AHT HOME - Anderson Hand Therapy
advertisement

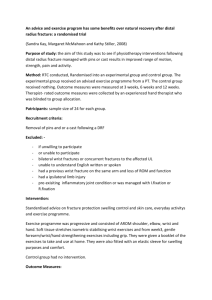
AHT HOME At Anderson Hand Therapy we recognise that work oriented programs are a vital component of hand-therapy. Goal oriented tasks are the ultimate treatment tool to restore range of motion, strength, and co-ordination. Work hardening and conditioning achieved with individual and activity focussed treatment plans, is integral to how we work with our patients and essential to a rapid, successful return to work. TREATMENT IONTOPHORESIS Iontophoresis is a treatment modality which administers an anti-inflammatory agent at the injury site using medicated electrodes. The medication is driven into the area using electrical stimulation. It is a therapeutic substitute for cortisone injection where cortisone is inappropriate. Advantages over cortisone include: Non invasive drug entry into skin and underlying tissue. No associated pain No long term joint or tissue damage Controlled and slower rate of administration Iontophoresis has been demonstrated to be most effective when used in conjunction with traditional modalities to provide immediate relief of symptoms (1). When treating patients with inflammatory conditions, eg tendonitis, carpal tunnel syndrome, or tennis elbow, our experience indicates the best results are obtained treating acute conditions. Scar, however, is likely to respond favourably when treated months post surgery. Please call us on 0413 426 474 if you feel a trial of iontophoresis may benefit your patients. (1) Gudeman, S.D. American Journal of Sports Medicine 25 ( ULTRASOUND This treatment modality is the use of high frequency acoustic energy used in rehabilitation to promote tissue healing, reduce pain and restore mobility. Low intensity ultrasound is used to : Control inflammation Control oedema Enhance healing Higher intensities are used as a heating agent to: Reduce pain Reduce stiffness Improve tissue extensibility Ultrasound can also be used in the softening of scar tissue by changing the pattern of collagen fibres and by increasing circulation. Most studies with ultrasound have looked at its use in the treatment of epicondylitis and do indicate that it may be effective as part of a total treatment plan. However there is little support for Ultrasound at any intensity when used on its own without other therapeutic intervention. There also does not appear to be any good clinical evidence to show that ultrasound assists in the delivery of topically applied medicines such as hydrocortisone, a technique known as phonophoresis. Subjective reports from patients we have seen, do however indicate that topical creams such as “Voltaren” are felt more intensely when applied pre pulsed Ultrasound treatment. If you would like more information on Ultrasound or would like to organise a trial for your patient, call Hamish on 0413 426 474. THERAPEUTIC HEAT Heat is used to reduce pain, decrease joint stiffness and improve local circulation. Studies have shown that heated connective tissue will retain elongation achieved in therapy better than tissue that does not receive heat treatment. Heat should not be used during inflammatory phases, and fragile skin should be checked frequently during application. Patients with cognitive deficits should be supervised with any heat modality. Two of the simplest methods are paraffin wax baths, and heat packs or wheat bags. The latter are effective, cheap, easy to use, and can be quickly heated in a microwave. Paraffin wax is an extremely popular treatment with arthritic patients and home units are available. A picture of such a unit is shown here. Home units range from $50 to $250. TENS Transcutaneous Electrical Nerve Stimulation (TENS) is a commonly used method of pain control, which is explained by 1) the gate control theory and 2) the release of endogenous opiates. Indications: Acute pain relief Chronic pain or C.R.P.S. (R.S.D.) Post-operative pain Contraindications: Cardiac pacemakers Poor patient cooperation / understanding SPLINTS SPLINTING THE THUMB Injuries to the base of the thumb are many and varied, ranging from a significant Bennets fracture, to a grade one ligamentous strain, to an arthritic condition. Unfortunately the demands that functional tasks such as writing, or holding a golf club place on this joint mean that recovery, even from a mild injury can be slow and painful. Splinting the joint provides it with support and pain relief, whilst not interfering with daily tasks. The splint can be made of thermoplastic or neoprene, depending on the degree of support the patients function or the nature of the injury requires. Many simple, different patterns can be employed enabling thumb splints to be used in sports, at the workplace, or at home. CONDITIONS DISTAL RADIUS FRACTURES Distal radius fractures have been estimated to account for one sixth of all fractures seen in emergency rooms. Of these, the Colles fracture with its distal displacement of the distal fragment and associated comminution is the most common. They are more frequently seen in women, increase with age and often occur from low energy falls. When possible therapy should be initiated even with the wrist immobilised. Goals are to regain or maintain elbow, shoulder motion and to address any difficulties with finger or thumb motion by the time the wrist can be moved. Oedema control and pain management are vital, as is patient education and compliance. “It is a poor prognosistic sign if problems with oedema, pain and ROM of the uninvolved joints have not been resolved by the time the wrist is ready to be mobilised”(1) Maximum functional recovery often occurs after bone union has been activated and therapy has been stopped. Stable fractures can take up to 6 months and complex, intraticular fractures from 1—2 years to achieve a good functional outcome. (1) Lascter, G.F.: Therapeutic Management of Distal Radius Fractures. In Hunter, J. et al editors: Rehabilitation of the Hand, ed 5, St Louis Mosby, 2002 . ARTHRITIS: JOINT PROTECTION Seven basic principles that can be applied to everyday activities so as to reduce stress and pain to affected joints. 