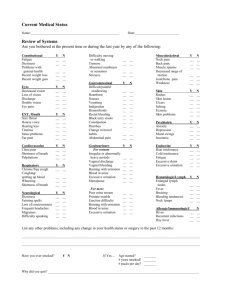
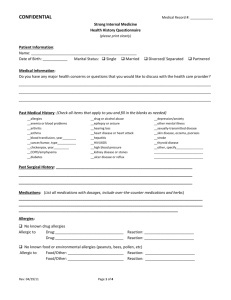
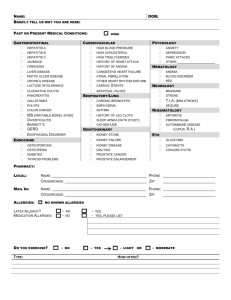
patient health questionnaire
advertisement

MRN: Patient Name: PATIENT HEALTH QUESTIONNAIRE Radiation Oncology (Patient Label) REVIEWED DATE / INITIALS SAFETY: Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? YES NO ALLERGIES: YES Do you have medications? any allergies to NO If YES, please list medication allergies: Are you allergic to iodine/IV contrast dye? ___________________________________________________________________________________ PERTINENT HISTORY Medical History (please list past and current conditions): Medical Problems Surgeries Do you have any of the specific medical conditions listed below: YES NO Inflammatory Bowel Disease Crohn’s Disease Ulcerative Colitis Lupus Scleroderma Claustrophobia UCLA Form #500704 Rev. (01/12) Page 1 of 5 MRN: Patient Name: PATIENT HEALTH QUESTIONNAIRE Radiation Oncology (Patient Label) Have you ever had: YES NO Previous Radiotherapy Previous Chemotherapy GYNECOLOGICAL (female patients only): Number of pregnancies: Number of children: Age at first live birth: Age periods first started: Age at menopause (if postmenopausal): Menopause Status: Have you ever taken oral contraceptives or hormone replacement medication? If yes, what type: YES NO Date of last Pap Smear: Date of last Mammogram: Premenopausal Postmenopausal Don’t know FAMILY HISTORY YES Have any of your family members ever had cancer? If yes, please list relationship and type of cancer in your family member(s): NO SOCIAL HISTORY: Smoking YES NO If you smoke currently or have smoked in the past: Number years smoked Number packs per day Number years quit YES NO If you drink alcohol currently or have done so in the past: Number days drink/week Number drinks/day Never smoked Smoke currently Smoked previously Alcohol Never drink alcohol Occasionally drink alcohol Frequently drink alcohol UCLA Form #500704 Rev. (01/12) Number years quit Page 2 of 5 MRN: Patient Name: PATIENT HEALTH QUESTIONNAIRE Radiation Oncology (Patient Label) Employement: Are you employed? NO If yes, what is your occupation: YES YES Support Systems: Do you live alone? Do you live with your spouse, significant other, family or friends? Do you live in your own house/appartment? Do you live in a nursing home? Do you live in an assisted living environment? Other comments: Transportation: Would transportation to UCLA for daily treatments be difficult for you? If Yes, please explain: YES NO NO System Review: Please check “yes” or “no” box to indicate if you have any of the following YES Immunology/Allergy Allergies to animals or plants Reactions (Runny Nose or itchy eyes) Cardiovascular Irregular heart beat (arrythmias) Chest Pain Difficulty walking two blocks (dyspnea) Swelling of hands, feet or ankles (edema) Shortness of breath while walking or lying down (orthopnea) Heart Murmur (palpitations) UCLA Form #500704 Rev. (01/12) NO YES NO Genitourinary (Female) Burning or painful urination Frequent urination Blood in urine Incontinence Frequent night time urination Kidney / bladder stones Sexual difficulty Urgency with urination Urine color change Vaginal discharge/bleeding Vaginal spotting Page 3 of 5 MRN: Patient Name: PATIENT HEALTH QUESTIONNAIRE Radiation Oncology (Patient Label) System Review (Continued): Please check “yes” or “no” box to indicate if you have any of the following YES Constitutional Poor appetite Fatigue Fevers Lethargy (sluggisness, sleepiness) Malaise (uneasiness) Night Sweats Chills Recent Weight Change: Gain Loss If yes, amount: _________lbs Endocrine Hot flashes Menstrual irregularities Intolerance to hot/cold (thyroid disease) Ears, Nose & Throat Pain swallowing / Sore throat (dysphagia) Ear pain Nose bleeding (epistaxis) Change in hearing ability Mouth dryness Oral bleeding Ear infection (otitis) Sinus infection (sinusitis) Excessive sputum production Taste changes Ear ringing Voice change Eyes Blurred vision Double vision Excessive tearing (lacrimation) Night blindness Excessive light sensitivity (photophobia) Other visual difficulties / changes in vision UCLA Form #500704 Rev. (01/12) NO YES NO Genitourinary (Male) Burning or painful urination Frequent urination Blood in urine Impotence Incontinence Frequent night time urination Kidney / bladder stones Scrotal/testicular swelling Urgency with urination Urine color change Hematologic Abnormal bruising or bleeding Swollen glands (lymph nodes) Skin Blisters Abnormal itching (pruritus) Rash Musculoskeletal Inflammation of joints (arthritis) Bone Pain Joint Pain Muscle weakness Range of motion problems Psychiatric Depression Anxiety Respiratory Cough Blood in sputum (hemoptysis) Page 4 of 5 MRN: Patient Name: PATIENT HEALTH QUESTIONNAIRE Radiation Oncology (Patient Label) System Review (Continued): Please check “yes” or “no” box to indicate if you have any of the following YES Gastrointestinal Abdominal pain Recent change in bowel habits Constipation Frequent diarrhea Heartburn or indigestion Fresh blood in stools Hemorrhoids Black stools Nausea Vomiting NO YES NO Neurological Disorientation Dizziness Gait problems Headaches Insomnia Memory loss Motor weakness Paralysis Convulsions (seizures) Sensory problems Stroke Patient Signature: ____________________________________ Date: _____________ Time: ________ If completed by an individual other than the patient, please state relationship to the patient: __________ ___________________________________________________________________________________ This Past Medical History, Family History, Social History, and Review of Symptoms have been reviewed with the patient, by the physician(s) noted below: Resident Signature: __________________________________ Date: _____________ Time: ________ Attending Signature: __________________________________ Date: _____________ Time: ________ UCLA Form #500704 Rev. (01/12) Page 5 of 5