Gastric Outflow Obstruction
advertisement

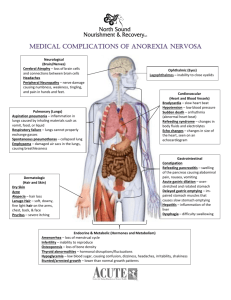
Gastric Outflow Obstruction R. M. Bright Department of Clinical Sciences, College of Veterinary Medicine & Biomedical Sciences, Colorado State University, Fort Collins, CO 80523, USA The stomach is an unequal dilatation of the foregut, which extends as a J-shaped loop from below the esophagus and diaphragm in the upper left abdominal quadrant to the duodenum in the upper right quadrant. The greater curvature of the stomach, facing caudally, is located mostly to the left of the midline. The lesser curvature faces cranially and is accentuated when the stomach is empty. The distal stomach is somewhat immobilized by the hepatogastric and hepatoduodenal ligaments. Within these structures are the common bile duct, the hepatic ducts, and the portal vein. The stomach is divisible into four parts. The cardia is immediately distal to the gastroesophageal junction below the diaphragm. It blends into the fundus, which provides receptacle and storage functions and, along with the body, is the most expandable portion of the stomach. The cardia, body, and fundus comprise approximately two thirds of the proximal stomach. The fundus and body are histologically indistinguishable from each other. The pyloric antrum forms the remaining third of the stomach and leads into the pyloric sphincter. The mucosa of the body and fundus is rugose. The mucosa-submucosa are loosely attached to the underlying muscle, making it somewhat mobile. The antral mucosa contains fewer rugal folds and is flatter. The mucosa-submucosa are more firmly attached to the underlying muscle. When the stomach is empty, the rugal folds are most distinct. The muscle layers of the stomach contain an outer layer of longitudinally arranged muscle fibers, an oblique layer, and deep to this are circularly arranged muscle fibers. The latter are plentiful in the antrum because of its important function of grinding, retropulsing, and emptying of gastric contents. The pylorus is a thickened continuation of the circular smooth muscle, which, along with its mucosal lining, forms an intraluminal bulge that can be palpated. The pylorus is considered a true antatomic sphincter owing to these abundant circular muscle fibers that encircle it. The blood supply to the stomach is by way of the celiac artery and some of its branches. The left and right gastroepiploic arteries primarily nourish the greater curvature, whereas the lesser curvature is supplied by the right and left gastric arteries, which eventually anastomose. Venous drainage is accomplished by the gastrosplenic and gastroduodenal veins emptying into the portal vein. The proximal stomach serves a reservoir function and expands greatly in response to liquid and food. "Receptive relaxation" of the fundus and body of the stomach is induced when the animal swallows, resulting in decreased motor activity and pressure. Gastric accommodation follows as pressure begins to increase within the fundus. The primary role of the fundus is to empty liquids without allowing any modest change in the pressure within the fundus to raise intragastric pressure. Partial or complete removal of the fundus will raise the intragastric pressure more readily, however, resulting in an increased rate of emptying of liquids. This has no effect on the rate of emptying solids. 1 The distal stomach is primarily responsible for grinding, filtering, and propelling solid food until it reaches a particle size of 1 to 2 mm in diameter. Even after antrectomy, up to 60% of emptied particles are smaller than 1 mm. In the fed state, peristaltic waves occur at a rate of 4 to 5 per minute, which helps propel the food toward the pylorus. The pylorus, as a "gate-keeper," is responsible for keeping material in the stomach until it reaches the appropriate particle size. When the smaller particles begin to move aborally, the pylorus is partially relaxed and emptying occurs. Near the end of each antral contraction, the pylorus closes, forcing the larger particles to be retropulsed back into the antrum and body of the stomach so grinding can continue. In the fasted state, the stomach and intestine alternate between quiescent time and short times of intense myoelectrical activity. This results in vigorous aboral contractions and forms the migrating motor complexes, which extend through the entire intestinal tract. In the dog, this occurs every 2 to 3 hours. This is the period when nondigestable materials and cellular debris move out of the stomach. Antral contractions are stronger during the fed state and when relaxation of the pylorus is at its maximum. The pylorus, besides regulating the size of particles that leave the stomach, is also responsible for limiting the amount of duodenogastric reflux. It is known in dogs that bile, pancreatic juice, and intestinal contents have a deleterious effect on the gastric mucosa. The amount of duodenal material inside the stomach depends on the rate and volume of duodenogastric reflux and the rate at which regurgitated material is removed from the stomach. Duodenogastric reflux is a common phenomenon and is not affected by the type of. However, if gastric emptying