaken by line management or alternatively the appraisal can be delegated to an appropriate appraiser)
To undertake 1 to 1s / supervisions on a regular basis
To ensure you undertake your mandatory and statutory training
To discuss your appraisal and future objectives with their line manager
To attend a KSF Master Class in preparation for your appraisal
Your appraiser :
To plan and prepare for your appraisal
To conduct an objective review of performance
To agree future targets/objectives b ased upon the Trust’s targets/objectives, business plans at corporate and team level and your role
To jointly review and evaluate impact of training and development
To identify any training and development needs, priorities and methods
To discuss your appraisal and future objectives with line management
To follow up on actions agreed at the appraisal meeting
To attend a KSF Master Class in preparation for your appraisal
14
KSF Appraisal Training
KSF training is a mandatory requirement for all employees who come under
Agenda for Change and for all appraisers who will be utilising KSF.
The following relates to KSF training for appraisers and appraisees:
KSF Appraisal Skills Awareness - Management Master Class ( for line managers / appraisers who have never appraised )
This is a full day workshop covering all aspects of KSF policy, procedure and documentation as well as the softer skills required when carrying out appraisals. This training is mandatory for all line managers / appraisers responsible for carrying out KSF appraisal who have never appraised before.
To book a place contact the Education Centre on extension 2553 or alternatively you can book on-line through the Learning and Development
Department’s intranet pages.
KSF Briefing / Simplified KSF (for line managers / appraisers who currently appraise )
This is a 1 hour session covering all aspects of KSF policy, procedure and documentation. This training is mandatory for all line managers / appraisers responsible for carrying out KSF appraisals who currently appraise employees.
To book this please contact Ext: 2016.
Preparing for your KSF Appraisal Workbook (KSF Training for Trust
Employees)
Training on preparing for your KSF Appraisal should be undertaken by all
Trust employees (under Agenda for Change) and is mandatory before a KSF appraisal can be carried out.
You can download the above workbook from the Learning and Development
Department intranet site ( under Appraisal Home Page and KSF Appraisal
Workbook for Employees ). To note, this takes about 1 hour (approximately) to complete.
Please ensure that you let the L&D Department know that you have completed the workbook . You can fill out a completion form on the L&D intranet site ( under Appraisal Home Page and KSF Appraisal Workbook for
Employees ) or call Ext: 2553.
15
Trust Values and Behaviours
Please ensure that at all times you are living the Trust values:
Our Values
Value: We treat people how we would like to be treated ourselves
We will :
Show you respect, courtesy & professionalism
Treat you with kindness, compassion & dignity
Communicate with you in a clear, honest & responsible manner
Value: We work together to provide the best quality we can
We will :
Share the same goals, finding answers together
Recognise your contribution by treating you fairly & equally
Constantly learn from you, so we share & develop together
Value: We focus on your individual & diverse needs
We will :
Personalise the care we give to you
Keep you informed & involve you in decisions
Take the time to listen to you
16
Section 5
Safe Environment
Security Awareness & Crime Prevention
AIM OF SECURITY AWARENESS & CRIME PREVENTION
To ensure that our staff and patients are (and feel) secure and safe at all times
OBJECTIVES – We do this by:
Reinforcing a security awareness with Trust staff and patients
Removing or reducing the risk of crime
Preventing violence, aggression and harassment to staff and patients
Protecting all property against theft or criminal damage
Ensuring a close working relationship between the Trust and local police
ASSIST CRIME REDUCTION IN THE WORKPLACE
10 USEFUL TIPS TO REDUCE CRIME:
1. Keep your personal belongings safe and secure at all times.
2. Close your office window and lock your door, even if only out for a minute.
3. Do not leave anything visible in your car, clothing is the second most stolen item.
4. Report all breaches of security to your line manager immediately.
5. Report weaknesses in existing security systems to your line manager.
6. Challenge unknown people in your workplace IF SAFE TO DO SO.
7. Make use of existing security systems such as access control, alarm systems, personal alarms, locks, policies etc.
8. Always think safety, be aware of your surroundings and be safe.
9. Report all incidents of violence and aggression, loss and theft on the IR1 system.
10. Ensure your escape route is clear when dealing with service users and the public.
IDENTIFICATION (I/D), SMART CARDS AND ACCESS FOBS
You must wear your photo identification at all times
Politely challenge anyone not wearing photo I/D
Your I/D must be produced if requested
Wearing I/D protects you and your colleagues
– Trust Policy
Any loss of card(s) or access fob must be reported immediately
PROTECTING YOURSELF & YOUR VEHICLE
Avoid poorly lit streets, areas and less busy locations
Consider carrying a personal attack alarm
Check your car regularly, any breakdown can leave you vulnerable
17
Always remove your ignition key on leaving your car and secure all doors and windows
STAFF RESIDENCES
Display your parking permit if your vehicle is parked on the Trust site
Report anyone or anything suspicious to Security and/or the Police
Ensure all doors and windows (particularly ground floor) are closed and
secure
Take care that curtains are properly closed
Keep your keys secure, report any loss immediately and do not duplicate keys
Do not mark or tag residence keys with your details or address
VIOLENCE & AGGRESSION
The Trust will robustly deal with all incidents of violence and aggression to staff including prosecuting offenders.
All incidents must be reported by electronically submitting an IR1 form
Conflict Resolution Training is available and mandatory for all frontline staff. Liaise with your line manager or the Education Centre
Customer Care Training is also available for other members of staff
REPORTING SECURITY INCIDENTS
All incidents must be reported by the individual member of staff
Security incidents are reported using the Trust incident reporting System via IR1
Immediate assistance is available by ringing 3333
Ensure that your line manager is informed of any report made
CRIME PREVENTION
Any thoughts or ideas to reduce crime or protect staff and patients are always welcome. Please contact Mike Lees (2310) or Lisa Corbridge (5413)
URGENT ASSISTANCE
Emergency contact number
– 3333
LOCAL SECURITY MANAGEMENT
The Head of Resilience and Security and Trust Local Security Management
Specialist (LSMS) is Mike Lees supported by Lisa Corbridge. They can be contacted on Extensions 1386 or 1387
The Security Office can be contacted on Extension 4948
FINALLY
SAFETY AND SECURITY IS MAINTAINED BY TEAMWORK, VIGILANCE AND
COMMON SENSE.
18
Violence and aggression
The trust has a zero tolerance policy in relation to Violence and Aggression please ensure that you report all incidents with the Incident Reporting System
(Sentinel)
Training
Conflict Resolution Training with some Customer Care
[high/extreme risk]
The trust provide Conflict Resolution Training (Mandatory and Statutory Level
1 course) for all members of staff that experience high/extreme levels of violence and aggression, these areas have been identified through the completion of a risk assessment by the lead for your area. To note, some customer care training will also be offered.
This training can be booked by you or your lead via the SharePoint site on the
Learning and Development intranet site.
Customer Care with some Conflict Resolution Training
[low/moderate risk]
Areas at low/moderate risk of experiencing violence and aggression are now being offered a new course that consists of Customer Care but with some
Conflict Resolution Training . This course has been categorised as a
Mandatory and Statutory Level 2 course. It will serve two functions a) help to maintain and improve customer care and b) help to keep employees safe.
This training can be booked by you or your lead via the SharePoint site on the
Learning and Development intranet site.
19
Equality and Diversity
The Trust has an Equality and Diversity Advisor. The work of the Equality and
Diversity Advisor is to ensure the Trust reflects the Equality requirements detailed in the Equality Act 2010. These are:
Promoting Equality of opportunity
Promoting good relations between others
Eliminating unlawful discrimination.
