Hand Muscle Power Deficits ICD-9-CM codes: ICF codes: Activities
advertisement

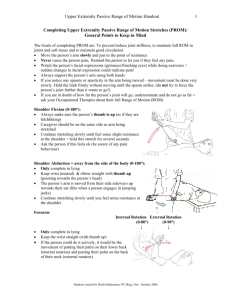
1 Hand Muscle Power Deficits ICD-9-CM codes: ICF codes: 727.03 Radial styloid tenosynovitis 727.04 Trigger digits Activities and Participation Domain codes: d4301 Carrying in the hands; d4400 Picking up; d4401 Grasping; d4452 Reaching; d4453 Turning or twisting the hands or arms Body Structure code: s73012 Muscles of forearm Body Functions code: b7300 Power of isolated muscles and muscle groups Common Historical Findings: Thumb abductors/extensors musculotendinous involvement: Pain in dorso-radial wrist that is most noticeable with pinching and wrist movements Onset associated w/repetitive thumb and wrist movements or trauma to the area (e.g., blow to lateral wrist) Finger flexors musculotendinous involvement: Pain, stiffness, and swelling of the volar surface of finger and palm Snapping or locking with attempted movement Common Impairment Findings - Related to the Reported Activity Limitation or Participation Restriction: Thumb abductors/extensors musculotendinous involvement: Symptoms reproduced with: Resisted APL and EPB tests (weak & painful) Stretch to APL/EPB tendons (Finklestein’s) Palpation/provocation of the APL and EPB tendons Finger flexors musculotendinous involvement: Symptoms reproduced with: Resisted FDP and FDS tests (weak and painful) Palpation/provocation of the FDP and/or FDS tendon Physical Examination Procedures: Manual Resistive Test Abductor Pollicis Longus Manual Resistive Test Extensor Pollicis Brevis Cues: Abduction of the thumb is a movement perpendicular to the palm-away from the palm Extension of the thumb is a movement parallel to the palm - away from the palm Cuong Pho DPT, Joe Godges DPT Loma Linda U DPT Program KPSoCal Ortho PT Residency 2 Provocation of APL and EPB Tendons Cues: If acute - gentle palpation reproduces symptoms If sub acute - stronger provocation may be required to reproduce the symptoms In normals - firm pressure is painfree Finkelstein’s Test Cues: Stretch of APL and EPB Instruct patient to grab thumb with fingers - then slowly ulnarly deviate the wrist (demonstrate motion to the patient) Perform test slowly to avoid further tissue injury and pain Cuong Pho DPT, Joe Godges DPT Loma Linda U DPT Program KPSoCal Ortho PT Residency 3 Wrist Mobility Deficits: Description, Etiology, Stages, and Intervention Strategies The below description is consistent with descriptions of clinical patterns associated with wrist Radial Styloid Tenosynovitis the vernacular term “DeQuervain’s Syndrome” Description: Pain, tenderness and swelling over the first dorsal compartment, increased with thumb and/or wrist motions. Pain is worse with passive stretch into wrist ulnar deviation with the thumb held in neutral (Finklestein’s test) or repetitive active thumb abduction and extension. The aggravating stress is greatest when radial deviation is combined with a gripping motion of the thumb because of the angulation of the tendons causes tearing stress to the extensor retinaculum. Pain may radiate either proximally or distally toward the thumb or elbow. There may be decreased abduction range in the carpometacarpal joint of the thumb, and palpable thickening of the extensor sheath and the tendons distal to the extensor tunnel. Etiology: A stenosing tenosynovitis of the first dorsal compartment. The compartment is approximately 1 in. in length and is formed by the osseous groove in the radial styloid and the overlying extensor retinaculum. This first dorsal compartment houses the tendons of abductor pollicis longus (APL) and extensor pollicis brevis (EPB). It usually affects women between the ages of 30 and 60 years old, and those who participate in wheelchair sports. It is most common in repetitive activities such as keyboarding, filing, carpentry, assembly-line work, and golfing. It may also occur transiently during pregnancy and breast feeding. Acute Stage / Severe Condition: Physical Examinations Findings (Key Impairments) ICF Body Functions code: b7101.3 SEVERE impairment of mobility of several joints • • • • • • Palpable crepitus is occasionally present moving through the extensor sheath Symptoms reproduced with provocatory pressure over the first compartment Triggering of thumb may imply excessive stenosis or a nodule formation on APL or EPB Weakness in the wrist radial deviation, EPB, APL Tenderness is usually felt in the “anatomical snuff box” along radial side of wrist with palpation. Pain can radiate distally into thumb/hand, and proximally to elbow. Pain may limit thumb active extension and abduction Sub Acute Stage / Moderate Condition: Physical Examinations Findings (Key Impairments) ICF Body Functions code: b7101.2 MODERATE impairment of mobility of several joints As above – but with the following differences • The movement limitations are decreased • Strength deficits are less • Provocatory pain is less intense, and