is delayed, the reflux rate is stimulated, which may result in an erosive gastritis or ulcer formation. Similarly, when surgery of the pyloric sphincter or resection of the pylorus has occurred, the reflux of bile and pancreatic and intestinal secretions may increase. These secretions may be innocuous in some animals, but in others, reflux gastritis or bilious vomiting may occur. This is termed postoperative alkaline reflux gastritis. Gastric outflow obstruction is most often caused by mural, mucosal, and luminal abnormalities. Foreign bodies can produce either partial or complete obstruction as can inflammatory diseases caused by eosinophilic gastritis, fungal gastritis, chronic gastric ulcer disease, and neoplasia, most notably, adenocarcinoma. Suture-induced granuloma following pyloric surgery has also been reported. Gastric volvulus, seen primarily in large or giant breeds, can result in outflow problems as well. Vomiting is the most frequent sign seen with gastric outlet problems. The normal stomach is usually empty within 8 to 10 hours after eating. Vomiting after this time suggests a gastric retention disorder. The content of the vomitus may be bile and mucus when vomiting occurs on an empty stomach. This may suggest a duodenogastric reflux problem or gastric hypomotility. Conversely, in the absence of bile, the presence of nondigested material 12 to 24 hours after eating would suggest an outflow obstruction problem. 2 Pyloric Stenosis (Congenital) This condition is primarily seen in brachycephalic breeds and in the Siamese cat. This stenosis results from hypertrophy of the circular smooth muscle of the pylorus. Signs are usually not seen in the first 6 to 8 weeks of age. They appear when the animals are weaned and begin to take solid food. The difficulty of emptying solid food is the hallmark of this disease. Gastrin and its effects on the smooth muscle of the pylorus have been implicated but the mode of inheritance and exact pathogenesis are unknown. Pentagastrin, a gastrin analogue, has been given to pregnant animals, resulting in pyloric stenosis in the neonate as a result of hypertrophy of the muscle. Surgery is necessary to correct this problem. Pyloromyotomy carries little risk and is accompanied by good results. Acquired Antral Pyloric Gastropathy The acquired form of antral pyloric stenosis usually results from dramatic hypertrophic changes to the mucosa and, occasionally, to the circular smooth muscle as well. Type I hypertrophy involves the muscle; type II, the combination of muscle and mucosa; and type III, the mucosa. Benign inflammatory infiltrates are commonly seen on biopsy samples. Grossly, these masses can resemble polyps. They can be smooth-surfaced or slightly lobulated. Some are somewhat sessile and can be single or multiple and confined to the antrum. This acquired form of hypertrophy is typically seen in middle-aged small breeds, in which progressive vomiting is the most common clinical manifestation. The vomiting can be delayed up to 24 hours after eating, and it is not uncommon to see the absence of bile and undigested food in the vomitus. Melena and/or hematemesis would indicate erosive gastritis or ulcer disease that can also contribute to gastric emptying delays. The treatment of choice is some type of pyloroplasty with resection of the hypertrophied polypoid-like masses. The prognosis following surgery is good, with early return to normal gastric emptying. Any hypomotility that persists will usually respond to short-term use of a prokinetic agent. Bilious vomiting following surgery may indicate an excessive amount of duodenogastric reflux caused by the pyloric operation. Sucralfate (Carafate, Hoechst Marion Roussel), systemic antacids and feeding a small meal before bedtime may be necessary on a short-term basis or indefinitely. Neoplasia Gastric neoplasia is rare in the dog and no cause is known. Adenocarcinoma is the most common malignant tumor in dogs and it can manifest as an ulcerated mass, polypoid in appearance or scirrhous in nature. Other gastric tumors include lymphosarcoma, (most common in cats), leiomyoma/sarcoma, and adenomatous polyps. Any of the gastric tumors can cause partial or complete gastric outflow obstruction). They can also result in gastric ulceration or altered gastric motility. 3 As is typical of any mass obstructing gastric outflow, progressive vomiting is the predominant sign. Hematemesis and melena are commonly seen with adenocarcinomas owing to their frequent ulceration. Foreign Bodies Foreign bodies are the most common cause of gastric outlet obstruction in dogs and cats. Vomiting is the sign most often observed and, if the foreign body is sharp-edged, hematemesis may be seen. Many foreign bodies can pass through the pylorus during the interdigestive period owing to the migrating motor complexes. Ideally, foreign bodies can be retrieved by means of endoscopy, with surgery serving as a viable option if this is not possible. Miscellaneous Other causes of chronic intermittent vomiting include granulomatous conditions caused by Phythium and rarely, eosinophilic gastritis. Fungal diseases are most commonly seen in the Gulf Coast states, affecting primarily