Antivirals and Respiratory Outbreaks
advertisement

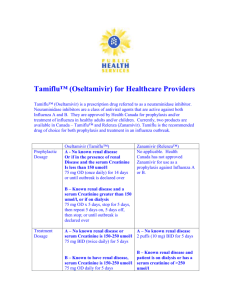
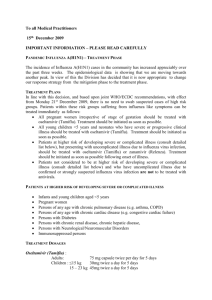
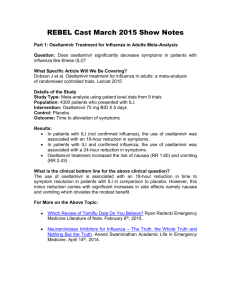
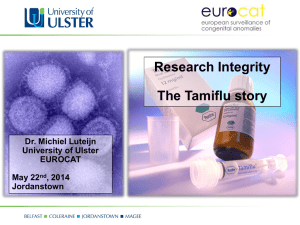
Antivirals and Respiratory Outbreaks Allison McGeer, MSc, MD, FRCPC Mount Sinai Hospital University of Toronto www.microbiology.mtsinai.on.ca Disclosures My research group receives/has received funding for investigator initiated research, and via sponsored clinical trials, participation on data safety monitoring boards and honoraria for lectures and advisory board participation, from the following companies with products related to influenza diagnosis, management and prevention: Adamas Pharmaceuticals Astra-Zeneca Biocryst Copan Diagnostics Gilead Biosciences GlaxoSmithKline Hoffman LaRoche Luminex Technologies Medicago Medonyx Novartis Sanofi-Pasteur Solvay Biologics Influenza in Ontario LTCFs 1990-1997 Season 90/91 91/92 92/93 93/94 94/95 95/96 96/97 97/98 No. outbreaks Attack rate (mean, range) % cases with pneumonia (mean, range) Case fatality rate (mean, range) Vaccine efficacy (mean) 8 21 20 32 39 13 94 155 15% (3-46) 34% (13-73) 26% (4-55) 33% (5-74) 27% (3-100) 38% (12-100) 27% (1-74) 11% (0-37) 12% (0-56) 7% (0-47) 2% (0-12) 5% (0-90) 14% (0-50) 11% (0-65) 3% (0-17) 5% (0-12) 5% (0-49) 38% 20% 23% 42% Questions about antivirals • What antiviral? • Which residents need treatment/prophylaxis and when? When should dose adjustment for reduced creatinine clearance be considered? Which staff should receive prophylaxis? When can prophylaxis be discontinued? What response is appropriate if cases continue to occur despite prophylaxis? Neuraminidase inhibitors (oseltamivir; zanamivir) M2 inhibitors (amantadine) Antivirals: Amantadine, oseltamivir, zanamivir FOR SUSCEPTIBLE STRAINS – Prophylaxis, all 65-80% effective No head-to-head comparisons, but no differences apparent – Treatment No data to suggest that their effectiveness is different More data for oseltamivir than zanamivir than amantadine Amantadine - limitations Not effective against influenza B Currently, both A(H3N2) and A(H1N1) are resistant Very limited data on effectiveness of treatment Rapid emergence of resistance on treatment 8-12% rate of CNS side effects (20% of patients report some CNS side effect) Relatively low toxic/therapeutic ratio Zanamivir All influenza isolate strains susceptible – Lower selection for resistance on therapy Not absorbed – No systemic adverse events – ?less effective in severe disease Difficult to deliver to demented, frail elderly Characteristics of residents associated with difficulty performing inhalations No (%) with difficulty P value Activities of daily living: <.001 Mostly independent 2/24 (8%) Largely dependent 12/76 (16%) Completely dependent 15/26 (58%) Oriented <.001 To person/place/time 1/33 (3%) Two of three 2/19 (11%) One of three 4/25 (16%) Not oriented 22/49 (45%) Amount of zanamivir delivered to residents Oseltamivir Capsule or suspension Very high toxic to therapeutic ratio Day 1 Day 5 Dutkowski et al. International Journal of Antimicrobial Agents ; 2010:35: 461-467 Adverse effects associated with high dose Adverse event Placebo Oseltamivir (bid) 75mg 225mg 450mg Headache 20% 17% 24% 23% Nausea 8% 8% 26% 31% Vomiting 2% 3% 7% 16% Dizziness 4% 2% 11% 10% Dutkowski et al. International Journal of Antimicrobial Agents ; 2010:35: 461-467 Oseltamivir Capsule or suspension Very high toxic to