To that end the content of our equality training considers recent equality legislation which includes all 9 protected characteristics (otherwise known as
PC’s). These protected characteristics are: o Race o Religion or belief o Age o Sex o Sexual orientation o Gender reassignment o Disability o Marriage and Civil partnership o Pregnancy & maternity
This work is reflected through a number of mediums: o Quarterly E&D Strategic Steering Group- chaired by Director of
HR&OD. o E-Learning package. o Equality Impact Assessment Master Classes. o Diversity Champion workshops. o Cultural Communication Awareness Training delivered by our local community partners. o Staff electronic briefings. o Equality &Diversity webpage(SharePoint) . o Staff Induction training. o Trust annual Equality and Diversity report.
Further details can be accessed on the Learning and Development website for dates and venues of training.
You’re Equality and Diversity Advisor is:
Beverley Powell
Human Resources Department
Block 1
Gawber Road
Tel: (01226) 43 2757 beverley.powell@nhs.net
20
Health and Safety
The Health and Safety at Work etc. Act 1974 places a statutory responsibility for health and safety on the Trust as an employer in relation to its employees.
The Act also places a responsibility upon you as individual members of staff.
Policies and Procedures
There are a number of policies and procedures in place for all aspects of health and safety within the Trust. Copies of the policies can be obtained on the Trust’s intranet pages.
Fire Safety
Regulatory Reform (Fire Safety) Order 2005
The above legislation sets out the following duties:-
Risk assessments have been undertaken by a competent person
All employees have a duty to:-
Carry out basic fire prevention techniques
Know who their fire marshals are
Know the Trust’s fire procedure
Know the evacuation procedures
In all circumstances, if any person suspects or discovers a fire, you must:-
Break the nearest break glass point
Confirm the incident to the switchboard by calling 3333
Health and Safety Training
The Health and Safety Department provide training on all aspects of health and safety: Stress, COSHH, Working at Heights, Noise etc
Annual fire, health and safety training - Part of the Trust’s Mandatory training Week
Three day Health and Safety Management Training course aimed at all
Managers, Supervisors and Health and Safety Trade Union
Representatives
One day Health and Safety Management Training course aimed at all
Board Members and Directors
21
Health and Safety - Key Contact
If you require further information or advice on any aspect of health and safety please contact :
Victoria Davies – Health and Safety Co-ordinator
Extension 2140
22
Medical Devices
The Trust manages its medical devices in line with the recommendation of the
Medicines and Healthcare Products Regulatory Agency (MHRA) Directive
Bulletin DB2006(05) Managing Medical Devices.
Policy and procedures relating to medical devices are on the hospital intranet site under the Medical Device Co-ordinators Group link.
All staff have a personal responsibility to keep up to date with training and minimum training requirements can be found in each clinical area.
Each clinical area has an Equipment Controller who can direct staff to information related to use of medical devices.
Any member of staff can request update training at any time for any piece of equipment they may be required to use.
Decontamination of medical equipment must be undertaken in accordance with the Decontamination Policy.
Any equipment found to be faulty must be decontaminated and labelled
‘ready for collection for repair’.
No member of staff may use any piece of equipment unless they have received training and been deemed competent to use it safely.
23
Section 6
Clinical Care
Patient Journey
Patients fall into 3 categories
– outpatients, day cases and inpatients.
Outpatients
The majority of outpatients are referred to clinics by their GP, via the Choose and Book System, where they will attend a consultation.
Due to the nature of the visit it is sometimes viable for outpatients to move from one consultant to another.
Inpatients
Inpatients fall into two categories - emergency and planned admissions.
Planned Admissions and Day Cases
These patients are given a date for admission following clinic attendance. If they are to have surgery they may attend a pre-assessment clinic to prepare as much as possible before the day of admission.
Some patients may be admitted directly to the Day Surgery Unit and be prepared for theatre there. They will have their surgery, be recovered and discharged home again on the same day from this unit.
Patients with more complex care needs will be admitted to an inpatient ward and go to theatre, usually on the same day. Some patients will be admitted to the surgical assessment unit and transferred to an inpatient ward directly from theatre; others will be admitted directly to the inpatient ward. These patients may take some time to recover from their treatment and will spend a number of days on the ward before being discharged home.
Emergency Admissions
The majority of these patients are assessed and admitted to the wards through A&E. Medical patients will be taken from A&E to ward 18 which is the
Medical Emergency Unit (MEU), and after thorough assessment and treatment will either be transferred to another medical ward or discharged home
24
Key Quality Aspects of the Patient Journey
Patients should be given appropriate information to help them make informed choices about their care
Communication with staff, patients and visitors should be clear and respectful at all times
Privacy and dignity should be maintained at all times
Policy and procedures are available to guide practice and ensure a professional approach to care and should always be adhered to
All staff have a part to play in ensuring that patients experience high quality care
Departments
Women’s and Children’s:
Children’s services
Gynaecology
GU Medicine
Maternity
Neonatal Unit
Obstetrics
Medicine:
Cardiology
Chemotherapy
Dermatology
Diabetes
Elderly Medicine
Emergency Department
Gastroenterology
Medical Investigation Unit
Respiratory
Stroke
General Surgery:
Audiology
Dental
Endoscopy Unit
ENT
General Surgery
Orthopaedics
Ophthalmics (supplied from Rotherham)
Urology (supplied from Sheffield)
Wards 30 - 34
For other specialist services or complex care patients are transferred to other hospitals.
25
Patient Safety
7 Steps to Patient Safety
Building a safety culture
Leading and supporting staff
Integrating risk management activity
Promoting reporting
Involving and communicating with patients and the public
Learn and share safety lessons
Implement solutions to prevent harm
The Trust’s Strategy for Patient Safety is built around the National Patient
Safety Agency’s 7 Steps to Patient Safety. It is included in the Risk
Management Strategy, and there are also separate policy documents, such as the Incident Reporting Policy, that provide more detailed procedures about how elements of the strategy are implemented.
26
Infection Control
Infections acquired as a result of healthcare have a major impact on both the patient and the healthcare provider. For the patient, the acquisition of infection causes anxiety and discomfort, delays recovery and in some instances results in long term morbidity or even death.
Each year healthcare associated infec tions (HCAI’s) are estimated to cost the
NHS £1 billion and annually 5000 deaths are attributed to healthcare associated infections. Locally targets are set in relation to specific HCAI’s.
Failure to meet these targets results in substantial financial penalties and ultimately has an effect on the Trusts reputation.
Infection Prevention and Control clearly has an important role to play in ensuring patient’s receive high quality care. Many challenges are faced, including the ever increasing threat from antimicrobial resistant microorganisms, the emergence of new pathogens, growing service developments, national guidelines and targets. Good infection prevention and control is essential to ensure that people who use health services receive safe and effective care. Effective prevention and control of infection must be part of everyday practice and applied consistently by everyone.
Infection Control Policies and Procedures
These are found on the hospital intranet site. Click onto Infection Control and you will be directed to the Infection Prevention and Control website.
Training
Annual Infection control training is mandatory and encompasses hand hygiene, MRSA, Clostridium difficile, barrier nursing, decontamination, standard infection control precautions and sharps safety.
HIV and blood borne virus study day. This is mandatory for all nursing staff and is a once only session. Subsequently a 3 yearly update in required.
Training is also provided on current topics e.g. influenza. Practical aspects of hand hygiene is provided by the ‘Clean Your Hands Champions’ in each clinical area annually.
Specific training on Infection Control issues can also be accommodated.
Please feel free to contact the Infection Prevention and Control team for advice or support.