1. Respect your pain and avoid non-essential tasks that aggrevate your pain. 2. Take regular, short breaks during an activity. 3. Reduce the amount of effort required to do a task ie. Change how you do the task or use adaptive equipment. 4. Use the largest and strongest joints available for a task. 5. Maintain muscle strength and joint range of motion. 6. Avoid static positioning of joints. 7. Use each joint in its most stable position and functional plane. These principles are applicable to the whole body, not just the hand and are especially important for those patients with inflammatory conditions. CASE STUDIES CASE STUDY #1 John has been a plasterer for 25 years. His job entails long hours of holding a trowel in his right hand and applying the plaster with a repetitive action, constantly deviating his wrist under load. He developed a chronic ache with ulnar deviation that he never sought treatment for. Discussing the demands of the job with John, it became apparent that he might benefit from a splint that restricted end range ulnar deviation, yet still allowed him to hold a trowel, move his wrist, and carry heavy items. The splint is pictured below. John has been using it for 8 months now, and he has been able to complete all the tasks required of him without discomfort. CASE STUDY #2 Miss S is a legal secretary who presented with the complaint of extensor forearm pain. Her work required a medium level of repetition with continual static exertions. Miss S also reported chronic neck and low back pain for which she had been receiving fortnightly chiropractic intervention for three years. It became apparent quickly that although soft tissue treatment and graduated strengthening would be valuable, they would not be the complete answer. An ergonomic assessment was completed. Recommendations included adjusting the position of Miss S’s monitor, altering the style of her workstation, and the provision of a phone headset. Miss S was compliant with her work conditioning program and was subsequently discharged from Hand Therapy five weeks after her initial visit. A follow up call at four months revealed that she was no longer requiring chiropractic adjustments. CASE STUDY #3 Mrs R has worked in a commercial kitchen for 15 years. Three months ago she had bilateral carpal tunnel releases. Incorporated into the standard rehabilitation of scar management and nerve gliding were activities that mimicked her work duties. We began this process of work hardening despite Mrs R reporting scar hypersensitivity and weakness. The functional hand use was relevant to Mrs R and gave her realistic expectations of her ability to return to work. We completed a worksite evaluation prior to Mrs R’s return to work, and were able to cease rehabilitation at seven weeks post surgery, just prior to her return to full duties. RESEARCH Below is a selection of abstracts of presentations made by AHT over the past 5 years. Research is an essential part of AHT, and all aspects of our treatment are evidence based. GOLF GRIP RESEARCH Adapting the golf club grip to address hand pain and injury. Ben Hogan, winner of over 60 USPGA titles, famously insisted upon the following maxim; “Good golf begins with a good grip”. But what happens when a good grip is not possible due to hand injury or joint degeneration? Golf professionals often recommend the golfer build up the handles of their clubs to address impaired grip, however, there is no research to support such a grip’s efficacy, and the benefit of such an adaption remain anecdotal. The purpose of my research, then, is to examine the potential that golf grips with larger diameters have in reducing the joint stress and associated pain experienced by golfers with pathological hand conditions. I intend to review the biomechanics of the hand and wrist in a standard golf grip, and examine how these biomechanics may change as the club handle is altered. Current grip options will be discussed and compared with customised, built up grips. DIGITAL REPLANTATION VS AMPUTATION Early studies on replantation were interested in the survival of the digit. More recent studies have focussed on the function of replanted fingers. There have been no studies performed comparing functional outcomes of single replanted digits to amputated digits at the same level. Objective: The aim of this project is to compare the functional outcomes of patient post microsurgical replant of a digit to those who had undergone terminalisation of an amputated digit at a similar level and from a similar mechanism of amputation. Method: This is a retrospective study. The subjects were all patients who had been managed through The Plastics Unit at St. Vincent’s Hospital Melbourne over the last two to ten years. Patients who had undergone microsurgical replant were matched with subjects with injuries of the same finger and similar level but which had been terminalised. This study used standardised functional questionnaires including the DASH and the Michigan Hand Outcomes Questionnaire. The Jebsen Test of Hand Function was also used. Objective measures of ROM, grip and pinch strength, and sensation using the Semmes Weinstein Monofilaments and two-point discrimination were also measured. Results from patients with replanted fingers were compared to the results of patients who had had terminalisation of the same digit at a similar level. Results: Raw data is still being collected. Preliminary results indicate that subjective assessments of function, and overall satisfaction are much higher in the replantation group. This study remains ongoing, and data