provoked closer to end range of motion Settled Stage / Mild Condition: Physical Examinations Findings (Key Impairments) ICF Body Functions code: b7101.1 MILD impairment of mobility of several joints As above – but with the following differences • Movement limitations are less • Strength deficits are minimal • The provocatory pain is elicited primarily with overpressure at end range Cuong Pho DPT, Joe Godges DPT Loma Linda U DPT Program KPSoCal Ortho PT Residency 4 Intervention Approaches / Strategies Acute Stage / Severe Condition: Goals: Control pain and symptoms, and decrease inflammation • Physical Agents Ultrasound or phonporesis to aid reduction of inflammation over the first dorsal compartment Iontophoresis may also be used to aid reduction of inflammation • External Devices (Taping/Splinting/Orthotics) A thumb spica short-arm splint may help position the wrist and decrease the use and irritation of the first dorsal compartment • Manual Therapy Soft tissue mobilization to restricted myofascial tissue (e.g, extensor retinaculum, APL, and EPB) that may be causing restriction, or in muscle spasms Mobilizations with movement (MWM) of active movements of the thumb and wrist superimposed on a passive radial glide of the proximal row of carpal bones • Therapeutic Exercise Gentle passive range of motion of thumb and wrist • Medications Anti-inflammatory medications (NSAIDS), and pain relievers. After 2 weeks if unsuccessful at pain relief, corticosteroid injections. • Ergonomic Instruction Modify or avoid aggravating activities during work or recreational environments, postures and tasks (e.g., hand/wrist position while filing, golfing, or doing assembly line work) Sub Acute Stage / Moderate Condition Goals: Restore normal and pain free range of motion As above with the following differences: Inflammation is controlled, so mobilization phase begins. • • • More aggressive with repetitive activities of the thumb especially at end range Progressive resistive exercise begin when 80-85 % of painless range of motion is attained Less use of modalities for treatment, and only for post exercise pain, and inflammation management Cuong Pho DPT, Joe Godges DPT Loma Linda U DPT Program KPSoCal Ortho PT Residency 5 Settled Stage / Mild Condition Goals: Maintain or return to functional activities of the wrist and hand • • Correct any biomechanical deficits that may occur during functional activity Therapeutic Exercise: Increase progressive resistive exercises and functional strengthening exercises as tolerated Intervention for High Performance / High Demand Functioning in Workers or Athletes Goals: Return to optimum level of function for work and leisure time activities, and reduce likelihood of re-injury while attaining previous level of function. (usually within 1 month) Approaches / Strategies listed above • • Work on endurance training and work hardening for specific occupation or sport activity Gripping activities should be painless Cuong Pho DPT, Joe Godges DPT Loma Linda U DPT Program KPSoCal Ortho PT Residency 6 Selected References Alberton G, et al. Extensor Triggering in de Quervain’s Stenosing Tenosynovitis. J Hand Surg. 1999;24A(6)1311-1314. Anderson B, et al. Treatment of De Quervain’s Tenosynovitis With Corticosteroids. Arthritis and Rheumatism. 1991;34(7)793-798. Anderson M, et al. A Patient With De Quervain’s Tenosynovitis: A Case Report Using an Australian Approach to Manual Therapy. Phys Ther. 1994;74(4):314-326. Apple DF, at. al. Overuse Syndrome of the Upper Limb in People with Spinal Cord Injury. Department of Veterans Affairs. 1996;5:97-107. Backstrom K. Mobilization With Movement as an Adjunct Intervention in a Patient With Complicated De Quervain'’ Tenosynovitis: A Case Report. J Ortho Sports Phys Ther. 2002;32(3):86-94. Cooney WP. The Wrist Diagnosis, and Operative Treatment. vol. 2 Mosby, St. Louis, 1998. Johnson CA. Occurrence of de Quervain’s Disease in Postpartum Women. J Family Practice. 1991;32(3):325-327. Kent T, et al. Patient Satisfaction and Outcomes of Surgery for de Quervain’s Tenosynovitis. J Hand Surg. 1999;24A(5):1071-1077. Lichtman DM. The Wrist and Its Disorders. W.B. Saunders Company, Philadelphia, 1988. More S. De Quervain’s Tenosynovitis. American College of Occupational and Environmental Medicine. 1997;39(10):990-1002. Piligian G, et all. Evaluation and Management of Chronic Work-Related Musculoskeletal Disorders of the Distal Upper Extremity. American Journal of Industrial Medicine. 2000;37:7593. Schned E. DeQuervain Tenosynovitis in Pregnant and Postpartum Women. Obstetrics & Gynecology. 1986;68(3):411-114. Sinan A, et al. Comparison of Nonsurgical Treatment Measures for de Quervain’s Disease of Pregnancy and Lactation. J Hand Surg. 2002;27(2):322-324. Zingas C, et al. Injectin Accuracy and Clinical Relief of De Quervain’s Tendinitis. J Hand Surg. 1998;23A(1):89-96. Cuong Pho DPT, Joe Godges DPT Loma Linda U DPT Program KPSoCal Ortho PT Residency