Consultant Microbiologist &
Director of Infection Prevention &
Control
Dr J Rao Ext: 2749
Bleep 207
Consultant Microbiologist Dr Y M Pang Ext: 4986
27
Assistant Director of Infection
Prevention & Control
Specialist Nurse, Infection
Prevention and Control
Clinical Nurses, Infection
Prevention & Control
Denise Potter
Christine Fisher
Susan Burns &
Lynda Slater
Ext: 2825
Ext: 2825
Bleep 472
Ext: 2825
Bleep 371,411
28
Safeguarding Vulnerable Adults
Introduction
‘There can be no hiding places when it comes to exposing the abuse of vulnerable adults’
‘All workers at all levels of the organisation have a responsibility to respond to adult protection concerns ’.
No Secrets - Department of Health 2000
Who is a ‘Vulnerable Adult?’
A vulnerable adult is a person who is or may be in need of community care services by reason of mental or other disability, age or illness and is unable to care for him/her self, or unable to protect him/her self against significant harm or exploitation.
What is abuse?
It may be a single act or systematic ill-treatment of vulnerable adults
It may be intentional
Multi-agency policy and procedures are established in Barnsley and are available to assist staff in identifying abuse and acting upon findings.
Trust Processes?
Any member of staff who suspects abuse should report this to the Named
Nurse for Safeguarding Adults. This concern will then be investigated using
South Yorkshire Safeguarding Procedures in partnership with other social care and health agencies.
It is essential that any concerns are communicated and acted upon.
Remember:
Safeguarding is everybody’s business
Ian Boldy
Named Nurse Safeguarding Adults
Ext 5432
AP 1249
29
Safeguarding Children
Mission Statement
At this Hospital, we believe that abuse of any kind is unacceptable, and that everyone has a right to live their life free from violence and fear (Art.3 Human
Rights Act), particularly children.
We are committed to working in partnership with other agencies that are working to safeguard the welfare of children and protect them from harm.
Statutory Duty
The Children Act 2004 (Sect. 11) places a duty on the Hospital to: discharge its function with due regards to the need to safeguard and promote the welfare of children.
The Children Act 1989 places a duty on all staff at BHNFT to:
Put children first
– their needs are paramount (Part1)
To share information and concerns and refer to investigating agencies
To co-operate with investigating agencies (Sect. 27)
Training
Children and families have a right to expect the highest standards of care and competence from all the professionals they come into contact with. Staff should know how to recognise and respond to concerns about the welfare of a child even if working in adult focused areas. This is both an organisational responsibility to provide training and a professional responsibility to undertake training (Working Together 2006 4.4 - 4.6). The Trust Curriculum and
Safeguarding Children Training Strategy require mandatory training for safeguarding children.
For staff who do not have contact with clients/patients, they should access
Level 1 training – Safeguarding Children Basic Awareness (non-patient contact). This staff group simply need to read a leaflet and answer three questions. The leaflet is available through NMLS (s earch for ‘safeguarding children’ and locate the course 163-0370305 – Safeguarding Children nonpatient contact e-learning 2011). Alternatively, staff can obtain a hard copy by ringing 2092 to request. This must be undertaken every three years.
All staff at BHNFT who come into contact with clients/patients should undertake Safeguarding Children Basic Awareness training Level 2 training, either as:
Taught session (via the Training Dept)
E-learning package (please ring 2092 for login details)
Bespoke sessions in departmental areas (contact the team on 2092 to arrange)
This training should be undertaken every three years.
30
All staff that have significant contact with children and families should build on their understanding and knowledge, and should access level 3 multi agency training. For more details of training levels and how to access training, please visit the Safeguarding Children Intranet page, or ring the department on 2092 to discuss.
WHAT TO DO IF YOU SUSPECT A CHILD IS BEING ABUSED
Listen, don’t promise confidentiality.
Talk to your line manager.
Seek further advice and support from the Named Nurse Safeguarding
Children on ext 2092. The Team is available Mon – Fri, 9am to 5pm.
Advice out of hours should be sought from the Paediatrician on call.
Make reference to the Child Protection Procedures, which can be found on the safeguarding children intranet page.
Check the Safeguarding Children List on Barnsley 772361 (office hours). Out of hours contact the Emergency Duty Team on 0844 984
1800.
Make a ref erral to Children’s Social Care as appropriate
ALWAYS MAINTAIN YOUR FOCUS ON THE CHILD .
31
Information Governance
Dr Jugnu Mahajan - Caldicott Guardian
All NHS Trusts have an appointed Caldicott Guardian who oversees all aspects of Information Governance.
Terri Milligan – Information Governance Manager
If you have any questions or queries please contact the Information
Governance Department Ext 2017
What you should know about Information Governance!
Never access a work colleague, family member or friends’ records
Never share passwords or smart cards – an audit trail exists
If asked for confidential information always:
Ask why? Is there a legitimate reason for the request?
Ask for proof of the identity of the person requesting the information
Ask your manager for advice if unsure
Report instances of a security/confidentiality breach to the Information
Governance Department.
Beginners Guide to Information Governance
The Beginners Guide to Information Governance is a 30 minute training module which has replaced TIGER and is mandatory to all staff. The training can be completed either through e-learning on NLMS or a classroom session can be booked through the Education Centre.
This training should be completed once only followed by the ‘Refresher’ module’ on an annual basis.
Refresher Module
The Refresher module is mandatory to all staff and takes approximately 15 minutes to complete via e-learning using NLMS. This training should be taken annually following completion of the ‘Beginners Guide to Information
Governance’.
Both the Beginners Guide and the refresher module provide all employees with the necessary knowledge on Information Governance legislation and
Policy to ensure staff are aware of their personal responsibilities.
32
Clinical Audit / Health Records Standards
This information contains:
Health Record Standards for all staff who make an entry into a health record at BHNFT e.g. Nurses, Midwives, Medical Staff, Allied Health Professionals and admininstration staff.
A health record
A health record should be contemporaneous and a complete record of a patient’s care and treatment. This will ensure good patient safety, demonstrated by complete, accurate and timely records giving a clear picture of events s o that “those coming after you can see what has been done, or not done, and why and by whom”. This will ensure not only that patient care is not compromised but also that “any decisions made can be justified or reconsidered at a later date”.
Clinical audit of standards
A clinical audit of record keeping standards will be undertaken in all specialties at least once in any 12 month period. Both the content and quality of the note keeping will be audited.
STANDARDS
Factual information:
Record contains only factual information (no comments about appearance, or habits etc), unless clinically relevant.
Chronological order:
All records are in a chronological order, with the latest documents at the rear of the current admission, within the speciality section.
Securely fastened:
All records must be securely fastened within the folder e.g. test results, medical notes and referral letters.
All entries must be:
Legible (staff, patients/carers are able to read them but not necessarily understand)
Written in black ink
Dated, timed and signed
Have printed name (or use stamp or GMC number)
Designation
Bleep number if applicable
Each page of the current admission contains:
Patient’s full name
Date of birth
Hospital ID number
NHS Number
33
Accident and Emergency record:
If the patient has attended Accident and Emergency and has subsequently been admitted, there should be a copy of the Accident and Emergency record contained in the patient’s notes.
Maintenance of record for accuracy:
Ditto marks are not used
Only the Trust’s approved abbreviations are used
Errors are crossed out with a single line
Errors are signed
Errors are dated
Errors are timed
Printed name alongside correction (or use of stamp or GMC number)
Correction fluid is not to be used
Record contains:
Assessment (initial patient history)
Assessment (past medical history)
Operation notes (if applicable)
Diagnosis/problem
Treatment/care plan
Drug prescription chart present if required
Discharge information must include:
A copy of the electronic discharge summary is in the notes.