analysis will focus on comparison of scores on the primary independent variables. SPLINTING FOR SPORTS COACHES FINGER; FIVE SPLINTS TO PROTECT AN INJURED HAND AND PREVENT LONG TERM DEFORMITY McCue established the term "coaches finger" for an on-field finger injury that receives no treatment, but has significant consequences (McCue 1974). When accurate diagnosis with early intervention is not initiated, what first appeared to be an innocuous injury becomes complicated, and treatment is often unsuccessful (McCue, 1974). Conversely, prompt intervention can result in no residual deformity or recurrence of injury (Palmer, 1978). Five simple hand splints that protect healing injuries or fractures during play will be presented. Each design will be discussed along with the diagnoses they protect. Two of the five splints are designed for the thumb, the other three are for phalangeal or metacarpal protection. The designs are custom made, low profile, and fabricated from low temperature, lightweight thermoplastic and/or neoprene. Variations in taping, attachment and padding will also be addressed. Each splint design has been trialled and refined on both professional and amateur athletes. The goal of splinting these injuries has been to return the athlete to their sport as quickly and safely as possible. In many cases, the footballer can immediately return to training or play with the protective splint in place. McCue FC (1974). The coaches finger. Journal Of Sports Medicine, 2(5) 270-275 Palmer RE (1978) Sports Casting of the In-season Athelete. Peoria, Illinois SPLINT DESIGN THE DART THROWER’S MOTION; CAN SPLINTING ENCOURAGE EARLY MOBILISATION? Several recent studies as well as opinions expressed at the recent International Hand Surgery and Therapy Congress in March of this year have indicated that early mobilisation of the wrist post surgery may be best in the dart thrower’s plane, that is from wrist extension and radial deviation, to wrist flexion and ulnar deviation.(1,2) This theory is based upon carpal kinematic studies that suggest that this direction is unique in the radiocarpal joint stability it creates, with scaphoid and lunate motion approaching zero along the dart thrower’s path.(1,2) Whilst conclusions in these studies might recommend early mobilisation or new rehabilitation protocols based, there is little to be found that supports their results clinically. If the patient needs to be restricted to the dart throwers motion, then instruction alone is unlikely to be sufficient. This presentation will review the relevant carpal kinematics, discuss rehabilitation options, and introduce prototypes of splints specifically designed to limit motion in the above plane. (1) Crisco, J. et al. In Vivo Radiocarpal Kinematics and the Dart Thrower’s Motion. Journal of Bone and Joint Surgery, 87A(12), Dec 2005 (2) Werner, F. et al. Scaphoid and Lunate Motion During a Wrist Dart Throw Motion. Journal of Hand Surgery, 29A(3), May 2004 JOURNAL REVIEW Splinting in the Treatment of Arthritis of the First Carpometacarpal Joint. Swigart, CR., Eaton, RG., Glickel, SZ., Johnson, C. The Journal of Hand Surgery, Vol 24A No. 1 January 1999. This was an interesting retrospective study, ostensibly written to redress the imbalance between research into surgical options for CMC arthritis, and conservative treatment like splinting. A total of 130 thumbs were included, in varying stages of disease. Splints that immobilised the CMC joint and restricted wrist motion were fabricated. Response to splinting was recorded shortly after splinting, and at a 6 month follow-up. 62% of patients who replied to the follow-up questionnaire re function, reported some relief of symptoms with splinting. Those patients with initially less severe symptoms were more likely to report improvement. The study lacked a control group, and from a rehabilitation perspective, an objective functional measure would have been useful. The splint used, although custom-made, appeared cumbersome, and perhaps larger than necessary to immobilise the CMC joint. A similar study that the researchers did refer to, used a smaller “short opponens” type splint, and had similar success in forestalling, and even eliminating the need for surgery. Ultimately, the researchers conclusion supported splinting as a conservative option at least as initial treatment, and certainly for early stage CMC arthritis. From our perspective, splints whether soft, prefabricated, or custom can definitely benefit the arthritic patient to maintain independence. Carpal Tunnel Syndrome and Pregnancy Courts, RB: Splinting for symptoms of carpal tunnel syndrome during pregnancy. Journal of Hand Therapy 8(1)31-34, 1995. Carpal tunnel syndrome (CTS) is a compression of the median nerve at the wrist. It was first described in pregnancy in 1945, is usually diagnosed in the third trimester, and has a reported incidence in pregnant women from 1-50%. Courts (1995), attempted to determine whether splints were effective in reducing symptoms in this population. His study consisted of a case series of 82 pregnant women, with a total of 135 hands diagnosed with carpal tunnel syndrome. Eight subjective symptoms were assessed, along with grip and pinch strengths. Data was taken prior to intervention, one week after splinting, and one month post-partum. The women did not receive any other treatment or therapy for their symptoms. After one week of splinting, a significant number of participants reported a decrease in their symptoms. At the conclusion of the study, 76% of participants had complete resolution. The weakness of this study is its lack of a control group. His findings however are very much in keeping with similar research. Wrist splinting and education on wrist positioning has been shown to be an effective way of limiting the discomfort and impaired function that is associated with CTS.