male large-breed and younger dogs. The granulomas that form in the submucosa and muscularis mucosae are caused by the penetration of ingested spores that eventually enter the lymphatics. Eosinophilic gastritis can stimulate a large amount of granulation tissue to be formed anywhere in the stomach. If this lesion is large enough and present in the antrum, it can cause serious gastric emptying problems. This disease may be immune. These granulomas, when viewed grossly with endoscopy or during surgery, are indistinguishable from neoplastic lesions. Extraluminal lesions can encroach on the antrum and, therefore, interfere with gastric emptying. Ultrasonography is usually helpful in distinguishing these lesions from intraluminal ones. Depending on the origin of the mass, systemic involvement may also occur. Important causes of gastric emptying problems that can be confused with some type of mechanical obstruction are motility disorders. This is not well documented in dogs and cats and the diagnosis is usually made based on delayed gastric emptying in the absence of an obstructive lesion. Trichobezoars in cats may be caused by the lack of migrating motor complexes. Emptying of any type of foreign material in the stomach of a cat, therefore, may be. Hypomotility disorder may occur in dogs that have survived an acute gastric-dilatationvolvulus episode. This may be associated with a large and flaccid stomach, which has been observed during acute gastric-dilatation-volvulus surgery. The vomiting associated with this is presumed to be related to delayed gastric emptying because response to a prokinetic agent is favorable. Long-term use of a prokinetic agent may be necessary in some instances. Metabolic problems, although not as well documented in animals as in people, may delay gastric emptying. These include hypokalemia, diabetes mellitus, hypothyroidism, uremia, and hepatic encephalopathy. 4 Perioperative Considerations Regardless of the cause of gastric outflow obstruction, serious metabolic consequences can result from chronic and frequent vomiting that may accompany a gastric emptying disorder. Dehydration and metabolic alkalosis with its accompanying electrolyte imbalances (hypochloremia, hypokalemia) should be corrected when possible before any surgical intervention. A large, distended, fluid-filled stomach can present a serious risk to any animal undergoing anesthesia and/or surgery. These animals are at a greater risk of gastroesophageal reflux that could lead to an aspiration pneumonia or reflux esophagitis. Immediately after induction of anesthesia, an orogastric tube with a suction device attached should be passed into the stomach to remove it contents. In addition, a prokinetic agent and systemic antacid can be used during the perioperative period to decrease the risk of potential problems related to reflux of gastric contents. References 1. Morson BC, Dawson IMP, Day DW, et al. Morson & Dawson's Gastrointestinal Pathology, 3rd ed. Oxford: Blackwell Scientific, 1990, p. 77. 2. Guilford WG, Strombeck DR. In: Strombeck's Small Animal Gastroenterology, 3rd ed. Guilford WG, et al (ed). Philadelphia: WB Saunders, 1996, p. 239. - Available from amazon.com 3. Rees WDW, Brown CM. Physiology of the stomach and duodenum. In: Bockus Gastroenterology, 5th ed. Haubrich WS, Schaffner F, Berk JE (eds). Philadelphia: WB Saunders, 1995, p. 582. - Available from amazon.com 4. Twedt DC, Magne ML. Diseases of the stomach. In: Textbook of Veterinary Internal Medicine, 3rd ed. Ettinger SJ (ed). Philadelphia: WB Saunders, 1989, p. 1289. - Available from amazon.com 5. Stanton MLE. Gastric outlet obstruction. In: Disease Mechanisms in Small Animal Surgery, 2nd ed., Bojrab MJ, Smeak DD, Bloomberg MS (eds). Philadelphia: Lea & Febiger, 1993, p. 235. - Available from amazon.com 6. Sonnenberg A, Muller-Lissner SA, Schattenmann G, et al. Duodenogastric reflux in the dog. Am J Physiol 242:G603, 1982. - PubMed 7. Happe RP, Van Den Brom WE, Van Der Gaag I. Duodenogastric reflux in the dog, a clinicopathological study. Res Vet Sci 33:280, 1982. - PubMed 8. Cooperman AM. Postoperative alkaline reflux gastritis. Surg Clin North Am 56:1445, 1976. - PubMed 9. Bright RM, Jenkins C, DeNovo RC. Pyloric obstruction in a dog related to a gastrotomy incision closed with polypropylene. J Small Anim Pract 35:629, 1994. 10. Bright RM. Surgery of the stomach. In: Saunders Manual of Small Animal Practice, 2nd ed. Birchard SJ, Sherding RG (eds). Philadelphia: WB Saunders, 2000, p. 777. - Available from amazon.com 11. Dulisch ML. Pyloromyotomy, pyloroplasty, and pyloric resection. In: Current Techniques in Small Animal Surgery, 4th ed. Bojrab MJ, Ellison GW, Slocum B (eds). Baltimore: Williams & Wilkins, 1997, p. 207. - Available from amazon.com 12. Jenkins CC, DeNovo RC Jr. Diseases of the stomach. In: Handbook of Small Animal Practice, 4th ed. Morgan RV, Bright RM, Swartout MS (eds). Philadelphia: WB Saunders, 2003, p. 335. 5 13. Johnson SE, Sherding, RG, Bright RM. Diseases of the stomach. In: Saunders Manual of Small Animal Practice, 2nd ed. Birchard SJ, Sherding RG (eds). Philadelphia: WB Saunders, 2000, p. 753. - Available from amazon.com – ===================== 6