How can I find out more?
For more information on the Trust’s Standards or the clinical audits being carried out, please do not hesitate to contact:
Deputy Director of Nursing Ext. 2299
Clinical Audit Ext. 2191
34
WELCOME TO BARNSLEY HOSPITAL SPECIALIST
PALLIATIVE CARE TEAM (HSPCT)
Sara Andrews Macmillan CNS in Specialist Palliative Care Ext 4921 Bleep
404
Annette Clark Macmillan CNS in Specialist Palliative Care Ext 4921 Bleep
384
Claire Brown Trainee Specialist Palliative Care Nurse
Vacancy Trainee Specialist Palliative Care Nurse
What is Palliative Care?
Palliative care is the person-centred attention to physical symptoms, psychological, social and spiritual distress and cultural needs in patients with limited prognosis, in order to optimise the quality of life for the patients and their families or friends.
General palliative care is palliative care that should be provided by all health and social care professionals, in primary or secondary care, within their duties to patients with life-limiting disease.
Specialist palliative care is palliative care provided at the expert level, by a trained multi-professional team, in order to manage persisting, severe or complex problems. It also provides specialist educational and practical resources to other non-specialist members of the primary or secondary care teams.
(Adapted from: Ahmedzai et al. The European School of Oncology International Working Party Report 2002)
When should I refer and for what reason?
In order to support clinical staff referring to the specialist palliative care teams in Barnsley, a set of ‘eligibility’ criteria have been developed that provide guidance. These criteria apply to all adult patients referred to the Specialist
Palliative Care Team. o The patient has active, progressive or advanced disease and the focus of care is quality of life. o Palliative care needs may be physical, psychological, social or spiritual and not based on diagnosis or prognosis.
Referral to specialist palliative care should be considered for any patient with or without cancer whose level of need is considered beyond the scope of the current caring team. Occasionally, other professionals need support in deciding which patients should be referred and therefore the following examples may be helpful but if in doubt please contact the team for further advice.
35
What sort of referrals meets the ‘eligibility’ criteria?
o Uncontrolled, complicated or multifaceted symptoms or short term specialised nursing requirements relating to mobility, functioning or self care including care close to death. o Emotional or behavioural difficulties relating to illness. o Social issues involving family, children, carers, finances, communication, carer crises where urgent admission has been necessary to enable the family to cope. o Unresolved issues of self-worth, loss of meaning or hope, complex decisions around withholding or withdrawing care.
What sort of referrals would not meet the ‘eligibility’ criteria?
o Conditions where the disease is inactive and stable and needs are unchanging. o Long term intensive nursing needs in the absence of other identified palliative care needs where longer-term care arrangements need to be made. o Long term care. o Hospital inpatients with stable disease who solely require additional practical support discharge.
When will the patient be contacted?
The standards for being contacted by a specialist palliative care professional are: o Routine - within three working days o Urgent - within two working days although wherever possible advice will be given at the time of referral
How do I make a Referral?
All referrals should be made to the team and will be triaged by the Clinical nurse specialist. Referrals may be made by any health or social care professional by telephone as follows:
Monday to Friday 9 am to 4 pm
Sara Andrews, Macmillan CNS (Bleep 404)
Annette Clark, Macmillan CNS (Bleep 384)
Tel: 01226 730000 Ext 4921
Direct Line: 01226 434921
(Only urgent referrals can be made via bleeps 384/404)
Consultants in Palliative Medicine
–
Dr Becky Hirst, Dr Rachel Vedder, Dr Sarah Wilcox (Locum)
(All the consultants are part time)
The Consultants Based at Barnsley Hospice (Secretary 01226 244244 Ext
252) but provide specialist palliative medical input to all the services in the
36
Barnsley district. The consultants attend the hospital on Monday, Tuesdays,
Wednesday and Fridays for ward rounds, education, service development and patient reviews.
The Consultants ward round times are variable therefore; referrals for the consultants must be made through the Clinical Nurse Specialists’ for triage.
Specialist Palliative Care Multi-disciplinary meeting
The HSPC team meet with the Community SPC team and the Hospice team on a weekly basis (Thursday 9-11am).The team present and discuss all new referrals and complex patients.
The meeting is held at Barnsley Hospice, therefore there are no HSPC team members in the hospital during this time.
Further information can be found on the Palliative Care Intranet site which is updated regularly.
37
Section 7
Learning from Experience
Incident Reporting
Incident reporting is the foundation of an effective risk management system.
The Incident Reporting Policy seeks to promote the reporting of all categories of incidents and near misses including serious incidents (SIs). (If you are involved in a serious incident where there is serious injury or perhaps the unexpected death of a patient escalate your concerns immediately to a senior manager or Trust Director).
An incident is any unexpected event, such as a patient fall, an injury whilst working, a medication error, or a complication of a patient treatment.
Reporting of incidents allows us to learn and improve services, and to identify any risks or trends we may have.
To report an incident you will need to:
Obtain a user name and password to access the Incident reporting system on the intranet (Sentinel IR1 on the left of the main menu).
Contact Risk Management on extension 2209 / 4572
Find your key trainer on your ward or department
Access the e-learning package
Training can also be offered through the risk management team, and managers likely to be involved with the investigation of incidents should attend the Investigation of Incidents and Claim/Root Cause Analysis Training available through the Corporate Curriculum.
Raising Concerns
The Trust also has other routes for highlighting concerns, and a range of policy documents can be found on the Policy Warehouse on the intranet, for example:
Whistle Blowing Policy
Bullying and Harassment
Concerns about patient care can also be reported directly to the National
Patients Safety Agency ( www.npsa.nhs.uk
)
38
Complaints Policy and Procedure
The Complaints Procedure provides a legal framework by which users of the
NHS can complain. It is intended to offer fairness to patients and staff, be a rapid and open process, and be honest and thorough. This can be quite a challenge and strict time frames are often involved. The stage that involves the hospital is called ‘Local Resolution’.
Complaints Procedure
Before a complaint becomes ‘formal’ we do like to think that most concerns and issues can be resolved on an informal basis on the ward or department.
Depending upon your role, you may be able to help resolve problems yourself, or through your manager, generally the Lead Nurse or Matron for the area.
If the person needs additional support or advice contact the Patient Advice and Liaison Service (PALS) on 2430, based on main reception. This may include people with special needs, such as translation service or disability etc.
If the person wants to make their complaint ‘formal’, contact the Complaints
Team on 2863 or provide the Complaints Leaflets which are available on each ward. A leaflet has been enclosed for your reference.
You may also wish to sign post them to the Independent Complaints
Advocacy Service (ICAS) on 0300 456 8349 who can help people with bringing a complaint.
Formal Procedure
If you receive a letter or serious complaint ensure it is passed to a manager or the Complaints Team promptly. It is important that the complaint is:
Registered and acknowledged within 3 days
– Complaints Team
Investigated by a formal process (e.g. root cause analysis) via a Divisional
Manager
Individually resolved through an agreed plan, outcomes and time scales
Responded to by the Chief Executive within the agreed time scale
Subject to clearly demonstrated Learning and Improvement where appropriate
If a person is not satisfied with how their complaint is handled they can go to the Health Service Ombudsman.
Further Advice/Training
The Complaints Policy and Procedure and other guidance documents are available on the Trust Policy Intranet site or from the Complaints Team.
Further advice and training is available by contacting Lynsey Cutler,
Complaints Manager on 2571.