therapeutic ratio Selection for resistance occurs – Usually H275Y (but others described) – Usually, virus is not fully virulent Antiviral resistance Not driven by antiviral use – Influenza viruses “balance” mutations – Single viral clade becomes successful each year If the patient does not have influenza, NO selective pressure Prophylaxis is less selective than treatment – BUT post-exposure prophylaxis MAY be pre-emptive treatment Residents Meet case definition – Treatment doses x 5 days UNLESS case is lab-confirmed, and clearly improving Ill (possibly related), but do not meet case definition – Treatment doses x 5 days Ill, but have recovered – Lab-confirmed influenza – NO prophylaxis – Lab testing negative/not done: Prophylaxis How long do you write prophylaxis scripts for? Too short, and you need repeat orders and repeat prescriptions for all residents Too long, and you waste drug (and money) Making a recommendation for initial prescriptions 14 day standard (IDSA recommendations) How many cases in the outbreak so far? What is the history of influenza outbreaks in this home? In your public health unit? How much activity is there due to other viruses? How big is the nursing home/unit? Oseltamivir compassionate use program, Ontario, 2000 (outbreak B8) Number of new cases 12 Neg/not tested Flu A positive 10 Oseltamivir start 8 6 4 2 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 Outbreak Day Number Number of new cases Oseltamivir compassionate use program, Ontario, 2000 (outbreak B4) Oseltamivir start 8 7 6 5 4 3 2 1 0 1 2 3 Bowles, JAGS 2002 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 Outbreak Day Number Dose reduction in renal failure Penicillin: patients with impaired renal function (<30ml/min) require modification of dose and interval Oseltamivir: for patients with a creatinine clearance <30ml/min, it is recommended that the dose is reduced to 75 mg od Scatter plot of baseline creatinine clearance results by age in LTCF residents (BCCDC) Creatinine Clearance 140 120 100 80 60 40 20 0 20 40 60 Age (years) 80 100 120 Oseltamivir and renal failure For creatinine clearance above 10ml/min, 75 mg od is safe Creatinine clearance of 10ml/min is equivalent to serum creatinine of about 250 umol/L (85 year old, 40kg) What about staff? Strongly recommend that staff who choose to be unimmunized acquire a prescription that can be filled later – Consider providing letter to health care providers Consider offering a choice of active antivirals Don’t worry about prophylaxis of immunized staff unless: (i) there is clearly defined lack of protection OR (ii) there is lab-confirmed illness in multiple vaccinated staff Oseltamivir Capsule or suspension Very high toxic to therapeutic ratio Day 1 Day 5 Dutkowski et al. International Journal of Antimicrobial Agents ; 2010:35: 461-467 Staff categories Not exposed – Minimum incubation period 12-18 hours – as long as have started oseltamivir, will be protected Exposed and incubating infection – Already shedding virus, or about to be shedding virus – and at 4 hours, will still be shedding virus – May develop symptoms at any time during next 24-48 hours Effect of Oral Oseltamivir Treatment on Vital Titers in Nasal Lavages Following Experimental Influenza A/Texas/36/91(H1N1) Infection The viral titer area under the curve value was lower in the combined oseltamivir group (n=56) compared with placebo (n=13); P=.02 Hayden, F. G. et al. JAMA 1999;282:1240-1246. Questions?