39
Section 8
Additional Information
Hospital Chaplaincy
Chaplains are appointed by the Trust for all the Christian denominations. The
Church of England priest and Chaplaincy Manager are full time: Bleep 345,
Extension 2725, or via switchboard.
Switchboard can always contact the part-time Roman Catholic and Free-
Church Chaplains if you would particularly like to speak to them at any time.
There is a chapel open at all times to anyone for prayer or just for some quiet.
This is situated on the ground floor near to the lifts which serve wards 16 to
24. Do feel free to come into the chapel at any time and put the lights on if it is dusk or at night. The chapel is used by all denominations for their services.
Weekly, in the chapel, there is a Eucharist Service for Anglicans (Sunday
10.45 am) and, occasionally, worship for Free-Church people (Sunday 6.00 pm) – people of all denominations are most welcome to come and take part in both these services. The services last for about 30 minutes. No one minds bleeps going off or people coming and going at any time during these!
The Chaplains can provide details of local Barnsley churches and places of worship if staff members are looking for a particular form of worship and do not know the area.
A group of staff meet for prayer and fellowship in the chapel with the Free-
Church Chaplain each Wednesday 12.45 pm to 1.15 pm and there is a
Christian meditation group on the first Tuesday of every month at 1.00 pm in the chapel which lasts for about ½ hour.
Everyone is welcome.
For Muslim people, residential block 13 has a floor set aside for prayer and meetings. Details of the keypad admission are available from the hospital reception. Please get in touch with Dr Sharlala, in Rheumatology (Bleep 365) or Dr Hamed in Cardiology, on bleep 599 for information about worship taking place in the prayer room.
If the Hospital Chaplains can be of personal help to you in any way at all during your time in Barnsley, please don’t hesitate to get in touch – we are here to provide a confidential service for members of staff or volunteers, as well as for our patients! Sometimes it helps to have a chat with someone outside your particular profession. The office is next to the chapel, call in at any time, or, if no one is around you can ring or bleep.
Pay a visit to our intranet site for full details of chaplaincy activities.
40
Blood Transfusion Training Requirements
Mandatory training is essential to ensure that all staff are fully aware of and are able to comply with both National standards and Trust guidelines to maintain safe transfusion practice.
Staff Roles
It is the role of the medical staff and appropriately trained Advance Nurse
Practitioners to ensure the appropriate use blood/blood components. They also have the sole responsibility for the request and prescribing of blood/blood components.
All staff members who perform venapuncture to obtain pre-transfusion blood samples must be aware of and comply to Trust and MHRA ( Medicines and
Healthcare products Regulatory Agency) requirements to ensure samples are labeled appropriately. All staff must be receive suitable training and achieve practice competency which should be updated every 3 years
Following the installation of the BARS (Blood Audit and Release System) any staff member who has been trained and deemed competent can issue and remove blood/blood components from the Blood Bank fridge and transport them safely to the ward/dept 24/7.
At ward/dept level Registered Nurses and Midwives play a key part in the pretransfusion checking process ensuring that the right patient receives the right blood/blood component.
All staff have a duty to report any adverse events or incidents for further investigation by the Blood Bank team, which if necessary will be escalated to the appropriate external agencies.
Available training
As identified in the Trust Corporate Curriculum appropriate bi-annual up-date training is available to all relevant staff groups by either;
The Hospital Transfusion Practitioner who will deliver formal training sessions by prior arrangement with individual ward/dept. or staff groups.
A variety of self directed E-learning packages are available via NLMS on the hospital intra net site designed to meet the needs of individual staff groups in relation to their roles and responsibilities within transfusion
A locally produced ‘on-line’ distance learning package aimed at long term medical staff of all grades - Safe and Appropriate use of blood products (BHNFT medics)
Additionally, in line with the National Patient Safety Agency safe practice notice 14, Right patient, Right blood ( www.npsa.nhs.uk
). All staff members
41
responsible for the collection, transportation and administration of blood/blood components must complete a three yearly competency based assessment.
All assessments must be completed by appropriately trained departmental staff or the Transfusion Practitioner.
42
Moving and Handling Awareness
What is Moving and Handling:
Any application of force to an object or an individual, including:
Lifting and lowering
Holding and carrying
Pushing and pulling
Throwing and catching
But more than this it also involves and influences the postures and positions we assume 24 hours a day, the way we sit, the way we stand, the postures and positions we adopt at work and at play. Anything, in fact, that influences spinal loading.
Remember:
There is no such thing as completely safe handling, but we can reduce loading on the spine by reducing the risks as much as possible.
We must AVOID handling wherever possible.
Principles of safer handling:
Avoid
Assess
Plan
Prepare
Perform
Why bother with moving and handling training?
More than a third of all accidents reported to the Health and Safety Executive
(HSE) are handling related. Back pain is the leading cause of sickness absence from work and is increasing in all sectors of industry.
Employer/Managers duty:
Avoid the need for hazardous moving and handling as far as is reasonably practicable
Assess the risk of injury from hazardous moving and handling that cannot be avoided
Reduce that risk of injury as far as is reasonably practicable
43
Employee’s responsibilities:
Follow Safe Systems of Work
Make proper use of the equipment provided
Seek help; do not put yourself or others at risk
Report any problems
Organisation of training within the Trust
Moving and Handling training is a mandatory requirement for all Trust employees.
Some Trust wards and departments have moving and handling key trainers working within them, able to provide information and training in safe practice and as identified in that ward or departments’ risk assessments.
For those areas and departments without key trainers, training is provided by the Moving and Handling Specialist, and a number of Mandatory sessions are scheduled for both clinical and non clinical staff on a monthly Corporate
Curriculum basis. Training consists of a theory/loads session, mandatory for all staff, and a practical people moving and handling session for those clinical staff delivering hands on patient cares. Details of these sessions are available from Education Department staff on ext 2553 or from the Moving and
Handling Specialist on ext 4939.
Training programmes
If arrangements are not made for your training, inform your manager, supervisor or the Moving and Handling Specialist based in the Occupational
Health Department.
Trust policy is that staff will not be expected to move or handle hazardous loads until they have received appropriate training.
It should not be presumed however that the provision of training alone will ensure safe manual handling, and has to be fully integrated within a system of risk assessment, care planning and a general awareness of safer systems of working.
Who gets pain?
8 out of 10 people get pain at some point in their lives
Most pain is due to sprains and strains which will naturally recover
Most pain is NOT due to serious disease or damage
(Faculty of Occupational Medicine 3/2000)
What if I get pain in the workplace?
Pain is your body’s first line of defence
Identify the cause if possible
Look at / change your work practice
44
In the event of injury:
Report to your supervisor or line manager
Complete an IR1 Accident Form as soon as possible
Seek adequate and appropriate treatment and pain relieving medication
Dependent upon the type and nature of your condition you may be seen by Occupational Health or the Moving and Handling Specialist
Occupational Health Dept:
Provides an impartial and confidential service for all aspects of health at work.
As well as advice and assistance on early return to work and workplace assessments
Managers can refer staff for assessment/advice
Staff members can self refer for assessment and advice
Occupational Health Dept: Ext 4939
Moving and Handling Specialist Ext 4935
Recovery:
Hurt does not mean harm. Pain is subjective and the level and extent of the pain experienced does not necessarily reflect the amount of damage we might perceive
Back pain is common, but rarely due to any serious disease
Prolonged bed rest is not good for you
Staying active will help you get better faster and prevent more back trouble
(The Back Book, TSO 2004)
Recovery:
Pain relief
Massage/manipulation
Heat/cold
Movement, movement, movement
What can I do personally to reduce the risk of back pain?
Get fit, keep fit
Adopt a good posture
Watch your weight
Quit smoking
Know your own capability and work always according to the risk assessments and safe systems of work for your area
Shaun Carney
Moving and Handling Specialist
Occupational Health Department
BHNFT
45
Occupational Health and Wellbeing Service
Barnsley Occupational Health and Wellbeing Service operates as an independent unit giving impartial advice to management and employees about the effects of work on health and health on work.
Barnsley Occupational Health and Wellbeing Service
(01226) 434939 or extension 4939
Block 9
Gawber Road
Barnsley
S75 2EP
Opening hours are:
8.30 am - 4.30 pm Monday
– Friday
Out of hours
(an answer machine service is available)
For urgent high risk blood exposure/incident
Where treatment is required, the Emergency
Department should be contacted immediately
Who is in the Occupational Health and Wellbeing Team?
Doctor and Nurses trained in Occupational Health
Moving and Handling Specialist
Specialist Practitioners in Health and Wellbeing
We also work closely with the extended multidisciplinary team e.g. Infection
Control, Physiotherapy, Health and Safety, Genito-urinary Medicine.
Occupational Health and Wellbeing Confidentiality
Staff can refer themselves without their manager’s knowledge.
A manager should refer staff if there is a problem relating to their health at work in line with the Sickness Absence Policy. Advice will be given to the employee and the manager with consent but medical details will remain confidential.
Your records are kept according to the Data Protection Act. No one inside or outside the Trust other than yourself and Occupational Health and
Wellbeing staff can see these records without your written consent.
46
What services do we offer?
Advice on health issues affecting work.
Fitness for work on employment.
Advice on fitness for work and sickness absence, management during employment.
Advice on workplace modification, redeployment or alternative work if appropriate, including rehabilitation, phased return.
Immunisation programme.
Health surveillance programmes e.g. lung function and hearing.
Skin surveillance.
Workplace visits/workstation assessments (VDU).
Policy development.
Moving and Handling Specialist advice incorporating the management of training and risk assessment.
Health and Wellbeing Team. The team supports individuals and teams at work with mental health and stress issues. They provide a proactive approach to managing stress at work, including training, group work and mediation for workplace conflict.
A range of 1:1 treatment therapies are available for staff experiencing mental health, home or work issues. These include Cognitive Behavioural interventions, counselling and EMDR for trauma.
Provision of external services to local business.
Contamination incident management.
Advice and management of infectious diseases.
Physiotherapy Referrals.
The Stress Champion for BHNFT sits in Occupational Health and
Wellbeing and is chair of the Stress Group who promote the cooperation and partnership between Management, Trade Unions, Safety representatives and Employees in the development and implementation of control measures to ensure health, safety and wellbeing of employees who state they are affected by stress issues and support managers indeveloping a SMART action plan based on the results of the HSE
Management Standards questionnaire. The aim being to be pro- active; education is provided to support staff in recognising stress symptoms in self and others and to act appropriatley using services available to prevent escaltion of symptoms.
47
What hazards at work could I be exposed to?
Violence and stress
Exposure to demanding deadlines, work overload, bullying and traumatic incidents may result in physical and emotional distress.
Radiation
Exposure to ionising and non-ionising radiation lasers can result in burns, skin disorders, eye injuries, cancer and other illnesses, although the likelihood is low if following safe working practices.
Musculoskeletal Injury
Causes include excessive work with VDUs, repeated movements, poor posture, excess force, lack of rest periods and poor equipment design.
Lifting heavy loads or improper lifting can cause neck and back injuries.
Effects include other sprains, work related upper limb disorders (WRULD) or repetitive strain injuries.
Hazardous substances and biological agents such as bacteria, viruses and chemicals.
Exposure can result from inhalation, swallowing, splashing into the eyes, absorption through the skin or from accidental inoculation - e.g. contamination incident.
The effects can include poisoning, burns, eye injuries, skin disorders, cancer, and transmission of blood-borne viruses, asthma and other lung diseases.
What is contamination injury?
An injury or splash incident which causes exposure to blood or high-risk body fluids.
What are the risks from contamination incidents?
The main risks from contamination incidents are infections with blood-borne viruses: Hepatitis B, HIV and Hepatitis C.
How can this occur?
Puncture of the skin with a dirty needle or sharp instrument.
Exposure through cuts or breaks in the skin e.g. cuts or skin conditions such as eczema.
Splashes of blood or body fluids in the eye or mouth.
48
Which body fluids are infectious?
High risk
Blood and visibly blood stained body fluids and those derived from blood e.g.
Amniotic fluid
Vaginal secretions
Semen
Breast milk
Cerebrospinal fluid
Peritoneal fluid
Saliva in association with dentistry
Unfixed tissues and organs and synovial fluid
Low risk
Urine
Vomit
Saliva
Faeces with no visible blood staining
If I have a contamination injury what should I do?
1 First Aid - encourage the wound to bleed but do not suck it . Wash thoroughly with warm soapy water and cover with a waterproof dressing - do not scrub . For splashes in the eye remove contact lens if worn, wash immediately with large amounts of eye wash solution (or tap water) for at least five minutes. Rinse nose and mouth if affected.
2 Report and assess the injury/incident —with your supervisor or manager.
Use Contamination Incident Pack located in your area. Determine if risk of transmission of BBV is significant and complete an accident form.
3 Seek advice from Occupational Health and Wellbeing Service during working hours or as soon as next open (unless high risk).
What will Occupational Health and Wellbeing do?
Record details of the incident.
Ascertain the infectious status of the source patient/assess risk/advise blood sample to be taken with source patient’s consent.
Check the immune status of the health care worker and take blood sample for storage and testing if required.
Provide appropriate treatment to minimise the risk of infection.
Offer support and counselling in conjunction with GU Medicine.
49
What if Occupational Health and Wellbeing is closed?
Contact Emergency Department for high-risk incidents (a high risk injury from a high risk source patient). You will need to attend immediately and have details of the source patient available (name, location etc.)
Otherwise the Occupational Health and Wellbeing Service can be contacted the next working day.
50
CONTAMINATION INJURY OCCURRED
First Aid
Assess injury in conjunction with manager
(use the Contamination Incident Pack located in your area)
OH (high risk only ED out of hours), can assist with Risk Assessment
High risk of contamination
Source patient known
Source patient unknown
Source patient assessed for level of risk for BBV by clinician or senior qualified professional
High risk assessment
ED/GU Medicine informed that a member of staff has sustained a high risk injury from a high risk patient post exposure prophylaxis considered
Complete accident form with manager
Source patient approached by competent
Low risk of contamination
Low risk assessment
Seek advice from OH
(Mon
– Fri 8.30 – 4.30)
Complete accident form with manager
OH will check your immune status and take a blood sample for storage and testing if required person (GU Medicine or Public Health)
))Nurse) to consent for blood test for BBV
51
Workplace Mediation and Harassment Advice
Workplace mediators are members of staff who have been trained in facilitating the mediation process for employees who are experiencing workplace conflict.
What is mediation?
Mediation offers a way of resolving interpersonal conflicts; misunderstandings and disagreements at work in a way that encourages clearer communication, good working relationships and an emphasis on solutions. Mediation is voluntary which means all parties involved must agree to the mediation and be willing to look for a resolution. The process is confidential and the mediator remains impartial throughout the process.
An information leaflet is available from Occupational Health.
Please contact Heather Howard on ext 4939 or any adviser or mediator for more information.
No place for harassment, bullying or conflict at work
In this leaflet you’ll find information on harassment, bullying, and workplace conflict and how to get help.
Read on to find out who you can talk to and where you can get more help and advice.
Act now and get it sorted!
52
What is Harassment?
Generally, harassment is any unwanted behaviour that can cause offence, hurt and humiliation. It is unwanted behaviour that can make you feel uncomfortable, embarrassed, unsafe, threatened or frightened.
Is it against the law?
Yes, some forms of harassment are against the law. These include harassment because of your sex, sexual orientation, colour, ethnic origin, nationality, disability and/or your religion/belief.
What is bullying?
Often persistent, it is threatening, abusive, malicious intimidating, belittling or insulting behaviour directed at an individual or a group. It can undermine the confidence and self-esteem of the person it is aimed at.
The Trust’s Policy for Challenging Bullying and Harassment in the Workplace
Do you feel you are being bullied or harassed? Please read the Trust Policy which advises what you can do. A copy of the full policy can be obtained in each department and on the intranet.
First Steps
Have you asked the person to stop what they are doing? You can do this through a meeting or in writing. A trade union representative can accompany you or help you to write a letter
Have you discussed the problem with your manager? Contact a harassment advisor to talk through your options
Harassment Advisers
Harassment Advisers are specially trained staff members who work in different roles and locations within the Trust. Advisers are a good first point of contact if you need advice, support or help to deal with harassment or bullying, their advice is impartial and confidential.
The role of the Harassment Advisers is to:
Provide assistance to employees with complaints of harassment and bullying
Explain to them how the procedures for making a complaint operate, informal and formal
Establish the main details of any complaint
Channel the complaint to the appropriate manager for action if the employee decides to take the matter further
53
HARASSMENT ADVISER CONTACT LIST
Harassment Advisers are specially trained staff members who work in different roles and locations within the Trust. Advisers are a good first point of contact if you need advice, support or help to deal with harassment or bullying. Their advice is impartial and confidential.
The role of Harassment Advisers is to:
Provide assistance to employees with complaints of harassment and bullying
Explain to them how the procedures for making a complaint operate, informal or formal
Establish the main details of any complaint
Channel the complaint to the appropriate manager for action if the employee decides to take the matter further
Debby Horbury deborah.horbury@nhs.net
Ext: 4361
I am a matron working within the surgical divisional team and have worked as a nurse in Barnsley since leaving school. The main function of my role as a
Matron is to ensure that the patient’s experience of our service is a good one, paying particular attention to the environment, infection control issues, standards of care and treating patients with dignity and respect. I have long held an interest in staff welfare and wellbeing and believe that as nurses we also have a duty of care for our colleagues.
Kay Churnside kay.churnside@nhs.net
Ext: 2744/2850
I am employed as a Sister in ITU, and have worked at BHNFT since 1987. I have experience in dealing with people especially in difficult situations. I have experienced bullying and harassment, so know how this can affect you. The lack of support networks at this time prompted me to become involved in this service to help others.
Karen Ross karenross@nhs.net
Ext: 2700
My job role is MDT Co-ordinator for Cancer Services and I am currently based on Ward 36. My hours of work are Monday, Tuesday and Wednesday.
Dawn Elsegood dawn.elsegood@nhs.net
Ext: 2996
I work in Risk Management as a Quality Co-ordination Assistant dealing with personal injury claims, formal complaints and Incident Report Forms (IR1’s).
My daily duties involve dealing with solicitors and complainants over the telephone and meeting face to face if necessary.
John Kitching jkitching@nhs.net
Ext: 2683
Some people know me by my nickname, which is Kitch. I have worked in
Barnsley Theatres for the past nineteen years my job title is Operating
Department Orderly. I also work as a Trade Union Rep for GMB and have supported staff who are experiencing bullying and harassment.
54
Vikki Redhall v.redhall@nhs.net
Ext: 2808
I have worked both in HR and at the Hospital since leaving school in 1996.
I am now a HR Officer, I deal with a variety of issues such as Disciplinary,
Grievance and Performance. I have had experience of dealing with staff who have been subject to bullying or harassment in the workplace and those who have been accused. The role of the Harassment Support Worker will enable me to provide staff with confidential and independent support on this issue.
Heather Howard heatherhoward@nhs.net
Ext: 4939
I work as a Mental Health Practitioner in Occupational Health. My role commenced in February 2007 and involves supporting staff experiencing mental health problems through early intervention and preventative work, including anxiety and depression management based on Cognitive
Behavioural techniques. My role also covers crisis intervention, education, facilitating teams, group-work, liaison with community mental health services, policy work, auditing of referrals and advice to other members of the
Occupational Health Team. I am interested in all aspects of supporting staff in the workplace, and believe that harassment at work has a detrimental effect on mental health.
55
OCCUPATIONAL HEALTH SERVICE
WORKPLACE MEDIATION HANDOUT
What is workplace mediation?
Mediation offers a way of resolving interpersonal conflicts; misunderstandings and disagreements at work in a way that encourages clearer communication, good working relationships and an emphasis on solutions. Mediation is voluntary which means all parties involved must agree to the mediation and be willing to look for a resolution.
Mediation is a confidential process where an impartial person
– the mediator – works with people who have a disagreement, dispute or conflict at work, to help them find their own solution and reach an agreement that will improve the situation. The process usually starts by talking to each of the people involved in the dispute separately, and then, later on, a joint meeting with both parties. It is a highly structured process so that both parties have the chance to speak without interruption to discuss how they would like to improve things in the future. The parties themselves come up with and agree a voluntary solution, which is documented at the end of the process.
Why should I choose mediation?
Conflict can cause stress at home and work, mediation can help resolve your disagreement so you can get on with your normal life again.
It is less costly than disciplinary procedures (in all senses of the word i.e. sickness and absence, the loss of experienced staff, negative staff morale, poor decision making and emotional stress).
When you are involved in a conflict, talking to the person you are in disagreement with can seem impossible. Mediation can re-establish those channels of communication.
The process culminates in a written agreement on your terms, which is not dictated by someone else. It isn’t legally binding but allows both parties to draw a line under the dispute and move forward.
It is totally confidential- nothing you disclose will be passed on to anyone else including your line manager unless you want it to be.
Notes will be taken by the mediator throughout the process, but these will be destroyed and no details will be kept in your personnel or occupational health file.
When can mediation be used?
Most types of conflict can be mediated, provided that both parties want to find a way forward. It can be used at any stage in a dispute but is often most effective if used early on. In the workplace, mediation is used to resolve issues such as perceived bullying, harassment; discrimination and can unlock any tensions between staff that are having a negative impact on morale.
Do I have to agree to mediation?
No. Mediation is entirely voluntary.
56
What if I am reluctant to be in the same room as the person I am in dispute with?
The mediator will take this into account and will not make you meet with the person unless you agree to. Ground rules will be set with both parties before the joint meeting, to stipulate how everyone will behave and ensure the meeting runs smoothly. You can ask for the joint meeting to be suspended at any time.
How long does it take?
Initial separate meetings will take about one to two hours. The joint meeting may take up to a day to complete, so time must be made available by everyone to go through the process.
Can I be made to keep to an agreement reached in mediation?
You will not be forced to agree to anything so you must be committed to sticking to what is finally agreed, otherwise there is no point in engaging in the mediation process. If an agreement cannot be reached, which can sometimes happen, you can still go on to using workplace procedures such as grievance or disciplinary, but you cannot bring up what has been said in mediation.
How can I access the service?
You can contact any of the workplace mediators for more information.
If you wish to access the service an assessment will be made to ensure the dispute is suitable for mediation.
57
Workplace Mediation Contact List
Workplace mediators are qualified people who can provide support for staff experiencing conflict at work.
What is mediation?
It is a way of resolving interpersonal conflicts ; misunderstandings and disagreements
Mediation is voluntary
The process is confidential
The mediator remains impartial
Your Workplace Mediators are:
Emma Lavery
Heather Howard
2808
4939
Jackie Dickens
Jan Mathieson
Josie Foster
Martin Jackson
4939
3056
2266
07790 146254
58
Irritable; Tense; Worried; Poor sleep; Restless; Anxious; Avoiding doing things?
You may benefit from attending our Stress Control Workshops
Would you like to learn stress control strategies?
The Health and Wellbeing Team are presenting a course of five workshops on stress control over a five week period. Each session, lasting two hours, will cover a different area of stress management (see over for outline of course).
This can be taken as a full course or can be delivered in your department to suit your needs.
You will receive a relaxation CD with plenty of handouts and learn ways to positively handle stress. Personal issues will not need to be discussed in the workshop.
To find out more about the course or to book a place, contact Heather
Howard/Dave Thompson on ext 4936 or email heatherhoward@nhs.net
59
Outline of the Course
Session One: Leaning about stress
We will look at the causes of stress and what keeps it going. We examine the way it affects your thoughts, actions and body. We explore the myths about stress and vulnerability to stress.
Session Two: What keeps stress going and controlling your body –
Relaxation. You will learn about the vicious circle formed by thoughts, actions and body symptoms and how this feeds your stress. You will learn how to use relaxation and be given a CD to keep. You can then practice at home.
Session Three: Controlling your thoughts
– Think your way out of stress
You will learn how stress and thoughts feed each other. You will learn how to complete ‘court case’ diaries to weigh up the evidence for your thoughts to help get them under better control.
Session Four: Controlling your actions – Learn better ways to control your life. You will learn ways to deal with problems in your life by using problem solving.
Session Five: Controlling your sleep, tying the course together and controlling the future. You will learn ways of getting off to sleep and then staying asleep. On the course you will learn to pull together all you have learned. You will see how all the skills fit and how they combine to give you a powerful range of skills. These will help you cope with the future.
60
Healthy Workplace Project
Barnsley Hospital launched the Healthy Workplace Project in 2009, with the intention to improve the physical, mental, emotional and social well being of its employees. A steering group was set up and a wide consultation was done to capture the views of employees, asking what would help them to feel better.
Four core areas were identified and thus 4 sub-groups were formed to develop projects and activities:
Physical Activity
Healthy Eating
Wellbeing & Stress Management
Smoking Cessation
Physical
In order to encourage staff to cycle to work, we launched the Cyclescheme initiative where staff can purchase a bike and accessories through a salary sacrifice scheme. We also offer bike sheds to enable staff to securely store their equipment, and showering facilities are available.
Fitness classes are held every week in the Hospital social club to encourage staff to get active, with the convenience of classes being held on site.
Healthy Eating
Over the course of the last two years the Trust has achieved both the Bronze
Eat Well at Work Award and the Silver Eat Well at work award as a result of work done in partnership between the Healthy Workplace Initiative and ISS.
Starting in January 2011 the Healthy Workplace Initiative has paid for shop space in the Outpatients reception to enable a local fruit and vegetable trader from Barnsley Market to attend and sell quality fruit and vegetables to patients and staff. This initiative whilst relatively low cost has had a significant impact resulting in positive advertising in the local press and excellent feedback from staff.
Wellbeing & Stress Management
The Trust has provided a series of stress control workshops aimed at helping employees to recognise and manage their own stress. The course consists of a series of five sessions which are two hours long each and are based on
Cognitive Behavioural Therapy techniques. Participants are helped to learn ways to control problems such as anxiety, poor sleep, anger and improving self-confidence. (Further detail and statistics relating to these workshops can be provided via an evaluation report carried out by the wellbeing team)
Smoking Cessation
The smoking cessation service has been supporting staff on site since
December 2008 and already has in place a number of incentives to encourage staff to access support and maintain their smoke free status.
These are accessible through the hospital based service or the town centre base on Eldon Street:
61
Free Nicotine Replacement Products
Protected time to attend support sessions
For further information on Healthy Workplace activities please contact Chris
Barton on ext 2288 or email cbarton1@nhs.net
62
Trade Union and Staff Side Information
The following Trade Unions are recognised by the Trust:
Union
UNISON
Secretary/Representative
Liz Mawson
GMB
Contact Details
07867454680/01226
299607
07790146254 Martin Jackson
Dave Myring
Lynn Parkinson
Ext 2450/07515777846
Ext 2506
UNITE
Royal College of
Nursing
College of
Radiographers
Royal College of
Midwives
Pat Young
Julie Rear-Barton
Ext 2832
432005/432249
CSP Joanne Bleasdale 432641
Further information can be obtained by contacting the above representatives
63
64
Desktop Counter Fraud Guide
65
Section 9
Appendices
APPENDIX ‘1’
MANDATORY TRAINING WEEK DATES 2013
2013
January
February
March
April
May
June
Week commencing 14 th
Week commencing 11 th
Week commencing 11 th
Week commencing 8 th
Week commencing 13 th
Week commencing 10 th
July Week commencing 8 th
August
September
Week commencing 12 th
Week commencing 9 th
Week commencing 7 th October
November Week commencing 4 th
December Week commencing 2 nd
Please note that not all mandatory training sessions are run during these dates but spread out throughout each month
66
Appendix 2
Corporate Induction
Local Induction
Fire Health & Safety
SUBJECT
Immediate Life Support Update
Mandatory and Statutory Training Delivery - 2013
5 Day Programme - W/C: 14 Jan, 11 Feb, 11 Mar, 8 Apr, 13 May, 10 Jun, 8 Jul, 12 Aug, 9 Sept, 7 October, 4 Nov, 2 Dec
3 Day Programme – W/C 28 Jan, 25 Feb, 25 Mar, 22 Apr, 24 Jun, 22 Jul, 23 Sept, 21 Oct, 18 Nov, 16 Dec.
E-learning available
MONDAY TUESDAY WEDNESDAY
N/A 9.00 – 11.00
2 hours delivered by line manager locally
√ 2.00 – 3.00 10.00 – 11.00
N/A 1.00 – 4.30
2.30 – 3.30
THURSDAY
1.00 – 4.30
Basic Life Support
Infection Control and Hand Hygiene (non-clinical)
Infection Control and Hand Hygiene (clinical)
Major Incidents & Emerging Incidents
Moving and Handling Theory
Moving and Handling Practical
Conflict Resolution
Equality & Diversity
Safeguarding Adults
Safeguarding Children Basic Awareness (patient contact)
N/A
√
11.00 – 12.00
3.00 – 4.00
9.00 – 10.00
9.00 – 10.00
12.30 – 1.30
√
E-Learning Only
√
10.15 – 11.45
N/A
√
9.00 – 10.45
11.00 – 12.45
11.15 – 12.15
9.00 – 10.45
1.15 – 3.00
Please refer to the link on the Learning & Development webpage
√ 12.45 – 1.45
1.45 – 4.15
12.30 – 1.30
10.00 – 11.45
2.00 – 3.45
√ 9.00-10.45
Safeguarding Children Basic Awareness (non-patient contact) Awareness Leaflet
Information Governance √
Fraud √
1.00– 1.45
10.45-11.00
10.15 – 11.45
9.00 – 10.00
10.15 – 12.00
FRIDAY
9.00 – 12.30
1.30 – 2.30
67